強迫性障害
Obsessive–compulsive disorder, OCD
☆ 強迫性障害(OCD)とは、侵入的な考え(強迫観念)を持ち、その強迫観念によって引き起こされる苦痛を和らげるために、一般的な機能を損なうほど特定のルーチン(強迫)を繰り返し行う必要性を感じる精神・行動障害である。強迫観念とは、不安、嫌悪、または不快の感情を生じさせる持続的な不要な考え、心的イメージ、または衝動のことである。一般的な強迫観念には、汚染 への恐怖、左右対称性への強迫、冒涜的な行動への恐怖、患者の性的指向、他者または自分自身を傷つけるかもしれないという恐怖などがある。強 迫観念とは、強迫観念に反応して、不安からの解放を達成するために起こる反復的な行動またはルーチンのことである。一般的な強迫観念には、過剰な手洗い、 掃除、数を数える、命令する、繰り返す、誘因を避ける、ため込む、中和する、保証を求める、祈る、物を確認するなどがある。
| Obsessive–compulsive disorder (OCD)
is a mental and behavioral disorder in which an individual has
intrusive thoughts (an obsession) and feels the need to perform certain
routines (compulsions) repeatedly to relieve the distress caused by the
obsession, to the extent where it impairs general function.[1][2][7] Obsessions are persistent unwanted thoughts, mental images, or urges that generate feelings of anxiety, disgust, or discomfort.[8] Some common obsessions include fear of contamination, obsession with symmetry, the fear of acting blasphemously, the sufferer's sexual orientation, and the fear of possibly harming others or themselves.[1][9] Compulsions are repeated actions or routines that occur in response to obsessions to achieve a relief from anxiety. Common compulsions include excessive hand washing, cleaning, counting, ordering, repeating, avoiding triggers, hoarding, neutralizing, seeking assurance, praying, and checking things.[1][9][10] People with OCD may only perform mental compulsions such as needing to know or remember things. While this is sometimes referred to as primarily obsessional obsessive–compulsive disorder (Pure O), it is also considered a misnomer due to associated mental compulsions and reassurance seeking behaviors that are consistent with OCD.[11] Compulsions occur often and typically take up at least one hour per day, impairing one's quality of life.[1][9] Compulsions cause relief in the moment, but cause obsessions to grow over time due to the repeated reward-seeking behavior of completing the ritual for relief. Many adults with OCD are aware that their compulsions do not make sense, but they still perform them to relieve the distress caused by obsessions.[1][8][9][12] For this reason, thoughts and behaviors in OCD are usually considered egodystonic. In contrast, thoughts and behaviors in obsessive-compulsive personality disorder (OCPD) are usually considered egosyntonic, helping differentiate between the two.[13] Although the exact cause of OCD is unknown, several regions of the brain have been implicated in its neuroanatomical model including the anterior cingulate cortex, orbitofrontal cortex, amygdala, and BNST.[14][1] The presence of a genetic component is evidenced by the increased likelihood for both identical twins to be affected than both fraternal twins.[15] Risk factors include a history of child abuse or other stress-inducing events such as during the postpartum period or after streptococcal infections.[1][16] Diagnosis is based on clinical presentation and requires ruling out other drug-related or medical causes; rating scales such as the Yale–Brown Obsessive–Compulsive Scale (Y-BOCS) assess severity.[2][17] Other disorders with similar symptoms include generalized anxiety disorder, major depressive disorder, eating disorders, tic disorders, body-focused repetitive behavior, and obsessive–compulsive personality disorder.[2] Personality disorders are a common comorbidity, with schizotypal and OCPD having poor treatment response.[13] The condition is also associated with a general increase in suicidality.[3][18][19] The phrase obsessive–compulsive is sometimes used in an informal manner unrelated to OCD to describe someone as excessively meticulous, perfectionistic, absorbed, or otherwise fixated.[20] However, the actual disorder can vary in presentation, and individuals with OCD may not be concerned with cleanliness or symmetry. OCD is chronic and long-lasting with periods of severe symptoms followed by periods of improvement.[21][22] Treatment can improve ability to function and quality of life, and is usually reflected by improved Y-BOCS scores.[23] Treatment for OCD may involve psychotherapy, pharmacotherapy such as antidepressants, or surgical procedures such as deep brain stimulation or, in extreme cases, psychosurgery.[4][5][24][25] Psychotherapies derived from cognitive behavioral therapy (CBT) models, such as exposure and response prevention, acceptance and commitment therapy, and inference based-therapy, are more effective than non-CBT interventions.[26] SSRIs are more effective when used in excess of the recommended depression dosage; however, higher doses can increase side effect intensity.[27] Commonly used SSRIs include sertraline, fluoxetine, fluvoxamine, paroxetine, citalopram, and escitalopram.[24] Some patients fail to improve after taking the maximum tolerated dose of multiple SSRIs for at least two months; these cases qualify as treatment-resistant and can require second-line treatment such as clomipramine or atypical antipsychotic augmentation.[4][5][27][28] While SSRIs continue to be first-line, recent data for treatment-resistant OCD supports adjunctive use of neuroleptic medications, deep-brain stimulation, and neurosurgical ablation.[29] There is growing evidence to support the use of deep brain stimulation and repetitive transcranial magnetic stimulation for treatment-resistant obsessive-compulsive disorder.[30][31] Obsessive–compulsive disorder affects about 2.3% of people at some point in their lives, while rates during any given year are about 1.2%.[2][6] More than three million Americans suffer from OCD.[32] According to Mercy, approximately 1 in 40 U.S. adults and 1 in 100 U.S. children have OCD.[33] Although possible at times with triggers such as pregnancy, onset rarely occurs after age 35, and about 50% of patients experience detrimental effects to daily life before age 20.[1][16][2][34] While OCD occurs worldwide,[1][2] a recent meta-analysis showed that women are 1.6 times more likely to experience OCD.[35] Based on data from 34 studies, the worldwide prevalence rate is 1.5% in women and 1% in men.[35] |
強迫性障害(OCD)とは、侵入的な考え(強迫観念)を持ち、その強迫観念によって引き起こされる苦痛を和らげるために、一般的な機能を損なうほど特定のルーチン(強迫)を繰り返し行う必要性を感じる精神・行動障害である[1][2][7]。 強迫観念とは、不安、嫌悪、または不快の感情を生じさせる持続的な不要な考え、心的イメージ、または衝動のことである[8]。一般的な強迫観念には、汚染 への恐怖、左右対称性への強迫、冒涜的な行動への恐怖、患者の性的指向、他者または自分自身を傷つけるかもしれないという恐怖などがある[1][9]。強 迫観念とは、強迫観念に反応して、不安からの解放を達成するために起こる反復的な行動またはルーチンのことである。一般的な強迫観念には、過剰な手洗い、 掃除、数を数える、命令する、繰り返す、誘因を避ける、ため込む、中和する、保証を求める、祈る、物を確認するなどがある[1][9][10]。これは主 に強迫性強迫性障害(Pure O)と呼ばれることもあるが、OCDと一致する関連した精神的強迫や安心を求める行動のため、誤用とも考えられている[11]。 強迫観念は頻繁に起こり、典型的には1日に少なくとも1時間を占め、生活の質を損なう[1][9]。強迫観念はその場では安心感をもたらすが、安心感を得 るために儀式を完了させるという報酬を求める行動を繰り返すため、強迫観念は時間とともに大きくなる。OCDの成人の多くは、強迫観念が意味をなさないこ とを自覚しているが、それでも強迫観念による苦痛を和らげるために強迫観念を行っている。これとは対照的に、強迫性パーソナリティ障害(OCPD)の思考 や行動は通常、自我統 合的であると考えられ、両者を区別するのに役立っている[13]。 OCDの正確な原因は不明であるが、前帯状皮質、眼窩前頭皮質、扁桃体、BNSTなど、脳のいくつかの領域が神経解剖学的モデルに関与していることが示唆 されている[14][1]。遺伝的要素の存在は、一卵性双生児が二卵性双生児よりも罹患する可能性が高いことからも明らかである。 [15] 危険因子には、児童虐待の既往歴、または産褥期や溶連菌感染後などの他のストレス誘発性事象が含まれる。 [1] [16] 診断は臨床症状に基づいて行われ、他の薬物関連または医学的原因を除外する必要がある;Yale-Brown Obsessive-Compulsive Scale(Y-BOCS)などの評価尺度で重症度を評価する。 [2] [17] 類似の症状を示す他の疾患には、全般性不安障害、大うつ病性障害、摂食障害、チック障害、身体焦点反復行動、強迫性パーソナリティ障害などがある[2]。 パーソナリティ障害は一般的に併存症であり、統合失調型およびOCPDは治療効果が低い。 [13]また、この疾患は自殺傾向の一般的な増加とも関連している。 18][19] 強迫性強迫性という言葉は、OCDとは無関係に、過度に几帳面で、完璧主義的で、のめり込んでいる、あるいは他のことにこだわっている人を表現するため に、非公式に使われることがある。 OCDは慢性的で長く続き、症状が重くなる時期と改善する時期を繰り返す [21] [22] 治療によって機能的な能力や生活の質を改善することができ、通常Y-BOCSスコアの改善によって反映される [23] 。 [4][5][24][25]認知行動療法(CBT)モデルから派生した心理療法、例えば暴露反応妨害療法、受容とコミットメント療法、推論に基づく療法 などは、非CBT介入よりも効果的である[26]。 SSRIは推奨されるうつ病の用量を超えて使用するとより効果的であるが、用量を増やすと副作用が強くなる。 [27] 一般的に使用されるSSRIには、セルトラリン、フルオキセチン、フルボキサミン、パロキセチン、シタロプラム、エスシタロプラムなどがある[24]。少 なくとも2ヵ月間、複数のSSRIの最大耐容量を服用しても改善しない患者もいる;このような症例は治療抵抗性と認定され、クロミプラミンや非定型抗精神 病薬の増強などの第2選択治療が必要となる。 [4][5][27][28]。SSRIが第一選択薬であることに変わりはないが、治療抵抗性強迫性障害に対する最近のデータでは、神経遮断薬、脳深部刺 激療法、神経外科的焼灼術の併用が支持されている[29]。治療抵抗性強迫性障害に対する脳深部刺激療法や反復経頭蓋磁気刺激の使用を支持するエビデンス が増えている[30][31]。 強迫性障害は人生のある時点で約2.3%の人が罹患し、ある年の罹患率は約1.2%である[2][6]。 300万人以上のアメリカ人が強迫性障害に苦しんでいる[32]。マーシーによると、アメリカの成人の約40人に1人、アメリカの子供の約100人に1人 が強迫性障害である。 [33]妊娠などのきっかけで発症することもあるが、35歳以降に発症することは稀であり、患者の約50%が20歳までに日常生活に有害な影響を経験して いる[1][16][2][34]。OCDは世界中で発症しているが[1][2]、最近のメタアナリシスでは、女性の方がOCDを経験する可能性が1.6 倍高いことが示されている[35]。34の研究のデータに基づくと、世界的な有病率は女性で1.5%、男性で1%である[35]。 |
| Signs and symptoms OCD can present with a wide variety of symptoms. Certain groups of symptoms usually occur together as dimensions or clusters, which may reflect an underlying process. The standard assessment tool for OCD, the Yale–Brown Obsessive Compulsive Scale (Y-BOCS), has 13 predefined categories of symptoms. These symptoms fit into three to five groupings.[36] A meta-analytic review of symptom structures found a four-factor grouping structure to be most reliable: symmetry factor, forbidden thoughts factor, cleaning factor, and hoarding factor. The symmetry factor correlates highly with obsessions related to ordering, counting, and symmetry, as well as repeating compulsions. The forbidden thoughts factor correlates highly with intrusive thoughts of a violent, religious, or sexual nature. The cleaning factor correlates highly with obsessions about contamination and compulsions related to cleaning. The hoarding factor only involves hoarding-related obsessions and compulsions, and was identified as being distinct from other symptom groupings.[37] When looking into the onset of OCD, one study suggests that there are differences in the age of onset between males and females, with the average age of onset of OCD being 9.6 for male children and 11.0 for female children.[38]Children with OCD often have other mental disorders, such as ADHD, depression, anxiety, and disruptive behavior disorder. Continually, children are more likely to struggle in school and experience difficulties in social situations (Lack 2012).When looking at both adults and children a study found the average ages of onset to be 21 and 24 for males and females respectively.[39] While some studies have shown that OCD with earlier onset is associated with greater severity, other studies have not been able to validate this finding.[40] Looking at women specifically, a different study suggested that 62% of participants found that their symptoms worsened at a premenstrual age. Across the board, all demographics and studies showed a mean age of onset of less than 25.[41] Some OCD subtypes have been associated with improvement in performance on certain tasks, such as pattern recognition (washing subtype) and spatial working memory (obsessive thought subtype). Subgroups have also been distinguished by neuroimaging findings and treatment response, though neuroimaging studies have not been comprehensive enough to draw conclusions. Subtype-dependent treatment response has been studied, and the hoarding subtype has consistently been least responsive to treatment.[42] While OCD is considered a homogeneous disorder from a neuropsychological perspective, many of the symptoms may be the result of comorbid disorders. For example, adults with OCD have exhibited more symptoms of attention–deficit/hyperactivity disorder (ADHD) and autism spectrum disorder (ASD) than adults without OCD.[43] In regards to the cause of onset, researchers asked participants in one study[41] what they felt was responsible for triggering the initial onset of their illness. 29% of patients answered that there was an environmental factor in their life that did so. Specifically, the majority of participants who answered with that noted their environmental factor to be related to an increased responsibility. Obsessions Main article: Intrusive thought See also: Primarily obsessional obsessive compulsive disorder Obsessions are stress-inducing thoughts that recur and persist, despite efforts to ignore or confront them.[44] People with OCD frequently perform tasks, or compulsions, to seek relief from obsession-related anxiety. Within and among individuals, initial obsessions vary in clarity and vividness. A relatively vague obsession could involve a general sense of disarray or tension, accompanied by a belief that life cannot proceed as normal while the imbalance remains. A more intense obsession could be a preoccupation with the thought or image of a close family member or friend dying, or intrusive thoughts related to relationship rightness.[45][46] Other obsessions concern the possibility that someone or something other than oneself—such as God, the devil, or disease—will harm either the patient or the people or things the patient cares about. Others with OCD may experience the sensation of invisible protrusions emanating from their bodies, or feel that inanimate objects are ensouled.[47] Another common obsession is scrupulosity, the pathological guilt/anxiety about moral or religious issues. In scrupulosity, a person's obsessions focus on moral or religious fears, such as the fear of being an evil person or the fear of divine retribution for sin.[48][49] Mysophobia, a pathological fear of contamination and germs, is another common obsession theme.[50][51] Some people with OCD experience sexual obsessions that may involve intrusive thoughts or images of "kissing, touching, fondling, oral sex, anal sex, intercourse, incest, and rape" with "strangers, acquaintances, parents, children, family members, friends, coworkers, animals, and religious figures", and can include heterosexual or homosexual contact with people of any age.[52] Similar to other intrusive thoughts or images, some disquieting sexual thoughts are normal at times, but people with OCD may attach extraordinary significance to such thoughts. For example, obsessive fears about sexual orientation can appear to the affected individual, and even to those around them, as a crisis of sexual identity.[53][54] Furthermore, the doubt that accompanies OCD leads to uncertainty regarding whether one might act on the troubling thoughts, resulting in self-criticism or self-loathing.[52] Most people with OCD understand that their thoughts do not correspond with reality; however, they feel that they must act as though these ideas are correct or realistic. For example, someone who engages in compulsive hoarding might be inclined to treat inorganic matter as if it had the sentience or rights of living organisms, despite accepting that such behavior is irrational on an intellectual level. There is debate as to whether hoarding should be considered an independent syndrome from OCD.[55] Compulsions Main article: Compulsive behavior Some people with OCD perform compulsive rituals because they inexplicably feel that they must do so, while others act compulsively to mitigate the anxiety that stems from obsessive thoughts. The affected individual might feel that these actions will either prevent a dreaded event from occurring, or push the event from their thoughts. In any case, their reasoning is so idiosyncratic or distorted that it results in significant distress, either personally, or for those around the affected individual. Excessive skin picking, hair pulling, nail biting, and other body-focused repetitive behavior disorders are all on the obsessive–compulsive spectrum.[2] Some individuals with OCD are aware that their behaviors are not rational, but they feel compelled to follow through with them to fend off feelings of panic or dread.[56] Furthermore, compulsions often stem from memory distrust, a symptom of OCD characterized by insecurity in one's skills in perception, attention, and memory, even in cases where there is no clear evidence of a deficit.[57] Common compulsions may include hand washing, cleaning, checking things (such as locks on doors), repeating actions (such as repeatedly turning on and off switches), ordering items in a certain way, and requesting reassurance.[58][59] Although some individuals perform actions repeatedly, they do not necessarily perform these actions compulsively; for example, morning or nighttime routines and religious practices are not usually compulsions. Whether behaviors qualify as compulsions or mere habit depends on the context in which they are performed. For instance, arranging and ordering books for eight hours a day would be expected of someone who works in a library, but this routine would seem abnormal in other situations. In other words, habits tend to bring efficiency to one's life, while compulsions tend to disrupt it.[60] Furthermore, compulsions are different from tics (such as touching, tapping, rubbing, or blinking) and stereotyped movements (such as head banging, body rocking, or self-biting), which are usually not as complex and not precipitated by obsessions.[61] It can sometimes be difficult to tell the difference between compulsions and complex tics, and about 10–40% of people with OCD also have a lifetime tic disorder.[2][62] People with OCD rely on compulsions as an escape from their obsessive thoughts; however, they are aware that relief is only temporary, and that intrusive thoughts will return. Some affected individuals use compulsions to avoid situations that may trigger obsessions. Compulsions may be actions directly related to the obsession, such as someone obsessed with contamination compulsively washing their hands, but they can be unrelated as well.[9] In addition to experiencing the anxiety and fear that typically accompanies OCD, affected individuals may spend hours performing compulsions every day. In such situations, it can become difficult for the person to fulfill their work, familial, or social roles. These behaviors can also cause adverse physical symptoms; for example, people who obsessively wash their hands with antibacterial soap and hot water can make their skin red and raw with dermatitis.[63] Individuals with OCD often use rationalizations to explain their behavior; however, these rationalizations do not apply to the behavioral pattern, but to each individual occurrence. For example, someone compulsively checking the front door may argue that the time and stress associated with one check is less than the time and stress associated with being robbed, and checking is consequently the better option. This reasoning often occurs in a cyclical manner, and can continue for as long as the affected person needs it to in order to feel safe.[64] In cognitive behavioral therapy (CBT), OCD patients are asked to overcome intrusive thoughts by not indulging in any compulsions. They are taught that rituals keep OCD strong, while not performing them causes OCD to become weaker.[65] This position is supported by the pattern of memory distrust; the more often compulsions are repeated, the more weakened memory trust becomes, and this cycle continues as memory distrust increases compulsion frequency.[66] For body-focused repetitive behaviors (BFRB) such as trichotillomania (hair pulling), skin picking, and onychophagia (nail biting), behavioral interventions such as habit reversal training and decoupling are recommended for the treatment of compulsive behaviors.[67][68] OCD sometimes manifests without overt compulsions, which may be termed "primarily obsessional OCD." OCD without overt compulsions could, by one estimate, characterize as many as 50–60% of OCD cases.[69] Insight and overvalued ideation The Diagnostic and Statistical Manual of Mental Disorders (DSM-5), identifies a continuum for the level of insight in OCD, ranging from good insight (the least severe) to no insight (the most severe). Good or fair insight is characterized by the acknowledgment that obsessive–compulsive beliefs are not or may not be true, while poor insight, in the middle of the continuum, is characterized by the belief that obsessive–compulsive beliefs are probably true. The absence of insight altogether, in which the individual is completely convinced that their beliefs are true, is also identified as a delusional thought pattern, and occurs in about 4% of people with OCD.[70][71] When cases of OCD with no insight become severe, affected individuals have an unshakable belief in the reality of their delusions, which can make their cases difficult to differentiate from psychotic disorders.[72] Some people with OCD exhibit what is known as overvalued ideas, ideas that are abnormal compared to affected individuals' respective cultures, and more treatment-resistant than most negative thoughts and obsessions.[73] After some discussion, it is possible to convince the individual that their fears are unfounded. It may be more difficult to practice exposure and response prevention therapy (ERP) on such people, as they may be unwilling to cooperate, at least initially.[74] Similar to how insight is identified on a continuum, obsessive-compulsive beliefs are characterized on a spectrum, ranging from obsessive doubt to delusional conviction. In the United States, overvalued ideation (OVI) is considered most akin to poor insight—especially when considering belief strength as one of an idea's key identifiers.[75] Furthermore, severe and frequent overvalued ideas are considered similar to idealized values, which are so rigidly held by, and so important to affected individuals, that they end up becoming a defining identity.[73] In adolescent OCD patients, OVI is considered a severe symptom.[76] Historically, OVI has been thought to be linked to poorer treatment outcome in patients with OCD, but it is currently considered a poor indicator of prognosis.[76][77] The Overvalued Ideas Scale (OVIS) has been developed as a reliable quantitative method of measuring levels of OVI in patients with OCD, and research has suggested that overvalued ideas are more stable for those with more extreme OVIS scores.[78] Cognitive performance Though OCD was once believed to be associated with above-average intelligence, this does not appear to necessarily be the case.[79] A 2013 review reported that people with OCD may sometimes have mild but wide-ranging cognitive deficits, most significantly those affecting spatial memory and to a lesser extent with verbal memory, fluency, executive function, and processing speed, while auditory attention was not significantly affected.[80] People with OCD show impairment in formulating an organizational strategy for coding information, set-shifting, and motor and cognitive inhibition.[81] Specific subtypes of symptom dimensions in OCD have been associated with specific cognitive deficits.[82] For example, the results of one meta-analysis comparing washing and checking symptoms reported that washers outperformed checkers on eight out of ten cognitive tests.[83] The symptom dimension of contamination and cleaning may be associated with higher scores on tests of inhibition and verbal memory.[84] Video game addiction See also: Video game addiction This section is an excerpt from Digital media use and mental health § OCD.[edit] In April 2018, the International Journal of Environmental Research and Public Health published a systematic review of 24 studies researching associations between internet gaming disorder (IGD) and various psychopathologies that found a 75% association between IGD and obsessive–compulsive disorder symptoms.[85] Pediatric OCD Approximately 1–2% of children are affected by OCD.[86] There is a lot of similarity between the clinical presentation of OCD in children and adults, and it is considered a highly familial disorder, with a phenotypic heritability of around 50%.[38][87] Obsessive–compulsive disorder symptoms tend to develop more frequently in children 10–14 years of age, with males displaying symptoms at an earlier age, and at a more severe level than females.[88] In children, symptoms can be grouped into at least four types, including sporadic and tic-related OCD.[36] The Children's Yale–Brown Obsessive–Compulsive Scale (CY-BOCS) is the gold standard measure for assessment of pediatric OCD.[89] It follows the Y-BOCS format, but with a Symptom Checklist that is adapted for developmental appropriateness. Insight, avoidance, indecisiveness, responsibility, pervasive slowness, and doubting, are not included in a rating of overall severity. The CY-BOCS has demonstrated good convergent validity with clinician-rated OCD severity, and good to fair discriminant validity from measures of closely related anxiety, depression, and tic severity.[89] The CY-BOCS Total Severity score is an important monitoring tool as it is responsive to pharmacotherapy and psychotherapy.[90][91] Positive treatment response is characterized by 25% reduction in CY-BOCS total score, and diagnostic remission is associated with a 45%-50% reduction in Total Severity score (or a score <15).[89] CBT is the first line treatment for mild to moderate cases of OCD in children, while medication plus CBT is recommended for moderate to severe cases.[92][93][94] Serotonin reuptake inhibitors (SRIs) are first-line medications for OCD in children with established AACAP guidelines for dosing.[95] Associated conditions People with OCD may be diagnosed with other conditions as well, such as obsessive–compulsive personality disorder, major depressive disorder, bipolar disorder, generalized anxiety disorder, anorexia nervosa, social anxiety disorder, bulimia nervosa, Tourette syndrome, transformation obsession, ASD, ADHD, dermatillomania, body dysmorphic disorder, and trichotillomania.[96] More than 50% of people with OCD experience suicidal tendencies, and 15% have attempted suicide.[17] Depression, anxiety, and prior suicide attempts increase the risk of future suicide attempts.[97] It has been found that between 18 and 34% of females currently experiencing OCD scored positively on an inventory measuring disordered eating.[98] Another study found that 7% are likely to have an eating disorder,[98] while another found that fewer than 5% of males have OCD and an eating disorder.[99] Individuals with OCD have also been found to be affected by delayed sleep phase disorder at a substantially higher rate than the general public.[100][101] Moreover, severe OCD symptoms are consistently associated with greater sleep disturbance. Reduced total sleep time and sleep efficiency have been observed in people with OCD, with delayed sleep onset and offset.[101] Some research has demonstrated a link between drug addiction and OCD. For example, there is a higher risk of drug addiction among those with any anxiety disorder, likely as a way of coping with the heightened levels of anxiety. However, drug addiction among people with OCD may be a compulsive behavior. Depression is also extremely prevalent among people with OCD. One explanation for the high depression rate among OCD populations was posited by Mineka, Watson, and Clark (1998), who explained that people with OCD, or any other anxiety disorder, may feel "out of control".[102] Someone exhibiting OCD signs does not necessarily have OCD. Behaviors that present as obsessive–compulsive can also be found in a number of other conditions, including obsessive–compulsive personality disorder (OCPD), autism spectrum disorder (ASD), or disorders in which perseveration is a possible feature (ADHD, PTSD, bodily disorders, or stereotyped behaviors).[103] Some cases of OCD present symptoms typically associated with Tourette syndrome, such as compulsions that may appear to resemble motor tics; this has been termed tic-related OCD or Tourettic OCD.[104][105] OCD frequently occurs comorbidly with both bipolar disorder and major depressive disorder. Between 60 and 80% of those with OCD experience a major depressive episode in their lifetime. Comorbidity rates have been reported at between 19 and 90%, as a result of methodological differences. Between 9–35% of those with bipolar disorder also have OCD, compared to 1–2% in the general population. About 50% of those with OCD experience cyclothymic traits or hypomanic episodes. OCD is also associated with anxiety disorders. Lifetime comorbidity for OCD has been reported at 22% for specific phobia, 18% for social anxiety disorder, 12% for panic disorder, and 30% for generalized anxiety disorder. The comorbidity rate for OCD and ADHD has been reported to be as high as 51%.[106] |
徴候と症状 OCDは様々な症状を呈す。ある種の症状群は、通常、次元やクラスターとして一緒に現れることが多く、そ れは根底にあるプロセスを反映している可能性があります。OCDの標準的な評価ツールであるYale-Brown Obsessive Compulsive Scale(Y-BOCS)では、13の症状カテゴリーが定義されています。症状構造に関するメタ分析のレビューでは、対称性因子、禁止思考因子、掃除因 子、ため込み因子の4因子のグループ化構造が最も信頼できるとしている。対称性因子は、順序付け、数え上げ、対称性に関する強迫観念、および反復強迫と高 い相関がある。禁じられた考え因子は、暴力的、宗教的、性的な性質の侵入的な考えと高い相関がある。掃除因子は、汚染に関する強迫観念や掃除に関する強迫 観念と高い相関がある。ため込み因子は、ため込みに関連する強迫観念と強迫行為のみを含み、他の症状群とは異なるものとして同定された[37]。 OCDの発症について調べると、ある研究によると、男性と女性では発症年齢に違いがあり、OCDの平均発症年齢は男性の子供で9.6歳、女性の子供で 11.0歳であることが示唆されています[38]。OCDを持つ子供は、ADHD、うつ病、不安障害、破壊行動障害などの他の精神障害を持つことがよくあ ります。大人と子供の両方を調査した研究によると、発症の平均年齢は男性で21歳、女性で24歳でした[39]。OCDの発症が早ければ早いほど重症度が 高いという研究結果もありますが、他の研究ではこの所見を検証することはできませんでした[40]。特に女性を調査した別の研究では、参加者の62%が月 経前の年齢で症状が悪化することが示唆されています。全ての人口統計や研究において、平均発症年齢は25歳未満であった[41]。 OCDのサブタイプには、パターン認識(洗濯サブタイプ)や空間的 ワーキングメモリー(強迫観念サブタイプ)のように、特定のタスク のパフォーマンスの改善と関連しているものもある。サブグループは神経画像所見や治療反応によっても区別されているが、神経画像研究は結論を出すほど包括 的なものではない。サブタイプに依存した治療反応が研究されており、ため込みサブタイプは一貫して治療反応が最も低い[42]。 OCDは神経心理学的には同質の障害と考えられているが、症状の多くは併存する障害の結果である可能性がある。例えば、OCDを持つ成人は、OCDを持た ない成人に比べ、注意欠陥/多動性障害(ADHD)や自閉スペクトラム症(ASD)の症状をより多く示している[43]。 発症の原因に関して、研究者はある研究[41]の参加者に、最初の発症の引き金となったのは何だと思うか質問しました。その結果、29%の患者が生活の中 に環境的な要因があると答えました。特に、そう答えた参加者の大多数は、その環境要因が責任感の高まりに関係していると指摘している。 強迫観念 主な記事 強迫観念 参照: 主に強迫観念にとらわれる強迫性障害 強迫観念は、無視しようとしたり、立ち向かおうとしたりする努力にもかかわらず、繰り返し持続するストレス誘発性の思考である。個人差はあるが、最初の強 迫観念は明確で鮮明である。比較的漠然とした強迫観念は、一般的な混乱感や緊張感を伴い、その不均衡が残っている間は生活が通常通りには進めないという信 念を伴う。より強い強迫観念は、親しい家族や友人が死ぬという考えやイメージにとらわれたり、人間関係の正しさに関連した侵入的な考えであったりする [45][46]。他の強迫観念は、自分以外の誰かや何か-例えば神、悪魔、病気など-が患者本人や患者が大切にしている人や物に危害を加えるという可能 性に関係する。OCDを持つ他の人は、自分の体から目に見えない突起物が出 ている感覚を経験したり、無生物が霊魂化されていると感じたりする。scrupulosityでは、人の強迫観念は、悪人であることへの恐れや、罪に対す る神の報復への恐れなど、道徳的または宗教的な恐れに焦点を当てている。 OCDの人の中には、「他人、知人、両親、子供、家族、友人、同僚、動物、宗教的 人物」との「キス、触れ合い、愛撫、オーラルセックス、アナルセックス、性交、近親相姦、レイプ」 などの侵入的な考えやイメージを伴う性的強迫観念を経験する人もおり、年齢に関係なく異 性的または同性愛的な接触を含むことがあります。例えば、性的指向に対する強迫的な恐怖は、性的アイデンティティの危機として、患 者本人や周囲の人にさえも現れることがある[53][54]。さらに、強迫性障害に伴う疑心暗鬼は、厄介な思考を行動に移すかどうかの不 安につながり、その結果、自己批判や自己嫌悪に陥る[52]。 OCDのほとんどの人は、自分の考えが現実と一致していないことを理解してい るが、その考えが正しい、あるいは現実的であるかのように行動しなければならないと 感じている。例えば、強迫的に物を溜め込んでしまう人は、そのような行動が知的レベルでは非合理的であることを受け入れているにもかかわらず、無機物をあ たかも生物の感覚や権利を持っているかのように扱う傾向があるかもしれません。溜め込みがOCDから独立した症候群とみなされるべきかどうかについては議 論がある[55]。 強迫観念 主な記事 強迫行為 強迫性障害のある人の中には、どうしてもそうしなければならないと感じて強迫的な儀式を行う人もいれば、強迫観念からくる不安を和らげるために強迫的な行 動をとる人もいます。このような行動をとることで、恐ろしい出来事の発生を防いだり、その出来 事を自分の考えから遠ざけたりすることができると感じているのでしょう。いずれにせよ、その理性は非常に特異であるか、または歪んでいるため、個人的に、 または罹患者の周囲の人々にとって、重大な苦痛をもたらす。過剰な皮膚摘み、毛抜き、爪噛み、その他の身体に焦点をあてた反復行動障害はすべて強迫スペク トラムに属する。 [56]さらに、強迫観念はしばしば記憶不信に起因しており、明確な証拠がない場合でも、知覚、注意、記憶の能力に対する不安によって特徴づけられる OCDの症状である[57]。 一般的な強迫行為には、手洗い、掃除、物の確認(ドアの鍵など)、動作の繰り返し(スイッチのオン・オフを繰り返すなど)、特定の方法で品物を注文する、 安心感を求めることなどが含まれる[58][59]。動作を繰り返し行う人もいるが、必ずしもこれらの動作を強迫的に行うとは限らない。例えば、朝晩の日 課や宗教的な習慣は通常強迫行為ではない。行動が強迫とみなされるか、単なる習慣とみなされるかは、その行動が行われる状況によって異なる。例えば、1日 8時間本を並べたり注文したりすることは、図書館で働く人には期待されることであるが、他の状況ではこの習慣は異常に思えるだろう。言い換えれば、習慣は 生活に効率性をもたらす傾向があり、強迫観念は生活を混乱させる傾向がある[60]。さらに、強迫観念はチック(触る、たたく、こする、まばたきなど)や 定型動作(頭をたたく、体を揺する、自己咬合など)とは異なり、通常はそれほど複雑ではなく、強迫観念によって引き起こされることもない。 [61]強迫観念と複雑なチックを区別することは時に困難であり、OCD患者の約10-40%は生涯チック障害を伴う[2][62]。 OCDの人は強迫観念を強迫観念からの逃避として利用しますが、強迫観念は一時的なものであり、また強迫観念が戻ってくることを自覚しています。強迫観念 を持つ人の中には、強迫観念の引き金となるような状況を避けるために強迫観念を用いる人もいる。強迫観念は、汚染に取りつかれた人が強迫的に手を洗うよう に、強迫観念と直接関係のある行動であることもあるが、無関係の行動であることもある[9]。OCDに典型的に伴う不安や恐怖を経験することに加え、罹患 者は毎日何時間も強迫観念を行うことがある。このような状況では、仕事、家族、社会的役割を果たすことが困難になります。このような行動はまた、有害な身 体的症状を引き起こすこともある。例えば、抗菌石鹸と熱いお湯で執拗に手を洗う人は、皮膚炎で皮膚が赤くなり、生皮になることがある[63]。 OCDを持つ人は、自分の行動を説明するために、しばしば合理化を用いますが、こ れらの合理化は行動パターンに適用されるのではなく、個々の出来事に適用されま す。例えば、強迫的に玄関のドアをチェックする人は、1回のチェックに関連する時 間やストレスは、泥棒に入られることに関連する時間やストレスよりも少なく、結果 的にチェックする方が良い選択であると主張するかもしれない。このような推論は周期的に起こることが多く、被害を受けた人が安全だと感じるために必要なだ け続くことがある[64]。 認知行動療法(CBT)では、OCD患者は強迫行為にふけることなく、侵入的思考を克服す るよう求められる。この考え方は記憶不信のパターンから支持されており、強迫観念が繰り返される頻度 が高ければ高いほど、記憶に対する信頼は弱くなり、記憶不信が強迫観念の頻度を増加させる というサイクルが続く。 [66] トリコチロマニア(毛抜き)、スキンピッキング、爪噛みなどの身体に焦点をあてた反復行動(BFRB)に対しては、習慣逆転訓練やデカップリングなどの行 動介入が強迫行動の治療に推奨されている[67][68]。 OCDは時に、あからさまな強迫観念を伴わずに現れることがあり、これは 「主に強迫性OCD 」と呼ばれる。あからさまな強迫観念を伴わないOCDは、OCD症例の50~60%を占めると推定されている[69]。 洞察と過大観念 精神障害の診断と統計マニュアル(DSM-5)では、OCDの洞察のレベルについて、良好な洞察(最 も深刻ではないもの)から洞察なし(最も深刻なもの)までの連続性を示しています。洞察が良い、あるいはまあまあ良いとは、強迫観念が真実でない、あるい は真実でない可能性があることを認めていることを特徴とし、洞察が悪いとは、連続体の中間に位置し、強迫観念がおそらく真実であると信じていることを特徴 とする。洞察が全くない場合、自分の信念が真実であると完全に思い込 んでいる状態であり、妄想的思考パターンとして同定され、OCD患者の約4% にみられる[70][71]。洞察のないOCDが重症化すると、罹患者は妄想の現実性 を揺るぎない信念として持つようになり、精神病性障害との鑑別が困難 になる[72]。 OCDの人の中には、過大評価された観念、つまり罹患者のそれぞれの文化に 比べて異常な観念を示し、ほとんどの否定的な考えや強迫観念よりも治療抵抗性 が高い人もいる[73]。このような人々に対して暴露療法や反応妨害療法(ERP)を実施することは、少なくとも当初は協力しようとしないため、より困難 である可能性がある。米国では、過大評価観念(OVI)は洞察力の欠如に最も類似していると考え られており、特に信念の強さを観念の主要な識別因子の1つと考える場合 [75] 、さらに、重度かつ頻度の高い過大評価観念は理想化された価 値観に類似していると考えられており、理想化された価値観は、罹患者によ って厳格に保持され、罹患者にとって非常に重要であるため、最終的にそ れが決定的なアイデンティティとなる[73]。青年期のOCD患者では、 OVIは重篤な症状と考えられている[76]。 歴史的に、OVIはOCD患者の治療成績の低下につながると考えられてきたが、現 在では予後の悪い指標であると考えられている[76][77]。過大評価観念尺度(OVIS)はOCD患者のOVIレベルを測定する信頼性の高い定量的な 方法として開発され、OVISのスコアが極端に高い人ほど過大評価観念が安定していることが研究で示唆されている[78]。 認知能力 OCDはかつては平均以上の知能を持つと信じられていましたが、必ずしもそうではな いようです[79]。2013年の総説によると、OCD患者は時に軽度ではあるが幅広い認知 機能障害を持つことがあり、最も顕著なのは空間的記憶、言語的記憶、流暢さ、実行機能、処理 速度に影響を及ぼすもので、聴覚的注意には有意な影響は見られないと報告されてい ます[80]。OCD患者は、情報をコード化するための組織的戦略の策定、セットシフト、運動 や認知の抑制に障害を示します[81]。 OCDの症状次元の特定のサブタイプは、特定の認知障害と関連している[82]。 例えば、洗浄とチェックの症状を比較したあるメタアナリシスの結果では、10個の認知テストのうち8個で洗浄者がチェック者を上回ったと報告されている[83]。 ビデオゲーム中毒 関連項目 ビデオゲーム中毒 本項は、デジタルメディアの利用とメンタルヘルス§OCDからの抜粋である[編集]。 2018年4月、International Journal of Environmental Research and Public Healthは、インターネットゲーム障害(IGD)と様々な精神病理学との関連を研究した24の研究のシステマティックレビューを発表し、IGDと強迫 性障害の症状との間に75%の関連があることを明らかにした[85]。 小児OCD 小児の約1~2%がOCDに罹患している[86]。小児と成人のOCDの臨床症状には多くの類似性があり、表現型の遺伝率は約50%で、非常に家族性の高 い障害と考えられている。 [38][87]強迫性障害の症状は、10~14歳の子供に多く発症する傾向があり、男性は女性よりも早い年齢で、より重篤な症状を示す[88]。 Children's Yale-Brown Obsessive-Compulsive Scale (CY-BOCS)は小児のOCDを評価するための最も標準的な尺度です。洞察力、回避、優柔不断、責任感、広範な遅さ、疑心暗鬼は全体的な重症度の評価 には含まれない。CY-BOCSは臨床医が評価したOCDの重症度と良好な収束的妥当性を示し、密接に関連する不安、抑うつ、チックの重症度の尺度とは良 好から公正な判別的妥当性を示している。 CBTは小児のOCDの軽度から中等度の症例に対する第一選択薬であり、中等度から重度の症例には薬物療法とCBTの併用が推奨される[92][93] [94]。セロトニン再取り込み阻害薬(SRI)は小児のOCDに対する第一選択薬であり、投与に関するAACAPガイドラインが確立されている [95]。 関連疾患 強迫性パーソナリティ障害、大うつ病性障害、双極性障害、全般性不安障害、神経性食欲不振症、社交不安障害、神経性過食症、トゥレット症候群、変身願望、 ASD、ADHD、皮膚滴定症、身体醜形障害、トリコチロマニアなど。 [96] OCD患者の50%以上が自殺傾向を経験し、15%が自殺未遂を経験している[17] 。 現在OCDを経験している女性の18~34%が摂食障害を測定するインベントリで正のスコアを示 していることが判明している[98]。別の研究では、7%が摂食障害である可能性が高いことが判明し ており[98]、別の研究では、OCDと摂食障害を持つ男性は5%未満であることが判明し ている[99]。 また、OCDを持つ人は、一般的な人よりもかなり高い割合で睡眠相後退症に罹患していることが判明しています[100][101]。 さらに、重度のOCD症状は、より大きな睡眠障害と一貫して関連しています。OCD患者では総睡眠時間や睡眠効率の減少が観察され、入眠やオフセ ットも遅れている[101]。 薬物中毒とOCDの関連性を示す研究もあります。例えば、不安障害のある人は薬物中毒になる危険性が高く、これは高 まった不安レベルに対処するためと考えられている。しかし、OCD患者の薬物中毒は強迫行為である可能性がある。うつ病もOCD患者の間で非常に多くみら れます。OCD患者のうつ病率が高いことの説明の1つとして、Mineka, Watson, and Clark (1998)は、OCDやその他の不安障害のある人は「コントロールできない」と感じている可能性があると説明している[102]。 OCDの兆候を示す人が必ずしもOCDであるとは限りません。強迫性パーソナリティ障 害(OCPD)、自閉症スペクトラム障がい(ASD)、忍耐が特徴的な障がい(ADHD、PTSD、身体障 害、定型行動)など、強迫として現れる行動は他の疾患でも見られることがありま す。 [103] OCDの中には、トゥレット症候群と典型的に関連する症状、例えば、運動性チックに似た強迫観念を示す症例があり、これはチック関連OCDまたはトゥレッ トOCDと呼ばれている。 OCDは双極性障害や大うつ病性障害と併存することが多い。OCD患者の60~80%が一生の間に大うつ病エピソードを経験しています。併存率は 19~90%と報告されているが、これは方法論の違いによるものである。双極性障害患者の9-35%はOCDを合併しており、一般人口の1-2%である。 OCDを持つ人の約50%は、周期性発作や軽躁病エピソードを経験しています。OCDは不安障害とも関連しています。OCDの生涯併存率は、特定恐怖症 22%、社交不安障害18%、パニック障害12%、全般性不安障害30%と報告されています。OCDとADHDの併存率は51%と報告されている [106]。 |
| Causes Main article: Cause of obsessive-compulsive disorder The cause of OCD is unknown.[1] Both environmental and genetic factors are believed to play a role. Risk factors include a history of adverse childhood experiences or other stress-inducing events.[2][107][108] Drug-induced OCD Some medications, toxin exposures, and drugs, such as methamphetamine or cocaine, can induce obsessive-compulsive disorder (OCD) in people without previous symptoms.[108] Some atypical antipsychotics (second-generation antipsychotics) such as olanzapine (Zyprexa) and clozapine (Clozaril) can induce OCD in people, particularly individuals with schizophrenia. The diagnostic criteria include: 1) General OCD symptoms (obsessions, compulsions, skin picking, hair pulling, etc.) that developed soon after exposure to the substance or medication which can produce such symptoms. 2) The onset of symptoms cannot be explained by an obsessive-compulsive and related disorder that is not substance/medication-induced and should last for a substantial period of time (about 1 month) 3) This disturbance does not only occur during delirium. 4) Clinically induces distress or impairment in social, occupational, or other important areas of functioning. [109][110][111][112][113] Genetics There appear to be some genetic components of OCD causation, with identical twins more often affected than fraternal twins.[2] Furthermore, individuals with OCD are more likely to have first-degree family members exhibiting the same disorders than matched controls. In cases in which OCD develops during childhood, there is a much stronger familial link in the disorder than with cases in which OCD develops later in adulthood. In general, genetic factors account for 45–65% of the variability in OCD symptoms in children diagnosed with the disorder.[114] A 2007 study found evidence supporting the possibility of a heritable risk for OCD.[115] Research has found there to be a genetic correlation between anorexia nervosa and OCD, suggesting a strong etiology.[116][117][118] First and second hand relatives of probands with OCD have a greater risk of developing anorexia nervosa as genetic relatedness increases.[116] A mutation has been found in the human serotonin transporter gene hSERT in unrelated families with OCD.[119] A systematic review found that while neither allele was associated with OCD overall, in Caucasians, the L allele was associated with OCD.[120] Another meta-analysis observed an increased risk in those with the homozygous S allele, but found the LS genotype to be inversely associated with OCD.[121] A genome-wide association study found OCD to be linked with single-nucleotide polymorphisms (SNPs) near BTBD3, and two SNPs in DLGAP1 in a trio-based analysis, but no SNP reached significance when analyzed with case-control data.[122] One meta-analysis found a small but significant association between a polymorphism in SLC1A1 and OCD.[123] The relationship between OCD and Catechol-O-methyltransferase (COMT) has been inconsistent, with one meta-analysis reporting a significant association, albeit only in men, and another meta analysis reporting no association.[124][125] It has been postulated by evolutionary psychologists that moderate versions of compulsive behavior may have had evolutionary advantages. Examples would be moderate constant checking of hygiene, the hearth, or the environment for enemies. Similarly, hoarding may have had evolutionary advantages. In this view, OCD may be the extreme statistical tail of such behaviors, possibly the result of a high number of predisposing genes.[126] Brain structure and functioning Imaging studies have shown differences in the frontal cortex and subcortical structures of the brain in patients with OCD. There appears to be a connection between the OCD symptoms and abnormalities in certain areas of the brain, but such a connection is not clear.[21] Some people with OCD have areas of unusually high activity in their brain, or low levels of the chemical serotonin,[127] which is a neurotransmitter that some nerve cells use to communicate with each other,[128] and is thought to be involved in regulating many functions, influencing emotions, mood, memory, and sleep.[129] Autoimmune A controversial hypothesis is that some cases of rapid onset of OCD in children and adolescents may be caused by a syndrome connected to Group A streptococcal infections (GABHS), known as pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections (PANDAS).[130][131][132] OCD and tic disorders are hypothesized to arise in a subset of children as a result of a post-streptococcal autoimmune process.[133][134][135] The PANDAS hypothesis is unconfirmed and unsupported by data, and two new categories have been proposed: PANS (pediatric acute-onset neuropsychiatric syndrome) and CANS (childhood acute neuropsychiatric syndrome).[134][135] The CANS and PANS hypotheses include different possible mechanisms underlying acute-onset neuropsychiatric conditions, but do not exclude GABHS infections as a cause in a subset of individuals.[134][135] PANDAS, PANS, and CANS are the focus of clinical and laboratory research, but remain unproven.[133][134][135] Whether PANDAS is a distinct entity differing from other cases of tic disorders or OCD is debated.[136][137][138][139] A review of studies examining anti-basal ganglia antibodies in OCD found an increased risk of having anti-basal ganglia antibodies in those with OCD versus the general population.[140] Environment OCD may be more common in people who have been bullied, abused, or neglected, and it sometimes starts after a significant life event, such as childbirth or bereavement.[127] It has been reported in some studies that there is a connection between childhood trauma and obsessive-compulsive symptoms. More research is needed to understand this relationship better.[21] |
原因 主な記事 強迫性障害の原因 強迫性障害の原因は不明である[1]が、環境的要因と遺伝的要因の両方が関与していると考えられている。危険因子としては、小児期の不利な経験やその他のストレスを誘発する出来事の既往が挙げられる[2][107][108]。 薬剤性OCD オランザピン(ジプレキサ)やクロザピン(クロザリル)などの非定型抗精神病薬(第二世代抗精神病薬)は、特に統合失調症の人にOCDを誘発することがあります。 診断基準は以下の通りです: 1)一般的なOCD症状(強迫観念、強迫行為、皮膚摘み、毛抜きなど)が、そのような症状を引き起こす物質や薬剤に暴露された直後に発症したこと。 2) その症状の発現は、物質や薬物によって誘発されたものではない強迫性障害や関連障害では説明できず、相当期間(約1ヶ月)持続すること。 3) この障害はせん妄時だけに起こるのではない。 4) 臨床的に、社会的、職業的、またはその他の重要な機能領域において苦痛または障害を引き起こす。[109][110][111][112][113] 遺伝 一卵性双生児は二卵性双生児よりも罹患率が高く、OCDの発症には遺伝的な要素もあるようです。OCDが小児期に発症する場合、成人期以降に発症する場合 よりも、家族的な関連性が強い。一般的に、OCDと診断された小児におけるOCD症状のばらつきの45-65%は遺伝的 要因によるものである[114]。 神経性食欲不振症とOCDの間には遺伝的相関があり、強い病因があることが示唆さ れている[116][117][118]。OCDを発症した患者の第一及び第二の親族は、遺伝的関連性が高 まるにつれて神経性食欲不振症を発症するリスクが高くなる[116]。 ヒトのセロトニントランスポーター遺伝子hSERTにOCDを持つ血縁関係のない家族で変異が見つかっている[119]。 システマティック・レビューによると、どちらの対立遺伝子も全体的にOCDと関連していないが、白人ではL対立遺伝子がOCDと関連していた[120]。 別のメタアナリシスでは、ホモ接合のS対立遺伝子を持つ人のリスク増加が観察されたが、LS遺伝子型はOCDと逆相関していた[121]。 ゲノムワイド関連研究では、OCDはBTBD3近傍の一塩基多型(SNP)と、トリオベースの解析ではDLGAP1の2つのSNPと関連していることが発見されたが、症例対照データで解析した場合には有意となるSNPはなかった[122]。 あるメタアナリシスでは、SLC1A1の多型と強迫性障害との間にわずかではあるが有意な関連が認められた[123]。 OCDとカテコール-O-メチルトランスフェラーゼ(COMT)の関係は一貫しておらず、あるメタアナリシスでは男性のみであるが有意な関連があると報告され、別のメタアナリシスでは関連がないと報告されている[124][125]。 進化心理学者によって、中程度の強迫行為には進化上の利点があった可能性があると仮定されている。例えば、衛生状態や囲炉裏、あるいは敵がいないかどうか 環境を常にチェックするような、適度な強迫行為である。同様に、溜め込みも進化的に有利であった可能性がある。この見解では、OCDはそのような行動の極 端な統計的末尾であり、おそらくは素因となる遺伝子の数が多い結果であると考えられる[126]。 脳の構造と機能 画像研究により、OCD患者の脳の前頭葉皮質と皮質下構造の違いが示され ている。OCDの症状と脳の特定の部位の異常との間には関連性があるように思われ ますが、そのような関連性は明らかではありません[21]。OCDを持つ人の中には、脳の活動が異常に高い部位を持 つ人や、化学物質であるセロトニンのレベルが低い人がいます[127]。セロトニンは、 神経細胞が互いにコミュニケーションをとるために使用する神経伝達物質で[128]、感情、 気分、記憶、睡眠に影響を与えるなど、多くの機能の調節に関与していると 考えられています[129]。 自己免疫 小児や青年におけるOCDの急速な発症のいくつかの症例は、A群溶血性連鎖球菌感染症(GABHS)に関連した症候群が原因である可能性があり、溶血性連 鎖球菌感染症に関連した小児自己免疫性神経精神疾患(PANDAS)として知られている。 [130] [131] [132] OCDおよびチック障害は、溶連菌感染後の自己免疫過程の結果として、小児のサブセットで生じるという仮説がある [133] [134] [135] PANDAS仮説は未確認であり、データによる裏付けもないため、2つの新しいカテゴリーが提唱されている: PANS(小児急性発症神経精神症候群)およびCANS(小児急性神経精神症候群)である[134][135]。CANSおよびPANS仮説には、急性発 症神経精神疾患の根底にある異なる可能性のある機序が含まれるが、個体のサブセットにおける原因としてGABHS感染を除外するものではない。 [134][135]PANDAS、PANS、およびCANSは、臨床研究および実験室研究の焦点であるが、依然として証明されていない[133] [134][135]。PANDASがチック障害または強迫性障害の他の症例とは異なる別個の実体であるかどうかは、議論されている[136][137] [138][139]。 強迫性障害における抗基底神経節抗体を調査した研究のレビューによると、強迫性障害の患者において、一般集団と比較して抗基底神経節抗体を有するリスクが高いことが判明している[140]。 環境 OCDは、いじめや虐待、ネグレクトを受けた経験のある人に多くみられ、出産や死別な どの人生の重要な出来事の後に発症することもあります。この関係をよりよく理解するためには、さらなる研究が必要である[21]。 |
| Mechanisms Main article: Biology of obsessive–compulsive disorder Neuroimaging 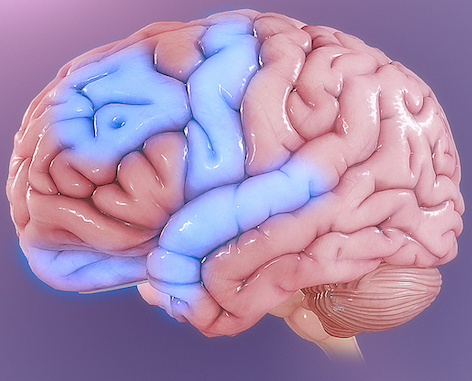 Some parts of the brain showing abnormal activity in OCD: Orbitofrontal cortex integrates rewards, emotions, and behaviors; anterior cingulate cortex is involved in error detection; amygdala is involved in emotional interpretation of reward Functional neuroimaging during symptom provocation has observed abnormal activity in the orbitofrontal cortex (OFC), left dorsolateral prefrontal cortex (dlPFC), right premotor cortex, left superior temporal gyrus, globus pallidus externus, hippocampus, and right uncus. Weaker foci of abnormal activity were found in the left caudate, posterior cingulate cortex, and superior parietal lobule.[141] However, an older meta-analysis of functional neuroimaging in OCD reported that the only consistent functional neuroimaging finding was increased activity in the orbital gyrus and head of the caudate nucleus, while anterior cingulate cortex (ACC) activation abnormalities were too inconsistent.[142] A meta-analysis comparing affective and nonaffective tasks observed differences with controls in regions implicated in salience, habit, goal-directed behavior, self-referential thinking, and cognitive control. For nonaffective tasks, hyperactivity was observed in the insula, ACC, and head of the caudate/putamen, while hypoactivity was observed in the medial prefrontal cortex (mPFC) and posterior caudate. Affective tasks were observed to relate to increased activation in the precuneus and posterior cingulate cortex, while decreased activation was found in the pallidum, ventral anterior thalamus, and posterior caudate.[143] The involvement of the cortico-striato-thalamo-cortical loop in OCD, as well as the high rates of comorbidity between OCD and ADHD, have led some to draw a link in their mechanism. Observed similarities include dysfunction of the anterior cingulate cortex and prefrontal cortex, as well as shared deficits in executive functions.[144] The involvement of the orbitofrontal cortex and dorsolateral prefrontal cortex in OCD is shared with bipolar disorder, and may explain the high degree of comorbidity.[145] Decreased volumes of the dorsolateral prefrontal cortex related to executive function has also been observed in OCD.[146] People with OCD evince increased grey matter volumes in bilateral lenticular nuclei, extending to the caudate nuclei, with decreased grey matter volumes in bilateral dorsal medial frontal/anterior cingulate gyri.[147][145] These findings contrast with those in people with other anxiety disorders, who evince decreased (rather than increased) grey matter volumes in bilateral lenticular/caudate nuclei, as well as decreased grey matter volumes in bilateral dorsal medial frontal/anterior cingulate gyri.[145] Increased white matter volume and decreased fractional anisotropy in anterior midline tracts has been observed in OCD, possibly indicating increased fiber crossings.[148] Cognitive models Generally, two categories of models for OCD have been postulated. The first category involves deficits in executive dysfunction and is based on the observed structural and functional abnormalities in the dlPFC, striatum and thalamus. The second category involves dysfunctional modulatory control and primarily relies on observed functional and structural differences in the ACC, mPFC, and OFC.[149][150] One proposed model suggests that dysfunction in the OFC leads to improper valuation of behaviors and decreased behavioral control, while the observed alterations in amygdala activations leads to exaggerated fears and representations of negative stimuli.[151] Due to the heterogeneity of OCD symptoms, studies differentiating various symptoms have been performed. Symptom-specific neuroimaging abnormalities include the hyperactivity of caudate and ACC in checking rituals, while finding increased activity of cortical and cerebellar regions in contamination-related symptoms. Neuroimaging differentiating content of intrusive thoughts has found differences between aggressive as opposed to taboo thoughts, finding increased connectivity of the amygdala, ventral striatum, and ventromedial prefrontal cortex in aggressive symptoms, while observing increased connectivity between the ventral striatum and insula in sexual or religious intrusive thoughts.[152] Another model proposes that affective dysregulation links excessive reliance on habit-based action selection[153] with compulsions. This is supported by the observation that those with OCD demonstrate decreased activation of the ventral striatum when anticipating monetary reward, as well as increased functional connectivity between the VS and the OFC. Furthermore, those with OCD demonstrate reduced performance in Pavlovian fear-extinction tasks, hyperresponsiveness in the amygdala to fearful stimuli, and hyporesponsiveness in the amygdala when exposed to positively valanced stimuli. Stimulation of the nucleus accumbens has also been observed to effectively alleviate both obsessions and compulsions, supporting the role of affective dysregulation in generating both.[151] Neurobiological From the observation of the efficacy of antidepressants in OCD, a serotonin hypothesis of OCD has been formulated. Studies of peripheral markers of serotonin, as well as challenges with proserotonergic compounds have yielded inconsistent results, including evidence pointing towards basal hyperactivity of serotonergic systems.[154] Serotonin receptor and transporter binding studies have yielded conflicting results, including higher and lower serotonin receptor 5-HT2A and serotonin transporter binding potentials that were normalized by treatment with SSRIs. Despite inconsistencies in the types of abnormalities found, evidence points towards dysfunction of serotonergic systems in OCD.[155] Orbitofrontal cortex overactivity is attenuated in people who have successfully responded to SSRI medication, a result believed to be caused by increased stimulation of serotonin receptors 5-HT2A and 5-HT2C.[156] A complex relationship between dopamine and OCD has been observed. Although antipsychotics, which act by antagonizing dopamine receptors, may improve some cases of OCD, they frequently exacerbate others. Antipsychotics, in the low doses used to treat OCD, may actually increase the release of dopamine in the prefrontal cortex, through inhibiting autoreceptors. Further complicating things is the efficacy of amphetamines, decreased dopamine transporter activity observed in OCD,[157] and low levels of D2 binding in the striatum.[158] Furthermore, increased dopamine release in the nucleus accumbens after deep brain stimulation correlates with improvement in symptoms, pointing to reduced dopamine release in the striatum playing a role in generating symptoms.[159] Abnormalities in glutamatergic neurotransmission have been implicated in OCD. Findings such as increased cerebrospinal glutamate, less consistent abnormalities observed in neuroimaging studies, and the efficacy of some glutamatergic drugs (such as the glutamate-inhibiting riluzole) have implicated glutamate in OCD.[158] OCD has been associated with reduced N-Acetylaspartic acid in the mPFC, which is thought to reflect neuron density or functionality, although the exact interpretation has not been established.[160] |
メカニズム 主な記事 強迫性障害の生物学 神経画像 強迫性障害で異常な活動を示す脳の部位: 前頭眼窩皮質は報酬、感情、行動を統合し、前帯状皮質はエラー検出に関与し、扁桃体は報酬の感情的解釈に関与する。 症状誘発時の機能的ニューロイメージングにより、眼窩前頭皮質(OFC)、左背外側前頭前皮質(dlPFC)、右運動前野、左上側頭回、淡蒼球外側部、海 馬、右大脳半球の異常活動が観察された。異常活動の弱い病巣は左尾状突起、後帯状皮質、上頭頂小葉にみられた[141]。しかしながら、OCDにおける機 能的神経画像に関するより古いメタアナリシスによると、一貫した機能的神経画像所見は眼窩回と尾状核の頭部における活動の増加のみであり、前帯状皮質 (ACC)の活性化異常は一貫性がなさすぎると報告されている[142]。 感情的課題と非感情的課題を比較したメタアナリシスでは、顕著性、習慣性、目標指示行動、自己言及的思考、認知制御に関与する領域で対照との差異が観察さ れた。非感情的課題では、島皮質、ACC、尾状/後頭葉で活動亢進が観察され、内側前頭前皮質(mPFC)と後部尾状葉で活動低下が観察された。OCDに おける皮質-線条体-視床-皮質のループの関与と、OCDと ADHDの併存率の高さから、そのメカニズムに関連性を見出す人も いる[143]。OCDにおける眼窩前頭皮質と背外側前頭前皮質 の関与は双極性障害と共通しており[145]、併存率の高さを説明しうる。 OCDの人は、両側の黒子核の灰白質容積が増加し、尾状核まで拡大し、両側の前頭前野背内側/前帯状回の灰白質容積が減少している。 [147] [145] これらの所見は、両側のレンズ状核/尾状核の灰白質容積の減少(むしろ増加)、および両側の背内側前頭回/前帯状回の灰白質容積の減少を示す他の不安障害 の人の所見とは対照的である[145]。 認知モデル 一般的に、強迫性障害の認知モデルは2つに分類される。1つ目は実行機能障害で、dlPFC、線条体、視床の構造的・機能的異常が観察される。第二のカテ ゴリーは、調節制御の機能障害であり、主にACC、mPFC、OFCにおいて観察された機能的、構造的な違いに基づいている[149][150]。 提案されているモデルの1つは、OFCの機能障害が行動の不適切な評価と行動制御の低下をもたらし、観察された扁桃体活性化の変化が恐怖の誇張と否定的刺激の表象をもたらすことを示唆している[151]。 OCDの症状は異質であるため、様々な症状を鑑別する研究が行われ ている。症状特異的な神経画像異常として、確認儀式では尾状突起とACCの過活動が、汚染関連症状では皮質と小脳領域の活動亢進が認められる。侵入的思考 の内容を鑑別する神経画像では、攻撃的思考とタブー思考とで違いがみられ、攻撃的症状では扁桃体、腹側線条体、および内側前頭前野の結合が亢進している一 方、性的または宗教的侵入的思考では腹側線条体と島との結合が亢進していることが観察された[152]。 別のモデルでは、情動調節障害は習慣に基づく行動選択への過度の依存[153]を強迫と関連づけると提唱している。これは、強迫性障害の患者が金銭的報酬 を予期する際に腹側線条体の活性化が低下し、VSとOFC間の機能的結合が増加しているという観察から支持される。さらに、強迫性障害の患者は、パブロフ 恐怖消滅課題の成績が低下し、恐怖刺激に対する扁桃体の過敏性、正の価値の刺激にさらされたときの扁桃体の低反応性を示す。側坐核を刺激すると、強迫観念 と強迫行為の両方が効果的に緩和されることも観察されており、両者の生成における情動調節障害の役割を裏付けている [151] 。 神経生物学的 OCDにおける抗うつ薬の有効性の観察から、OCDのセロトニン仮説が立てら れている。セロトニンの末梢マーカーの研究やプロセロトニン作動性化合物によるチャレンジは、セロトニン作動性システムの基礎的な過活動を示唆する証拠を 含め、一貫性のない結果をもたらした[154]。セロトニン受容体およびトランスポーターの結合研究は、SSRIによる治療によって正常化されたセロトニ ン受容体5-HT2Aおよびセロトニントランスポーター結合電位の高低を含め、相反する結果をもたらした。発見された異常のタイプに一貫性はないものの、 OCDにおけるセロトニン作動性システムの機能障害を示唆する証拠がある[155]。SSRIによる薬物療法が奏功した人では、眼窩前頭皮質の過活動が減 弱しており、この結果はセロトニン受容体5-HT2Aおよび5-HT2Cの刺激増加によって引き起こされると考えられている[156]。 ドパミンと強迫性障害の複雑な関係が観察されている。ドパミン受容体に拮抗する抗精神病薬は、OCDを改善する場合もあるが、他の症例を悪化させることも 多い。抗精神病薬はOCDの治療に使われる低用量では、自己受容体を阻害することにより、前頭前野のドーパミンの放出を実際に増加させる可能性がある。さ らに物事を複雑にしているのは、アンフェタミンの有効性、OCDで観察されるドーパミントランスポーター活性の低下[157]、線条体におけるD2結合の 低レベル[158]である。さらに、脳深部刺激後の側坐核におけるドーパミン放出の増加は症状の改善と相関しており、線条体におけるドーパミン放出の減少 が症状の発生に関与していることを示唆している[159]。 グルタミン酸作動性神経伝達の異常はOCDに関与している。脳脊髄グルタミン酸の増加、神経画像研究で観察された一貫性のない 異常、いくつかのグルタミン酸作動性薬物(グルタミン酸を阻害するリルゾー ルなど)の有効性などの所見から、グルタミン酸がOCDに関与していることが示唆 されている[158]。OCDはmPFCのN-アセチルアスパラギン酸の減少と関連してお り、これはニューロンの密度や機能性を反映していると考えられているが、 正確な解釈は確立されていない[160]。 |
| Diagnosis Formal diagnosis may be performed by a psychologist, psychiatrist, clinical social worker, or other licensed mental health professional. OCD, like other mental and behavioral health disorders, cannot be diagnosed by a medical exam,[7] nor are there any medical exams that can predict if one will fall victim to such illnesses. To be diagnosed with OCD, a person must have obsessions, compulsions, or both, according to the Diagnostic and Statistical Manual of Mental Disorders (DSM). The DSM notes that there are multiple characteristics that can turn obsessions and compulsions from normalized behavior to "clinically significant". There has to be recurring and strong thoughts or impulsive that intrude on the day-to-day lives of the patients and cause noticeable levels of anxiousness.[2] These thoughts, impulses, or images are of a degree or type that lies outside the normal range of worries about conventional problems.[161] A person may attempt to ignore or suppress such obsessions, neutralize them with another thought or action, or try to rationalize their anxiety away. People with OCD tend to recognize their obsessions as irrational. Compulsions become clinically significant when a person feels driven to perform them in response to an obsession, or according to rules that must be applied rigidly, and when the person consequently feels or causes significant distress. Therefore, while many people who do not have OCD may perform actions often associated with OCD (such as ordering items in a pantry by height), the distinction with clinically significant OCD lies in the fact that the person with OCD must perform these actions to avoid significant psychological distress. These behaviors or mental acts are aimed at preventing or reducing distress or preventing some dreaded event or situation; however, these activities are not logically or practically connected to the issue, or, they are excessive. Moreover, the obsessions or compulsions must be time-consuming, often taking up more than one hour per day, or cause impairment in social, occupational, or scholastic functioning.[161] It is helpful to quantify the severity of symptoms and impairment before and during treatment for OCD. In addition to the person's estimate of the time spent each day harboring obsessive-compulsive thoughts or behaviors, concrete tools can be used to gauge the person's condition. This may be done with rating scales, such as the Yale–Brown Obsessive Compulsive Scale (Y-BOCS; expert rating)[162] or the obsessive-compulsive inventory (OCI-R; self-rating).[163] With measurements such as these, psychiatric consultation can be more appropriately determined, as it has been standardized.[17] In regards to diagnosing, the health professional also looks to make sure that the signs of obsessions and compulsions are not the results of any drugs, prescription or recreational, that the patient may be taking.[164] There are several types of obsessive thoughts that are found commonly in those with OCD. Some of these include fear of germs, hurting loved ones, embarrassment, neatness, societally unacceptable sexual thoughts etc.[164] Within OCD, these specific categories are often diagnosed into their own type of OCD.[2] OCD is sometimes placed in a group of disorders called the obsessive–compulsive spectrum.[165] Another criterion in the DSM is that a person's mental illness does not fit one of the other categories of a mental disorder better. That is to say, if the obsessions and compulsions of a patient could be better described by trichotillomania, it would not be diagnosed as OCD.[2] That being said, OCD does often go hand in hand with other mental disorders. For this reason, one may be diagnosed with multiple mental disorders at once.[166] A different aspect of the diagnoses is the degree of insight had by the individual in regards to the truth of the obsessions. There are three levels, good/fair, poor and absent/delusional. Good/fair indicated that the patient is aware that the obsessions they have are not true or probably not true.[2] Poor indicates that the patient believes their obsessional beliefs are probably true.[2] Absent/delusional indicates that they fully believe their obsessional thoughts to be true.[2] Approximately 4% or fewer individuals with OCD will be diagnosed as absent/delusional.[2] Additionally, as many as 30% of those with OCD also have a lifetime tic disorder, meaning they have been diagnosed with a tic disorder at some point in their life.[2] There are several different types of tics that have been observed in individuals with OCD. These include but are not limited to, "grunting", "jerking" or "shrugging" body parts, sniffling, and excessive blinking.[164] There has been a significant amount of progress over the last few decades, and as of 2022 there is statically significant improvement in the diagnostic process for individuals with OCD. One study found that of two groups of individuals, one with participants under the age of 27.25 and one with participants over that age, those in the younger group experienced a significantly faster time between the onset of OCD tendencies and their formal diagnoses.[167] Differential diagnosis OCD is often confused with the separate condition obsessive–compulsive personality disorder (OCPD). OCD is egodystonic, meaning that the disorder is incompatible with the individual's self-concept.[168][169] As egodystonic disorders go against a person's self-concept, they tend to cause much distress. OCPD, on the other hand, is egosyntonic, marked by the person's acceptance that the characteristics and behaviors displayed as a result are compatible with their self-image, or are otherwise appropriate, correct, or reasonable. As a result, people with OCD are often aware that their behavior is not rational, and are unhappy about their obsessions, but nevertheless feel compelled by them.[170] By contrast, people with OCPD are not aware of anything abnormal; they will readily explain why their actions are rational. It is usually impossible to convince them otherwise, and they tend to derive pleasure from their obsessions or compulsions.[170] |
診断 正式な診断は、心理学者、精神科医、臨床ソーシャルワーカー、その他の資格を持った 精神保健の専門家によって行われます。OCDは、他の精神疾患や行動障害と同様に、医学的な検査で診断することはでき ません[7]。精神障害の診断と統計マニュアル(DSM)によると、OCDと診断されるには、強迫観念、強 迫行為、またはその両方がなければなりません。DSMは、強迫観念や強迫行為が通常の行動から 「臨床的に重要なもの 」になるには、複数の特徴があると指摘しています。患者の日常生活に侵入し、顕著なレベルの不安感を引き起こす反復的で強い考えや衝動がなければならない [2]。 これらの考えや衝動、イメージは、通常の問題に対する心配の範囲外の程度や種類である[161]。OCDの人は、強迫観念を不合理なものとして認識する傾向がある。 強迫観念が臨床的に重要な意味を持つようになるのは、強迫観念に応じて、あるいは厳格に適用されなけれ ばならない規則に従って、強迫観念を実行しなければならないと感じ、その結果、著しい苦痛を感じたり、 引き起こしたりする場合である。従って、OCDでない人の多くがOCDに関連した行動(例えば、パントリーで商品を高さ順 に並べるなど)をとることがありますが、臨床的に重要なOCDとの違いは、OCDを持つ人が 重大な心理的苦痛を避けるためにこれらの行動をとらなければならないという点にあります。これらの行動や精神的行為は、苦痛を予防したり軽減したり、何か 恐ろしい出来事や状況を防いだりすることを目的としていますが、これらの行動は論理的または実際的に問題と関連していないか、または過剰です。 さらに、強迫観念や強迫行為には時間がかかり、1日1時間以上かかることが多いか、 社会的、職業的、学業的機能に障害を引き起こしていることが必要である[161]。強迫観念や強迫行為に毎日費やす時間を本人が推定することに加え、具体 的な道具を 用いることで、その人の状態を測定することができます。これには、イェール・ブラウン強迫尺度(Y-BOCS;専門家評価)[162]や強迫目録(OCI -R;自己評価)[163]などの評価尺度を用いることができる。このような測定法を用いれば、標準化されているため、精神科受診をより適切に判断するこ とができる[17]。 診断に関して、医療専門家はまた、強迫観念や強迫行為の徴候が、患者が服用している可能性のある薬物(処方薬、娯楽薬など)の結果ではないことを確認する[164]。 OCD患者によく見られる強迫観念にはいくつかの種類があります。その中には、細菌に対する恐怖、愛する人を傷つけ ること、恥ずかしさ、綺麗好き、社会的に許容されない性的な考えなどがあります[164]。 OCDは強迫スペクトラムと呼ばれる疾患群に分類されることもあります[165]。 DSMのもう1つの基準は、その人の精神疾患が他の精神疾患のカテゴリーに当てはまらな いことです。つまり、もしある患者の強迫観念や強迫行為がトリコチロマニアに当ては まる場合、OCDと診断されることはありません。そのため、一度に複数の精神障害と診断されることもあります[166]。 診断の異なる側面は、強迫観念の真相に関して個人が持っている洞察力の度合いです。3つのレベル、良い/まあまあ、悪い、不在/妄想がある。良い/まあ良 いは、患者が自分の強迫観念が真実でないか、おそらく真実でないと自覚していることを示す[2]。悪い/まあ良いは、患者が自分の強迫観念はおそらく真実 であると信じていることを示す[2]。 [2]また、OCD患者の約30%は生涯チック障害を患っており、これは人生のある時点でチック障害と診断されたことを意味する[2]。 OCD患者にみられるチックにはいくつかの種類があります。これには、「うなり声」、「身じろぎ」、「鼻をすする」、「過剰なまばたき」などが含まれますが、これらに限定されるものではありません[164]。 ここ数十年の間に大きな進歩があり、2022年現在、OCD患者の診断プロセスには静的 に大きな改善が見られます。ある研究によると、27.25歳以下と27.25歳以上の2つのグループにおいて、若年層はOCD傾向の 発症から正式な診断までの期間が有意に早かったことが報告されています[167]。 鑑別診断 OCDはしばしば強迫性パーソナリティ障害(OCPD)と混同されます。OCDは自我強迫性障害であり、これはその障害が個人の自己概念と相容れないこと を意味する[168][169]。一方、OCPDは自我統 合的であり、その結果として示される特徴や行動が自己イメージと適合している、 あるいは適切である、正しい、または合理的であると本人が受け入れていることが 特徴である。 その結果、OCDの人はしばしば自分の行動が理性的でないことを自覚し、強迫観念を 不快に思いながらも、それにもかかわらず、強迫観念に駆られてしまう。そうでないと納得させることは通常不可能であり、強迫観念や強迫行為から喜びを得る傾向がある[170]。 |
| Management Cognitive behavioral therapy (CBT) and psychotropic medications are the first-line treatments for OCD.[1][171] Therapy One exposure and ritual prevention activity would be to check the lock only once and then leave. One specific CBT technique used is called exposure and response prevention (ERP), which involves teaching the person to deliberately come into contact with situations that trigger obsessive thoughts and fears (exposure), without carrying out the usual compulsive acts associated with the obsession (response prevention). This technique causes patients to gradually learn to tolerate the discomfort and anxiety associated with not performing their compulsions. For many patients, ERP is the add-on treatment of choice when selective serotonin reuptake inhibitors (SSRIs) or serotonin-norepinephrine reuptake inhibitors (SNRIs) medication does not effectively treat OCD symptoms, or vice versa, for individuals who begin treatment with psychotherapy.[21]This technique is considered superior to others due to the lack of medication used. However, up to 25% of patients will discontinue treatment due to the severity of their tics. CBT normally lasts anywhere from 12-16 sessions, with homework assigned to the patient in between meetings with a therapist. (Lack 2012). Modalities differ in ERP treatment but both virtual reality based as well as unguided computer assisted treatment programs have shown effective results in treatment programs.[172][173] For example, a patient might be asked to touch something very mildly contaminated (exposure), and wash their hands only once afterward (response prevention). Another example might entail asking the patient to leave the house and check the lock only once (exposure), without going back to check again (response prevention). After succeeding at one stage of treatment, the patient's level of discomfort in the exposure phase can be increased. When this therapy is successful, the patient will quickly habituate to an anxiety-producing situation, discovering a considerable drop in anxiety level.[174] ERP has a strong evidence base, and is considered the most effective treatment for OCD.[174] However, this claim was doubted by some researchers in 2000, who criticized the quality of many studies.[175] While ERP can lead a majority of clients to improvements, many do not reach remission or become asymptomatic;[176] some therapists are also hesitant to use this approach.[177] The recent development of remotely technology-delivered CBT is increasing access to therapy options for those living with OCD and remote versions appear to equally as effective as in-person therapy options. The development of smartphone interventions for OCD that utilize CBT techniques are another alternative that is expanding access to therapy while allowing therapies to be personalized for each patient.[178] Acceptance and commitment therapy (ACT), a newer therapy also used to treat anxiety and depression, has also been found to be effective in treatment of OCD.[179][180] ACT uses acceptance and mindfulness strategies to teach patients not to overreact to or avoid unpleasant thoughts and feelings but rather "move toward valued behavior."[181][182] Inference-based therapy (IBT) is a form of cognitive therapy specifically developed for treating OCD.[183] The therapy posits that individuals with OCD put a greater emphasis on an imagined possibility than on what can be perceived with the senses, and confuse the imagined possibility with reality, in a process called inferential confusion.[184] According to inference-based therapy, obsessional thinking occurs when the person replaces reality and real probabilities with imagined possibilities.[185] The goal of inference-based therapy is to reorient clients towards trusting the senses and relating to reality in a normal, non-effortful way. Differences between normal and obsessional doubts are presented, and clients are encouraged to use their senses and reasoning as they do in non-obsessive-compulsive disorder situations.[186][183] Research on Inference-Based Cognitive-Behavior Therapy (I-CBT) suggests it can lead to improvements for those with OCD.[187] A 2007 Cochrane review found that psychological interventions derived from CBT models, such as ERP, ACT, and IBT, were more effective than non-CBT interventions.[26] Other forms of psychotherapy, such as psychodynamics and psychoanalysis, may help in managing some aspects of the disorder. However, in 2007, the American Psychiatric Association (APA) noted a lack of controlled studies showing their efficacy, "in dealing with the core symptoms of OCD."[188] For body-focused repetitive behaviors (BFRB), behavioral interventions such as habit-reversal training and decoupling are recommended.[67][68] Psychotherapy in combination with psychiatric medication may be more effective than either option alone for individuals with severe OCD.[189][190][191] ERP coupled with weight restoration and serotonin reuptake inhibitors has proven the most effective when treating OCD and an eating disorder simultaneously.[192] Medication A blister pack of sertraline under the brand name Zoloft The medications most frequently used to treat OCD are antidepressants, including selective serotonin reuptake inhibitors (SSRIs) and serotonin-norepinephrine reuptake inhibitors (SNRIs).[4] Sertraline and fluoxetine are effective in treating OCD for children and adolescents.[193][194][195] SSRIs help people with OCD by inhibiting the reabsorption of serotonin by the nerve cells after they carry messages from neurons to synapse; thus, more serotonin is available to pass further messages between nearby nerve cells.[129] SSRIs are a second-line treatment of adult OCD with mild functional impairment, and as first-line treatment for those with moderate or severe impairment. In children, SSRIs can be considered as a second-line therapy in those with moderate to severe impairment, with close monitoring for psychiatric adverse effects.[171] Patients treated with SSRIs are about twice as likely to respond to treatment as are those treated with placebo, so this treatment is qualified as efficacious.[196][197] Efficacy has been demonstrated both in short-term (6–24 weeks) treatment trials, and in discontinuation trials with durations of 28–52 weeks.[198][199][200] Clomipramine, a medication belonging to the class of tricyclic antidepressants, appears to work as well as SSRIs, but has a higher rate of side effects.[4] In 2006, the National Institute for Health and Care Excellence (NICE) guidelines recommended augmentative second-generation (atypical) antipsychotics for treatment-resistant OCD.[5] Atypical antipsychotics are not useful when used alone, and no evidence supports the use of first-generation antipsychotics.[28][201] For OCD treatment specifically, there is tentative evidence for risperidone, and insufficient evidence for olanzapine. Quetiapine is no better than placebo with regard to primary outcomes, but small effects were found in terms of Y-BOCS score. The efficacy of quetiapine and olanzapine are limited by an insufficient number of studies.[202] A 2014 review article found two studies that indicated that aripiprazole was "effective in the short-term", and found that "[t]here was a small effect-size for risperidone or anti-psychotics in general in the short-term"; however, the study authors found "no evidence for the effectiveness of quetiapine or olanzapine in comparison to placebo."[5] While quetiapine may be useful when used in addition to an SSRI/SNRI in treatment-resistant OCD, these drugs are often poorly tolerated, and have metabolic side effects that limit their use. A guideline by the American Psychological Association suggested that dextroamphetamine may be considered by itself after more well-supported treatments have been attempted.[203] Procedures Electroconvulsive therapy (ECT) has been found to have effectiveness in some severe and refractory cases.[204] Transcranial magnetic stimulation has shown to provide therapeutic benefits in alleviating symptoms.[205] Surgery may be used as a last resort in people who do not improve with other treatments. In this procedure, a surgical lesion is made in an area of the brain (the cingulate cortex). In one study, 30% of participants benefitted significantly from this procedure.[206] Deep brain stimulation and vagus nerve stimulation are possible surgical options that do not require destruction of brain tissue. However, because deep brain stimulation results in such an instant and intense change, individuals may experience identity challenges afterward.[207] In the United States, the Food and Drug Administration approved deep-brain stimulation for the treatment of OCD under a humanitarian device exemption, requiring that the procedure be performed only in a hospital with special qualifications to do so.[208] In the United States, psychosurgery for OCD is a treatment of last resort, and will not be performed until the person has failed several attempts at medication (at the full dosage) with augmentation, and many months of intensive cognitive–behavioral therapy with exposure and ritual/response prevention.[209] Likewise, in the United Kingdom, psychosurgery cannot be performed unless a course of treatment from a suitably qualified cognitive–behavioral therapist has been carried out. Children Therapeutic treatment may be effective in reducing ritual behaviors of OCD for children and adolescents.[210] Similar to the treatment of adults with OCD, cognitive behavioral therapy stands as an effective and validated first line of treatment of OCD in children.[211] Family involvement, in the form of behavioral observations and reports, is a key component to the success of such treatments.[212] Parental interventions also provide positive reinforcement for a child who exhibits appropriate behaviors as alternatives to compulsive responses. In a recent meta-analysis of evidenced-based treatment of OCD in children, family-focused individual CBT was labeled as "probably efficacious," establishing it as one of the leading psychosocial treatments for youth with OCD.[211] After one or two years of therapy, in which a child learns the nature of their obsession and acquires strategies for coping, they may acquire a larger circle of friends, exhibit less shyness, and become less self-critical.[213] Trials have shown that children and adolescents with OCD should begin treatment with the combination of CBT with a selective serotonin reuptake inhibitor or CBT alone, rather than only an SSRI.[93][95] Although the known causes of OCD in younger age groups range from brain abnormalities to psychological preoccupations, life stress such as bullying and traumatic familial deaths may also contribute to childhood cases of OCD, and acknowledging these stressors can play a role in treating the disorder.[214] |
マネジメント 認知行動療法(CBT)と向精神薬がOCDの第一選択治療である[1][171]。 治療 暴露と儀式による予防の1つの方法は、鍵を1度だけ確認し、その場を離れることであ る。 具体的なCBTの技法の1つに暴露反応妨害法(ERP)と呼ばれるものがあり、強迫観念や恐怖の引き金となる状況に意図的に接触し(暴露)、強迫観念と関 連する通常の強迫行為を行わない(反応妨害)ように指導するものです。この手法により、患者は強迫行為を行わないことに伴う不快感や不安に耐えることを徐 々に学んでいく。多くの患者にとってERPは、選択的セロトニン再取り込み阻害薬(SSRI)やセロトニン・ノルエピネフリン再取り込み阻害薬 (SNRI)による薬物療法がOCD症状を効果的に治療できない場合、またはその逆で、精神療法による治療を開始する場合に選択される追加的治療法である [21]。この技法は薬物療法を用いないため、他の技法よりも優れていると考えられている。しかし、患者の25%まではチックの重症度により治療を中断す る。CBTは通常12~16回のセッションで行われ、セラピストとの面談の合間に宿題が出される。(Lack 2012)。ERP治療ではモダリティが異なるが、バーチャルリアリティベースの治療プログラムも、ガイドなしのコンピュータ支援治療プログラムも、治療 プログラムにおいて効果的な結果を示している [172] [173] 。 例えば、患者にごく軽度の汚染物に触れてもらい(曝露)、その後1回だけ手を洗う(反応予防)。別の例では、患者に家を出て鍵を1回だけ確認し(曝露)、 再度確認に戻ることはしないよう求めることもある(反応予防)。ある段階の治療が成功したら、暴露段階における患者の不快のレベルを上げることができる。 この療法が成功すると、患者は不安を引き起こす状況に対してすぐに慣れるようになり、不安レベルがかなり低下することを発見する [174] 。 ERPには強力なエビデンスがあり、OCDに最も効果的な治療法と考えられている[174]が、この主張は2000年に一部の研究者によって疑問視され、 多くの研究の質を批判された[175]。 ERPは大多数のクライエントを改善に導くことができるが、多くのクライエントは寛解に至らなかったり、無症状になったりする[176];また、このアプ ローチの使用をためらうセラピストもいる[177]。 最近、遠隔技術によるCBTが開発され、OCDを抱える人々への治療法の選択肢が増えつつあ り、遠隔療法は対面療法と同様に有効であると考えられています。CBTの技法を利用したOCDに対するスマートフォンによる介入法の開発は、治療へのア クセスを拡大するもう一つの選択肢であり、各患者に合わせた治療を可能にするものであ る[178]。 アクセプタンス&コミットメント療法(ACT)は、不安やうつ病の治療にも使われる新しい療法で、 OCDの治療にも有効であることが分かっています[179][180]。ACTはアクセプタンスとマインドフルネス の戦略を用いて、患者に不快な考えや感情に過剰に反応したり、避けたりするのではなく、 「価値ある行動に向かう」ことを教えます[181][182]。 推論に基づく療法(IBT)は、OCDを治療するために特別に開発された認知療法の一種です [183] 。 [184] 推論に基づく療法によると、強迫観念による思考は、現実や現実の可能 性を想像上の可能性に置き換えてしまうことで生じる。正常な疑い と強迫的な疑いとの違いが提示され、クライエントは強迫性障害でない状況と同じ ように感覚と推論を使うように勧められる[186][183]。 2007年のコクラン・レビューによると、ERP、ACT、IBTなどのCBTモデルから派生した心理的介入は、非CBTの介入よりも効果的であることが 判明している[26]。しかしながら、2007年に米国精神医学会(APA)は、「OCDの中核的な症状に対処する上で」その有効性を示す対照研究が不足 していることを指摘している[188]。身体焦点反復行動(BFRB)に対しては、習慣逆転訓練やデカップリングなどの行動介入が推奨されている[67] [68]。 精神療法と精神科の薬物療法を併用することは、重度のOCD患者にはどちらか一方を単独で行 うよりも効果的である[189][190][191]。OCDと摂食障害を同時に治療する場合、体重回復とセロトニン再取り込 み阻害薬を併用したERPが最も効果的であることが証明されている[192]。 薬物療法 Zoloftの商品名で販売されているセルトラリンのブリスターパック。 選択的セロトニン再取り込み阻害薬(SSRI)やセロトニン・ノルエピネフリン再取り込 み阻害薬(SNRI)を含む抗うつ薬[4]は、小児や青少年のOCD治療に効果的です[193][194][195]。 SSRIは神経細胞からシナプスにメッセージを伝達した後の神経細胞によるセロトニンの再吸収を阻害することにより、OCDの患者を助けます。 SSRIは軽度の機能障害を持つ成人のOCDの第二選択薬であり、中等度または重度の機能障害を持つOCDの第一選択薬である。小児では、SSRIは精神 医学的副作用を注意深く観察しながら、中等度から重度の機能障害を有する患者の第二選択治療として考慮されうる[171]。SSRIで治療された患者は、 プラセボで治療された患者の約2倍の確率で治療に反応するので、この治療は有効であると認められる[196][197]。 有効性は、短期(6~24週間)の治療試験でも、28~52週間の中止試験でも証明されている[198][199][200]。 三環系抗うつ薬の一種であるクロミプラミンは、SSRIと同様に効果があるように見えるが、副作用の発生率が高い[4]。 2006年、National Institute for Health and Care Excellence (NICE)のガイドラインは、治療抵抗性強迫性障害に対する第二世代(非定型)抗精神病薬の補強を推奨している[5]。非定型抗精神病薬は単独で使用し ても有用ではなく、第一世代抗精神病薬の使用を支持するエビデンスはない[28][201]。クエチアピンは主要アウトカムに関してはプラセボより優れて いないが、Y-BOCSスコアに関しては小さな効果が認められた。クエチアピンとオランザピンの有効性については、研究数が不十分であるため限定的である [202]。2014年の総説では、アリピプラゾールが「短期的に有効」であることを示した2件の研究が見つかり、「短期的にはリスペリドンまたは抗精神 病薬全般の効果サイズが小さい」ことがわかったが、研究著者は「プラセボと比較してクエチアピンまたはオランザピンの有効性を示す証拠はない」とした [5]。 「クエチアピンは治療抵抗性OCDにおいてSSRI/SNRIと併用することで有用となる可能性がありますが、これらの薬剤はしばしば忍容性が低く、代謝 性の副作用があるため使用が制限されます。アメリカ心理学会のガイドラインでは、より支持の高い治療が試みられた後に、デキストロアンフェタミンを単独で 考慮することが示唆されている[203]。 手続き 電気けいれん療法(ECT)は、一部の重症で難治性の症例に有効であることがわかっている[204]。 経頭蓋磁気刺激は、症状の緩和において治療効果があることが示されている[205]。 手術は、他の治療で改善しない人の最後の手段として用いられることがある。この方法では、脳の領域(帯状皮質)に外科的病変を作る。脳深部刺激と迷走神経 刺激は、脳組織の破壊を必要としない可能性のある外科的選択肢である。しかし、脳深部刺激療法は瞬時に強い変化をもたらすため、その後にアイデンティテ ィの問題を経験する可能性がある[207]。米国では、食品医薬品局が人道的器具免除のもとでOCDの治療に脳深 部刺激療法を承認しており、この処置は特別な資格を有する病院でのみ実施されるこ とを求めている[208]。 同様にイギリスでは、適切な資格を持った認知行動療法士による治療が行われない限り、精神 手術を行うことはできない[209]。 子ども 成人のOCD治療と同様に、認知行動療法は小児のOCD治療の第一選択として有効であ ると認められています[211]。行動観察や報告という形での家族の関与は、このような治療の成 功にとって重要な要素です[212]。子供のOCD治療に関する最近のメタアナリシスでは、家族中心の個人CBTは「おそらく効 果的である」とされ、OCDを持つ青少年に対する主要な心理社会的治療法の1つであるとされてい る。 [211] 治療を1~2年続け、強迫観念の本質を知り、対処の戦略を身につけると、友達の輪が広がり、内気な性格が減り、自己批判が少なくなる[213]。 低年齢層におけるOCDの原因として知られているものは、脳の異常から心理的なこだわりまで多岐にわたりますが、いじめやトラウマとなるような家族の死な どの生活上のストレスも小児期のOCDの一因である可能性があり、これらのストレス因子を認めることが障害の治療に一役買う可能性があります[214]。 |
| Prognosis Quality of life is reduced across all domains in OCD. While psychological or pharmacological treatment can lead to a reduction of OCD symptoms and an increase in reported quality of life, symptoms may persist at moderate levels even following adequate treatment courses, and completely symptom-free periods are uncommon.[215][216] In pediatric OCD, around 40% still have the disorder in adulthood, and around 40% qualify for remission.[217] The risk of having at least one comorbid personality disorder in OCD is 52%, which is the highest among anxiety disorders and greatly impacts its management and prognosis.[218] |
予後 OCDのQOLは全ての領域で低下する。心理学的または薬理学的治療により、OCDの症状が軽減し、生活の質が向上すると報告されてい るが、十分な治療を受けても症状が中等度のレベルで持続することがあり、完全に無症状の期間は稀であ る[215][216]。小児OCDでは、約40%が成人期になっても障害を有し、約40%が寛解の資格を有する[217]。 OCDに少なくとも1つの人格障害が併存するリスクは52%であり、これは不安障害の中で最も高く、その管理と予後に大きく影響する[218]。 |
| Epidemiology Further information: Delayed-maturation theory of obsessive–compulsive disorder 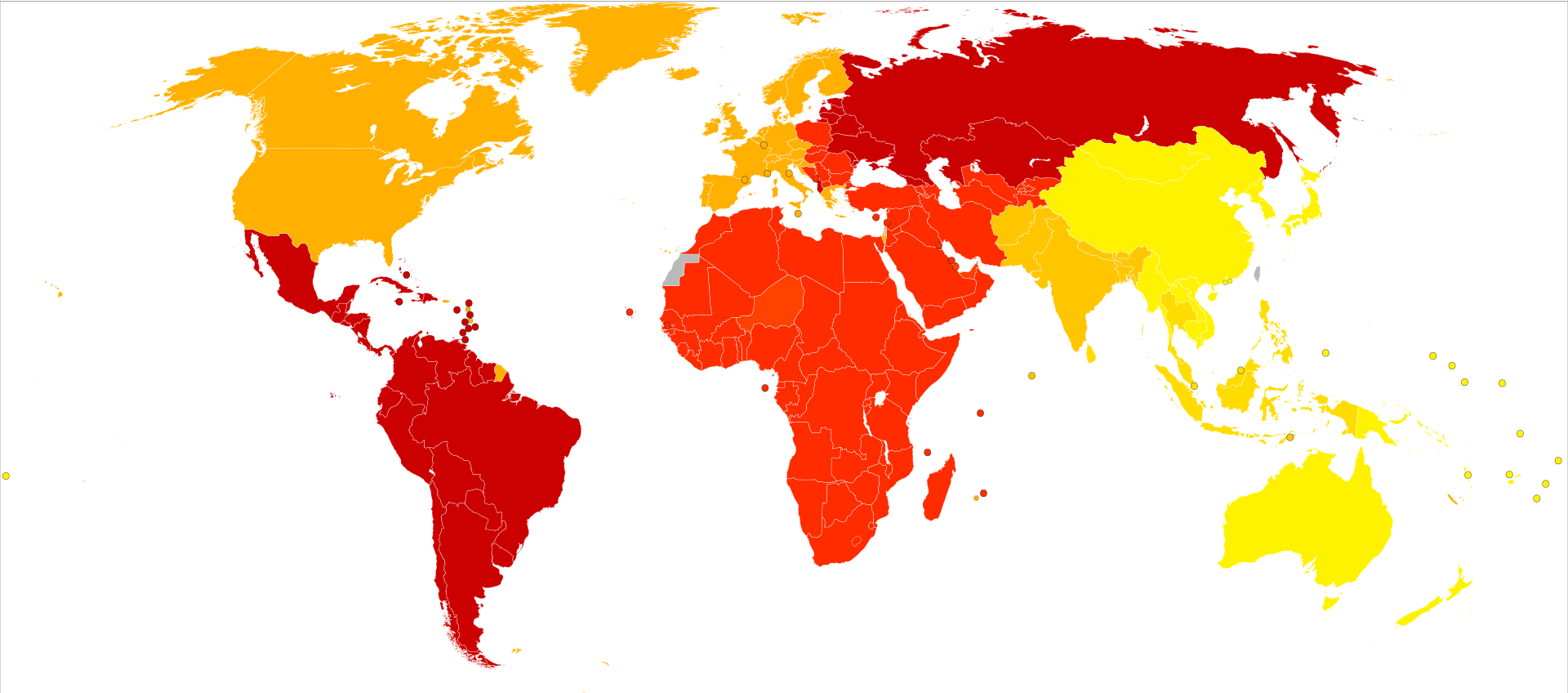 Age-standardized disability-adjusted life year estimated rates for obsessive-compulsive disorder per 100,000 inhabitants in 2004  Obsessive–compulsive disorder affects about 2.3% of people at some point in their life, with the yearly rate about 1.2%.[6] OCD occurs worldwide.[2] It is unusual for symptoms to begin after the age of 35 and half of people develop problems before 20.[1][2] Males and females are affected about equally.[1] However, there is an earlier age for onset for males than females.[219] |
疫学さらに詳しい情報 強迫性障害の成熟遅延理論 2004年における人口10万人当たりの強迫性障害の年齢標準化障害調整生存年推定値 強迫性障害は、約2.3%の人が人生のある時点で罹患し、年間罹患率は約1.2%である[6]。強迫性障害は世界中で発症する[2]。35歳以降に症状が 始まるのは珍しく、半数の人が20歳前に問題を発症する[1][2]。男性と女性がほぼ同じように罹患する[1]。しかし、男性の方が女性よりも発症年齢 が早い[219]。 |
| History Plutarch, an ancient Greek philosopher and historian, describes an ancient Roman man who possibly had scrupulosity, which could be a symptom of OCD or OCPD. This man is described as "turning pale under his crown of flowers," praying with a "faltering voice," and scattering "incense with trembling hands."[220][221][222] In the 7th century AD, John Climacus records an instance of a young monk plagued by constant and overwhelming "temptations to blasphemy" consulting an older monk, who told him: "My son, I take upon myself all the sins which these temptations have led you, or may lead you, to commit. All I require of you is that for the future you pay no attention to them whatsoever."[223]: 212 The Cloud of Unknowing, a Christian mystical text from the late 14th century, recommends dealing with recurring obsessions by attempting to ignore them, and, if that fails, to "cower under them like a poor wretch and a coward overcome in battle, and reckon it to be a waste of your time for you to strive any longer against them", a technique now known as emotional flooding.[223]: 213 Abu Zayd Al-Balkhi, the 9th century Islamic polymath, was likely the first to classify OCD into different types and pioneer cognitive behavioral therapy, in a fashion unique to his era and which was not popular in Greek medicine.[224] In his medical treatise entitled Sustenance of the Body and Soul, Al-Balkhi describes obsessions particular to the disorder as "Annoying thoughts that are not real. These intrusive thoughts prevent enjoying life, and performing daily activities. They affect concentration and interfere with ability to carry out different tasks."[225] As treatment, Al-Balkhi suggests treating obsessive thoughts with positive thoughts and mind-based therapy.[224] From the 14th to the 16th century in Europe, it was believed that people who experienced blasphemous, sexual or other obsessive thoughts were possessed by the devil.[168][223]: 213 Based on this reasoning, treatment involved banishing the "evil" from the "possessed" person through exorcism.[226][227] The vast majority of people who thought that they were possessed by the devil did not have hallucinations or other "spectacular symptoms" but "complained of anxiety, religious fears, and evil thoughts."[223]: 213 In 1584, a woman from Kent, England, named Mrs. Davie, described by a justice of the peace as "a good wife", was nearly burned at the stake after she confessed that she experienced constant, unwanted urges to murder her family.[223]: 213 The English term obsessive–compulsive arose as a translation of German Zwangsvorstellung (obsession) used in the first conceptions of OCD by Karl Westphal. Westphal's description went on to influence Pierre Janet, who further documented features of OCD.[71] In the early 1910s, Sigmund Freud attributed obsessive–compulsive behavior to unconscious conflicts that manifest as symptoms.[226] Freud describes the clinical history of a typical case of "touching phobia" as starting in early childhood, when the person has a strong desire to touch an item. In response, the person develops an "external prohibition" against this type of touching. However, this "prohibition does not succeed in abolishing" the desire to touch; all it can do is repress the desire and "force it into the unconscious."[228] Freudian psychoanalysis remained the dominant treatment for OCD until the mid-1980s, even though medicinal and therapeutic treatments were known and available, because it was widely thought that these treatments would be detrimental to the effectiveness of the psychotherapy.[223]: 210–211 In the mid-1980s, this approach changed, and practitioners began treating OCD primarily with medicine and practical therapy rather than through psychoanalysis.[223]: 210 One of the first successful treatments of OCD, exposure and response prevention, emerged during the 1960s, when psychologist Vic Meyer exposed two hospitalized patients to anxiety-inducing situations while preventing them from performing any compulsions. Eventually, both patients' anxiety level dropped to manageable levels. Meyer devised this procedure from his analysis of fear extinguishment in animals via flooding.[229] The success of ERP clinically and scientifically has been summarized as "spectacular" by prominent OCD researcher Stanley Rachman decades following Meyer's creation of the method.[230] In 1967, psychiatrist Juan José López-Ibor reported that the drug clomipramine was effective in treating OCD. Many reports of its success in treatment followed, and several studies had confirmed its effectiveness by the 1980s.[231][232] However, clomipramine was subsequently displaced by new SSRIs developed in the 1970s, such as fluoxetine and sertraline, which were shown to have less side effects.[4][232] Obsessive-compulsive symptoms worsened during the early stages of the COVID-19 pandemic, particularly for individuals with contamination-related OCD.[233] Notable cases John Bunyan (1628–1688), the author of The Pilgrim's Progress, displayed symptoms of OCD (which had not yet been named). During the most severe period of his condition, he would mutter the same phrase over and over again to himself while rocking back and forth.[223]: 53–54 He later described his obsessions in his autobiography Grace Abounding to the Chief of Sinners, stating, "These things may seem ridiculous to others, even as ridiculous as they were in themselves, but to me they were the most tormenting cogitations."[223]: 53–54 He wrote two pamphlets advising those with similar anxieties.[223]: 217–218 In one of them, he warns against indulging in compulsions: "Have care of putting off your trouble of spirit in the wrong way: by promising to reform yourself and lead a new life, by your performances or duties".[223]: 217–218 British poet, essayist and lexicographer Samuel Johnson (1709–1784) also had OCD. He had elaborate rituals for crossing the thresholds of doorways, and repeatedly walked up and down staircases counting the steps.[234][223]: 54–55 He would touch every post on the street as he walked past, only step in the middle of paving stones, and repeatedly perform tasks as though they had not been done properly the first time.[223]: 55 The "Rat Man", real name Ernst Lanzer, a notable patient of Sigmund Freud, suffered from what was then called "obsessional neurosis". Lanzer's illness was characterised most famously by a pattern of distressing intrusive thoughts in which he feared that his father or a female friend would be subjected to a purported Chinese method of torture in which rats would be encouraged to gnaw their way out of a victim's body by a hot poker.[235] American aviator and filmmaker Howard Hughes is known to have had OCD, primarily an obsessive fear of germs and contamination.[236] Friends of Hughes have also mentioned his obsession with minor flaws in clothing.[237] This was conveyed in The Aviator (2004), a film biography of Hughes.[238] English singer-songwriter George Ezra has openly spoken about his life-long struggle with OCD, particularly primarily obsessional obsessive–compulsive disorder (Pure O).[239] World renowned Swedish climate activist Greta Thunberg is also known to have OCD, among other mental health conditions.[240] American actor James Spader has also spoken about his OCD. In 2014, when interviewed for Rolling Stone he said: "I'm obsessive-compulsive. I have very, very strong obsessive-compulsive issues. I'm very particular. ... It's very hard for me, you know? It makes you very addictive in behavior, because routine and ritual become entrenched. But in work, it manifests itself in obsessive attention to detail and fixation. It serves my work very well: Things don't slip by. But I'm not very easygoing.[241] In 2022 the president of Chile Gabriel Boric stated that he had OCD, saying: "I have an obsessive–compulsive disorder that's completely under control. Thank God I've been able to undergo treatment and it doesn't make me unable to carry out my responsibilities as the President of the Republic."[242] In a documentary released in 2023, David Beckham shared details about his compelling cleaning rituals, need for symmetry in the fridge, and the impact of OCD on his life.[243] |
歴史 古代ギリシアの哲学者であり歴史家であるプルタークは、OCDやOCPDの症状である可能性のある几帳面さを持っていた古代ローマの男性について記述して いる。この人物は「花冠の下で青ざめ」、「たどたどしい声」で祈り、「震える手で線香」を撒いたと記述されている[220][221][222]。 紀元7世紀、ヨハネ・クリマコスは、絶え間ない圧倒的な「神を冒涜する誘惑」に悩まされた若い修道士が、年長の修道士に相談した例を記録している: 「私の息子よ、これらの誘惑があなたを導いた、あるいは導くかもしれないすべての罪を私が引き受ける。私があなたに要求するのは、将来にわたって、あなた がそれらに一切注意を払わないことである」[223]: 212 14世紀後半に書かれたキリスト教の神秘主義書である『無明の雲』では、繰り返される強迫観念への対処法として、それを無視しようと試みること、そしてそ れが失敗した場合には、「戦いに打ち勝った哀れな臆病者のように、それらに屈服し、それ以上それらに向かって努力することは時間の無駄であると考える」こ とを勧めている。 9世紀のイスラムの多才な人物であるアブ・ザイド・アル=バルキーは、ギリシャ医学では一般的でなかった、彼の時代特有の方法で、強迫性障害を様々なタイ プに分類し、認知行動療法を開拓した最初の人物と思われる[224]。このような侵入的思考は、人生を楽しんだり、日常生活を営んだりすることを妨げる。 強迫観念は集中力に影響を及ぼし、さまざまな仕事を遂行する能力を妨げる」[225]。治療法として、アル=バルキーは、強迫観念を肯定的な思考と心に基 づく療法で治療することを提案している[224]。 ヨーロッパでは14世紀から16世紀にかけて、冒涜的な考えや性的な考え、その他の強迫観念を経験する人は悪魔に取り憑かれていると信じられていた [168][223]: 213 この推論に基づいて、治療には悪魔祓いによって「取り憑かれている」人から「悪」を追放することが必要であった。 [226][227] 悪魔に憑依されていると考える人々の大多数は、幻覚や他の「壮大な症状」を持たなかったが、「不安、宗教的な恐怖、邪悪な考えを訴えた」[223]: 213 1584年、イングランドのケント州に住むデヴィ夫人という名の女性は、治安判事から「良妻賢母」と評されたが、自分の家族を殺したいという不本意な衝動 を常に経験していると告白した後、火あぶりにされそうになった[223]: 213。 強迫性という英語は、カール・ヴェストファーによる強迫性障害の最初の概念で使われたドイツ語のZwangsvorstellung(強迫観念)の翻訳と して生まれた。1910年代初頭、ジークムント・フロイトは強迫行為を、症状として現れる無意識の葛藤に起因するとした[226]。それに対して、人はこ の種の接触に対する「外的な禁止」を発達させる。しかし、この「禁止は、触りたいという欲求をなくすことには成功しない」のであり、できるのは欲求を抑圧 し、「無意識の中に強制的に押し込める」ことだけである。 [223]: 210-211 1980年代半ばになると、このアプローチは変化し、開業医は精神分析を通 じてではなく、主に薬や実践的な療法によってOCDを治療するようになりました。 1960年代、心理学者であるヴィック・マイヤーが、入院中の2人の患者に強迫行為をさせ ないようにしながら、不安を誘発する状況にさらしました。最終的に、2人の患者の不安レベルは管理可能なレベルまで低下した。マイヤーは、フラッディング による動物の恐怖消滅の分析からこの方法を考案し た[229]。ERPの臨床的・科学的な成功は、マイヤーがこの方法を考案してから数十年 後、著名な強迫性障害の研究者であるスタンリー・ラックマンによって「目を見張るよ うな」と要約されている[230]。 1967年、精神科医ホアン・ホセ・ロペス-イボルは、クロミプラミンがOCDの治療に有 効であることを報告しました。その後、治療に成功したという多くの報告がなされ、1980年代までにいくつかの研究でその有効性が確認されました [231][232]。しかし、クロミプラミンはその後、1970年代に開発されたフルオキセチンやセルトラリンなどの新しいSSRIに取って代わられ、 より副作用が少ないことが示されました[4][232]。 強迫症状は、COVID-19のパンデミックの初期段階において、特に汚染に関連したOCDの患者において悪化した[233]。 著名な症例 巡礼の道』の作者であるジョン・バニヤン(1628-1688)は、OCDの症状を示していた。最も重篤な時期には、体を前後に揺らしながら、同じフレー ズを何度も何度も独り言のように呟いていた[223]: 53-54 彼は後に自伝『罪人の長にあふれる恩寵』の中で、自分の強迫観念についてこう述べている。「これらのことは、他の人々にはばかばかしく思えるかもしれな い: 53-54 彼は、同じような不安を抱えた人々に助言する2つの小冊子を書いた[223]: 217-218 そのうちの1つで、彼は強迫観念に耽ることを戒めている: 「精神的な悩みを間違った方法で先送りにしないように気をつけなさい:自分を改め、新しい生活を送ると約束することで、演技や義務によって」[223]: 217-218 イギリスの詩人、エッセイスト、辞書学者であるサミュエル・ジョンソン(1709-1784)も強迫性障害であった。彼は玄関の敷居をまたぐときに入念な 儀式を行い、階段の段数を数えて繰り返し上り下りした[234][223]: 54-55 彼は通り過ぎるときにすべての道にある柱に触れ、敷石の真ん中しか踏まず、一度目はきちんとできていなかったかのように繰り返し仕事をこなした [223]: 55 ネズミ男」、本名エルンスト・ランツァーは、ジークムント・フロイトの著名な患者で、当時「強迫神経症」と呼ばれていたものに苦しんでいた。ランツァーの 病気が最も有名なのは、父親や女性の友人が、中国の拷問方法とされる、熱い火かき棒でネズミを齧らせ、被害者の体からネズミを出すという拷問を受けるので はないかと恐れる、苦痛を伴う侵入思考のパターンであった[235]。 アメリカの飛行家で映画監督のハワード・ヒューズは強迫性障害であったことが知られており、主に細菌や汚染に対する強迫的な恐怖を抱いていた[236]。 ヒューズの友人たちは、ヒューズが衣服の些細な欠陥に執着していたことにも言及している[237]。 これはヒューズの伝記映画である『アビエイター』(2004年)で伝えられている[238]。 イギリスのシンガーソングライター、ジョージ・エズラは、OCD、特に主に強迫性強迫性障害(Pure O)との生涯の闘いについて公然と語っている[239]。 世界的に有名なスウェーデンの気候活動家グレタ・トゥンバーグもまた、他の精神疾患の中でもOCDを患っていることで知られている[240]。 アメリカの俳優ジェームズ・スペイダーも強迫性障害について話している。2014年、『ローリング・ストーン』のインタビューを受けた際、彼はこう語って いる: 「僕は強迫性障害なんだ。とても強い強迫観念があるんだ。こだわりが強いんだ。とても辛いんだ。ルーティンや儀式が定着してしまうから。でも仕事では、細 部への強迫的なこだわりや執着という形で現れる。それは私の仕事にとても役立っている: 物事がすり抜けることがない。でも、私はのんびり屋ではないのです」[241]。 2022年、チリのガブリエル・ボリック大統領は、自分が強迫性障害であることを明言し、次のように述べた: 「強迫性障害は完全にコントロールできている。治療を受けることができ、共和国大統領としての責任を果たすことができないわけではないことを神に感謝しま す」[242]。 2023年に公開されたドキュメンタリーの中で、デビッド・ベッカムは、彼の強迫的な掃除の儀式、冷蔵庫内の対称性の必要性、強迫神経症が彼の人生に与えた影響についての詳細を語った[243]。 |
Society and culture This ribbon represents trichotillomania and other body-focused repetitive behaviors. Art, entertainment and media Movies and television shows may portray idealized or incomplete representations of disorders such as OCD.[244] Compassionate and accurate literary and on-screen depictions may help counteract the potential stigma associated with an OCD diagnosis, and lead to increased public awareness, understanding and sympathy for such disorders.[245][246] The play and film adaptations of The Odd Couple based around the character of Felix, who shows some of the common symptoms of OCD.[247] In the film As Good as It Gets (1997), actor Jack Nicholson portrays a man with OCD who performs ritualistic behaviors that disrupt his life.[248] The film Matchstick Men (2003) portrays a con man named Roy (Nicolas Cage) with OCD who opens and closes doors three times while counting aloud before he can walk through them.[249] In the television series Monk (2002–2009), the titular character Adrian Monk fears both human contact and dirt.[250][251] The one-man show The Life and Slimes of Marc Summers (2016), a stage adaptation of Marc Summers' 1999 memoir which recounts how OCD affected his entertainment career.[252] In the novel Turtles All the Way Down (2017) by John Green, teenage main character Aza Holmes struggles with OCD that manifests as a fear of the human microbiome. Throughout the story, Aza repeatedly opens an unhealed callus on her finger to drain out what she believes are pathogens. The novel is based on Green's own experiences with OCD. He explained that Turtles All the Way Down is intended to show how "most people with chronic mental illnesses also live long, fulfilling lives".[253] The British TV series Pure (2019) stars Charly Clive as a 24-year-old Marnie who is plagued by disturbing sexual thoughts, as a kind of primarily obsessional obsessive compulsive disorder.[254] |
社会と文化 このリボンは、トリコチロマニアやその他の身体に焦点を当てた反復行動を表しています。 芸術、娯楽、メディア 映画やテレビ番組は、OCDのような障害を理想化したり、不完全に表現したりすることがある[244]。 演劇や映画化された『オッド・カップル』では、OCDの一般的な症状のいくつかを示すフェ リックスのキャラクターを中心に描かれている[247]。 映画『アズ・グッド・アズ・イット・ゲッツ』(1997年)では、俳優ジャック・ニコルソンが、生活を混乱させる儀式的な行動を行う強迫性障害の男性を演じている[248]。 映画『マッチスティック・メン』(2003年)では、強迫性障害の詐欺師ロイ(ニコラス・ケイジ)が、ドアを3回開け閉めしながら、そのドアを通り抜ける前に声に出して数を数える様子を描いている[249]。 テレビシリーズ『モンク』(2002-2009年)では、主人公のエイドリアン・モンクが人との接触と汚れの両方を恐れている[250][251]。 一人芝居『The Life and Slimes of Marc Summers』(2016年)は、強迫性障害が彼の芸能活動にどのような影響を与えたかを語ったマーク・サマーズの1999年の回顧録を舞台化したものである[252]。 ジョン・グリーンによる小説『タートルズ・オール・ザ・ウェイ・ダウン』(2017年)では、10代の主人公アザ・ホームズが、人間のマイクロバイオーム に対する恐怖として現れる強迫性障害と闘っている。物語中、アザは指の治っていない角質を繰り返し開き、病原体と思われるものを排出する。この小説は、グ リーン自身の強迫性障害の体験に基づいている。彼は、『タートルズ・オール・ザ・ウェイ・ダウン』は、「慢性的な精神疾患を抱える人の多くが、充実した長 い人生を送る」ことを示すためのものだと説明している[253]。 イギリスのテレビシリーズ『Pure』(2019年)では、主に強迫性障害の一種として、不穏な性的思考に悩まされる24歳のマーニーをチャーリー・クライヴが演じている[254]。 |
| Research The naturally occurring sugar inositol has been suggested as a treatment for OCD.[255] μ-Opioids agonists, such as hydrocodone and tramadol, may improve OCD symptoms.[256] Administration of opiate treatment may be contraindicated in individuals concurrently taking CYP2D6 inhibitors such as fluoxetine and paroxetine.[257] Much current research is devoted to the therapeutic potential of the agents that affect the release of the neurotransmitter glutamate or the binding to its receptors. These include riluzole, memantine, gabapentin, N-acetylcysteine, topiramate and lamotrigine.[258] Research on the potential for other supplements, such as milk thistle, to help with OCD and various neurological disorders, is ongoing.[259] |
研究 天然に存在する糖であるイノシトールはOCDの治療薬として示唆されている[255]。 ヒドロコドンやトラマドールなどのμ-オピオイド作動薬は、OCD症状を改善する可能性がある[256]。 現在、神経伝達物質であるグルタミン酸の放出またはその受容体への結合に影響を及ぼす薬剤の治療可能性について、多くの研究が行われている。これには、リ ルゾール、メマンチン、ガバペンチン、N-アセチルシステイン、トピラマート、ラモトリギンなどが含まれる[258]。ミルクシスルなどの他のサプリメン トがOCDや様々な神経疾患に役立つ可能性についての研究が進行中である[259]。 |
| Anxiety Disorder Bipolar disorder Body dysmorphic disorder Compulsive hoarder Cyclothymia Delusional disorder Hypochondriasis Major depressive disorder Obsessive–compulsive spectrum Tic disorder Trichotillomania |
不安障害 双極性障害 身体醜形障害 強迫性溜め込み症 サイクロサイミア 妄想性障害 心気症 大うつ病性障害 強迫スペクトラム チック障害 トリコチロマニア |
| https://en.wikipedia.org/wiki/Obsessive%E2%80%93compulsive_disorder |
リ ンク
文 献
そ の他の情報
Copyleft, CC, Mitzub'ixi Quq Chi'j, 1996-2099
![]()
☆
 ☆
☆