依存症の予防とその歴史
Prevention and history of addiction
☆ 依存症の予防とその歴史:乱用または依存の可能性とは、医療目的以外で薬物を使用する傾向のことです。これは通常、陶酔感、気分変化、または鎮静を目的としています[131]。乱 用可能性は、薬物を使用する人が、それ以外では得られないものを望んでいる場合に使用されます。これを手に入れる唯一の方法は、薬物を使用することだ。乱 用可能性を検討する場合、その薬物が乱用されるかどうかを判断するための決定要因がいくつかある。これらの要因は、薬物の化学組成、脳への影響、および研 究対象集団の年齢、脆弱性、および(精神的および身体的)健康状態だ。[131] 乱用可能性の高い特定の化学組成を持つ薬物はいくつかある。これらは、コカイン、ヘロイン、吸入薬、マリファナ、MDMA(エクスタシー)、メタンフェタ ミン、PCP、合成カンナビノイド、合成カチノン(バスソルト)、ニコチン(例:タバコ)、アルコールなどだ。[132]
★依存症については「依存症」(Addiction)を参照してください
| Prevention Main articles: Harm reduction and Preventive healthcare Abuse liability Abuse or addiction liability is the tendency to use drugs in a non-medical situation. This is typically for euphoria, mood changing, or sedation.[131] Abuse liability is used when the person using the drugs wants something that they otherwise can not obtain. The only way to obtain this is through the use of drugs. When looking at abuse liability there are a number of determining factors in whether the drug is abused. These factors are: the chemical makeup of the drug, the effects on the brain, and the age, vulnerability, and the health (mental and physical) of the population being studied.[131] There are a few drugs with a specific chemical makeup that leads to a high abuse liability. These are: cocaine, heroin, inhalants, marijuana, MDMA (ecstasy), methamphetamine, PCP, synthetic cannabinoids, synthetic cathinones (bath salts), nicotine (e.g. tobacco), and alcohol.[132] |
予防 主な記事:ハームリダクションおよび予防医療 乱用可能性 乱用または依存の可能性とは、医療目的以外で薬物を使用する傾向のことです。これは通常、陶酔感、気分変化、または鎮静を目的としています[131]。乱 用可能性は、薬物を使用する人が、それ以外では得られないものを望んでいる場合に使用されます。これを手に入れる唯一の方法は、薬物を使用することだ。乱 用可能性を検討する場合、その薬物が乱用されるかどうかを判断するための決定要因がいくつかある。これらの要因は、薬物の化学組成、脳への影響、および研 究対象集団の年齢、脆弱性、および(精神的および身体的)健康状態だ。[131] 乱用可能性の高い特定の化学組成を持つ薬物はいくつかある。これらは、コカイン、ヘロイン、吸入薬、マリファナ、MDMA(エクスタシー)、メタンフェタ ミン、PCP、合成カンナビノイド、合成カチノン(バスソルト)、ニコチン(例:タバコ)、アルコールなどだ。[132] |
| Potential vaccines for addiction to substances Vaccines for addiction have been investigated as a possibility since the early 2000s.[133] The general theory of a vaccine intended to "immunize" against drug addiction or other substance abuse is that it would condition the immune system to attack and consume or otherwise disable the molecules of such substances that cause a reaction in the brain, thus preventing the addict from being able to realize the effect of the drug. Addictions that have been floated as targets for such treatment include nicotine, opioids, and fentanyl.[134][135][136][137] Vaccines have been identified as potentially being more effective than other anti-addiction treatments, due to "the long duration of action, the certainty of administration and a potential reduction of toxicity to important organs".[138] Specific addiction vaccines in development include: NicVAX, a conjugate vaccine intended to reduce or eliminate physical dependence on nicotine.[139] This proprietary vaccine is being developed by Nabi Biopharmaceuticals[140] of Rockville, MD. with the support from the U.S. National Institute on Drug Abuse. NicVAX consists of the hapten 3'-aminomethylnicotine which has been conjugated (attached) to Pseudomonas aeruginosa exotoxin A.[141] TA-CD, an active vaccine[142] developed by the Xenova Group which is used to negate the effects of cocaine. It is created by combining norcocaine with inactivated cholera toxin. It works in much the same way as a regular vaccine. A large protein molecule attaches to cocaine, which stimulates response from antibodies, which destroy the molecule. This also prevents the cocaine from crossing the blood–brain barrier, negating the euphoric high and rewarding effect of cocaine caused from stimulation of dopamine release in the mesolimbic reward pathway. The vaccine does not affect the user's "desire" for cocaine—only the physical effects of the drug.[143] TA-NIC, used to create human antibodies to destroy nicotine in the human body so that it is no longer effective.[144] As of September 2023, it was further reported that a vaccine "has been tested against heroin and fentanyl and is on its way to being tested against OxyContin".[145] |
物質依存症に対する潜在的なワクチン 依存症に対するワクチンは、2000年代初頭から可能性として研究されている。[133] 薬物依存症やその他の物質乱用に対して「免疫」を与えることを目的としたワクチンの一般的な理論は、脳に反応を引き起こす物質の分子を攻撃して消費した り、その他の方法で無効化したりするように免疫系を条件付け、依存者が薬物の効果を実現できないようにするというものだ。このような治療の対象として提案 されている依存症には、ニコチン、オピオイド、フェンタニルなどが挙げられています。[134][135][136][137] ワクチンは、「作用の持続期間が長く、投与の確実性があり、重要な臓器への毒性を軽減する可能性」から、他の依存症治療法よりも効果的である可能性が指摘 されています。[138] 開発中の特定の依存症ワクチンには、次のようなものがある。 NicVAX は、ニコチンに対する身体的依存を軽減または排除することを目的とした複合ワクチンである。[139] この独自開発のワクチンは、メリーランド州ロックビルにある Nabi Biopharmaceuticals[140] が、米国国立薬物乱用研究所の支援を受けて開発している。NicVAXは、3'-アミノメチルニコチンというハプテンを、Pseudomonas aeruginosaのエクソトキシンAに結合(付着)させたものである。[141] TA-CDは、コカインの効果を無効化するためにXenova Groupが開発した活性ワクチン[142]です。これは、ノルコカインと不活化コレラ毒素を組み合わせることで作成されます。その作用機序は通常のワク チンとほぼ同じです。大きなタンパク質分子がコカインに結合し、抗体の反応を刺激して分子を破壊する。これにより、コカインが血液脳関門を通過するのを防 ぎ、ドーパミンの放出による中脳辺縁系報酬回路での多幸感や報酬効果を無効化する。このワクチンは、ユーザーのコカインに対する「欲求」には影響せず、薬 物の物理的効果のみを阻害する。[143] TA-NICは、人体内のニコチンを破壊し無効化するヒト抗体を生成するために使用される。[144] 2023年9月現在、ヘロインとフェンタニルに対するワクチンが試験され、オキシコドンに対する試験が進行中であることがさらに報告されている。[145] |
| Treatment Main article: Treatment and management of addiction To be effective, treatment for addiction that is pharmacological or biologically based need to be accompanied by other interventions such as cognitive behavioral therapy (CBT) and dialectical behavioral therapy (DBT); individual and group psychotherapy, behavior modification strategies, twelve-step programs, and residential treatment facilities.[146][19] The transtheoretical model (TTM) can be used to determine when treatment can begin and which method will be most effective. If treatment begins too early, it can cause a person to become defensive and resistant to change.[41][147] |
治療 主な記事:依存症の治療と管理 薬物療法や生物学的療法に基づく依存症の治療が効果を発揮するためには、認知行動療法(CBT)や弁証法的行動療法(DBT)、個人療法やグループ療法、 行動修正戦略、12ステッププログラム、入院治療施設などの他の介入を併用する必要がある。[146][19] 治療開始のタイミングや最も効果的な方法を決定するために、トランセオретиカルモデル(TTM)が活用できる。治療が早すぎると、人格が防御的にな り、変化に抵抗を示すようになる。[41][147] |
| Epidemiology Further information: Countries by alcohol consumption, Opioid epidemic, and Prevalence of tobacco use Due to cultural variations, the proportion of individuals who develop a drug or behavioral addiction within a specified time period (i.e., the prevalence) varies over time, by country, and across national population demographics (e.g., by age group, socioeconomic status, etc.).[47] Where addiction is viewed as unacceptable, there will be fewer people addicted. Asia The prevalence of alcohol dependence is not as high as is seen in other regions. In Asia, not only socioeconomic factors but biological factors influence drinking behavior.[148] Internet addiction disorder is highest in the Philippines, according to both the IAT (Internet Addiction Test) – 5% and the CIAS-R (Revised Chen Internet Addiction Scale) – 21%.[149] |
疫学 詳細情報:アルコール消費量、オピオイドの流行、およびタバコの使用率 文化の違いにより、特定の期間内に薬物または行動依存症を発症する個人の割合(すなわち、有病率)は、時間、国、および国民の人口統計(年齢層、社会経済的地位など)によって異なる[47]。依存症が容認されない社会では、依存症になる人は少なくなる。 アジア アルコール依存症の有病率は、他の地域ほど高くない。アジアでは、社会経済的要因だけでなく、生物学的要因も飲酒行動に影響を与える。[148] インターネット依存症の有病率は、IAT(インターネット依存症検査)で5%、CIAS-R(改訂版チェン・インターネット依存症尺度)で21%と、フィリピンが最も高い。[149] |
| Australia Further information: Alcoholism in rural Australia The prevalence of substance use disorder among Australians was reported at 5.1% in 2009.[150] In 2019 the Australian Institute of Health and Welfare conducted a national drug survey that quantified drug use for various types of drugs and demographics.[151] The survey found that in 2019, 11% of people over 14 years old smoke daily; that 9.9% of those who drink alcohol, which equates to 7.5% of the total population age 14 or older, may qualify as alcohol dependent; that 17.5% of the 2.4 million people who used cannabis in the last year may have hazardous use or a dependence problem; and that 63.5% of about 300000 recent users of meth and amphetamines were at risk for developing problem use.[151] |
オーストラリア 詳細情報:オーストラリアの農村部のアルコール依存症 2009年のオーストラリア人の物質使用障害の有病率は5.1%と報告されている[150]。2019年、オーストラリア保健福祉研究所は、さまざまな種 類の薬物使用と人口統計を定量化した全国薬物調査を実施した。[151] この調査では、2019 年には 14 歳以上の人々の 11% が毎日喫煙しており、アルコールを飲む人の 9.9% (14 歳以上の人口の 7.5% に相当) がアルコール依存症と認定される可能性があり、大麻を使用した 240 万人中 5% が危険な使用または依存の問題を抱えている可能性があり、最近メタンフェタミンを使用した約 30 万人中 63.5% が危険な使用または依存の問題を抱えている可能性があることが明らかになった。5% が危険な使用または依存の問題を抱えている可能性があり、最近メタンフェタミンおよびアンフェタミンを使用した約 30 万人中 63.5% が問題使用を発症するリスクがあることが明らかになった。[151] |
| Europe Further information: Alcoholism in Ireland and Alcoholism in Russia In 2015, the estimated prevalence among the adult population was 18.4% for heavy episodic alcohol use (in the past 30 days); 15.2% for daily tobacco smoking; and 3.8% for cannabis use, 0.77% for amphetamine use, 0.37% for opioid use, and 0.35% for cocaine use in 2017. The mortality rates for alcohol and illicit drugs were highest in Eastern Europe.[152] Data shows a downward trend of alcohol use among children 15 years old in most European countries between 2002 and 2014. First-time alcohol use before the age of 13 was recorded for 28% of European children in 2014.[19] |
ヨーロッパ 詳細情報:アイルランドのアルコール依存症とロシアのアルコール依存症 2015年の成人人口における推定有病率は、過去30日間の過量飲酒が18.4%、毎日のタバコ喫煙が15.2%、大麻使用が3.8%、アンフェタミン使 用が0.77%、オピオイド使用が0.37%、コカイン使用が0.35%だった。アルコールと違法薬物の死亡率は東欧で最も高かった。[152] 2002年から2014年にかけて、ほとんどのヨーロッパ諸国で15歳の子どものアルコール使用率が減少傾向を示している。2014年には、ヨーロッパの 子どもの28%が13歳未満で初めてアルコールを摂取したことが記録されている。[19] |
| United States Further information: Cocaine in the United States, Crack epidemic in the United States, and Opioid epidemic in the United States Based on representative samples of the US youth population in 2011, the lifetime prevalence[note 7] of addictions to alcohol and illicit drugs has been estimated to be approximately 8% and 2–3% respectively.[153] Based on representative samples of the US adult population in 2011, the 12-month prevalence of alcohol and illicit drug addictions were estimated at 12% and 2–3% respectively.[153] The lifetime prevalence of prescription drug addictions is around 4.7%.[154] As of 2021, 43.7 million people aged 12 or older surveyed by the National Survey on Drug Use and Health in the United States needed treatment for an addiction to alcohol, nicotine, or other drugs. The groups with the highest number of people were 18–25 years (25.1%) and "American Indian or Alaska Native" (28.7%).[155] Only about 10%, or a little over 2 million, receive any form of treatments, and those that do generally do not receive evidence-based care.[156][157] One-third of inpatient hospital costs and 20% of all deaths in the US every year are the result of untreated addictions and risky substance use.[156][157] In spite of the massive overall economic cost to society, which is greater than the cost of diabetes and all forms of cancer combined, most doctors in the US lack the training to effectively address a drug addiction.[156][157] Estimates of lifetime prevalence rates in the US are 1–2% for compulsive gambling, 5% for sexual addiction, 2.8% for food addiction, and 5–6% for compulsive shopping.[23] The time-invariant prevalence rate for sexual addiction and related compulsive sexual behavior (e.g., compulsive masturbation with or without pornography, compulsive cybersex, etc.) within the US ranges from 3–6% of the population.[31] According to a 2017 poll conducted by the Pew Research Center, almost half of US adults know a family member or close friend who has struggled with a drug addiction at some point in their life.[158] In 2019, opioid addiction was acknowledged as a national crisis in the United States.[159] An article in The Washington Post stated that "America's largest drug companies flooded the country with pain pills from 2006 through 2012, even when it became apparent that they were fueling addiction and overdoses." The National Epidemiologic Survey on Alcohol and Related Conditions found that from 2012 to 2013 the prevalence of Cannabis use disorder in U.S. adults was 2.9%.[160] |
アメリカ合衆国 詳細情報:アメリカ合衆国におけるコカイン、アメリカ合衆国におけるクラック流行、アメリカ合衆国におけるオピオイド流行 2011年の米国の若年層人口の代表的なサンプルに基づいて、アルコールおよび違法薬物への依存症の生涯有病率[注7]は、それぞれ約8%および2~3% と推定されている。[153] 2011年の米国成人人口の代表的なサンプルに基づき、アルコールと違法薬物依存症の12ヶ月有病率はそれぞれ12%と2~3%と推計されている。 [153] 処方薬依存症の生涯有病率は約4.7%である。[154] 2021年現在、米国の薬物使用と保健に関する全国調査で調査された12歳以上の4,370万人が、アルコール、ニコチン、その他の薬物依存の治療を必要 としている。その人数が最も多いグループは、18~25歳(25.1%)と「アメリカインディアンまたはアラスカ先住民」 (28.7%)でした。[155] 治療を受けるのは約10%(200万人強)に過ぎず、その多くはエビデンスに基づくケアを受けていません。[156][157] アメリカでは、入院医療費の3分の1と全死亡の20%が、未治療の依存症と危険な薬物使用が原因となっています。[156][157] 糖尿病とすべての癌のコストを合わせたよりも大きい、社会全体への莫大な経済的コストにもかかわらず、米国の医師の大多数は薬物依存症を効果的に対処する ための訓練を受けていない。[156][157] 米国における生涯有病率の推計値は、強迫性ギャンブルが1~2%、性依存症が5%、食依存症が2.8%、強迫性買い物が5~6%となっている。[23] 米国における性依存症および関連する強迫性性行動(例:ポルノの有無を問わず強迫的な自慰行為、強迫的なサイバーセックスなど)の恒常的な有病率は、人口 の3~6%と推定されている。[31] ピュー・リサーチ・センターが2017年に実施した世論調査によると、米国成人のほぼ半数が、人生のある時点で薬物依存症に苦しんだ家族や親しい友人を知っている。[158] 2019 年、オピオイド依存症は米国における国家的な危機として認識されました[159]。ワシントン・ポスト紙の記事では、「米国の大手製薬会社は、依存症や過 剰摂取を助長していることが明らかになったにもかかわらず、2006 年から 2012 年にかけて、鎮痛剤を国内に大量に出回らせた」と報じられています。 アルコールおよび関連状態に関する全国疫学調査によると、2012 年から 2013 年にかけて、米国の成人の大麻使用障害の有病率は 2.9% だった。[160] |
| Canada A Statistics Canada Survey in 2012 found the lifetime prevalence and 12-month prevalence of substance use disorders were 21.6%, and 4.4% in those 15 and older.[161] Alcohol abuse or dependence reported a lifetime prevalence of 18.1% and a 12-month prevalence of 3.2%.[161] Cannabis abuse or dependence reported a lifetime prevalence of 6.8% and a 12-month prevalence of 3.2%.[161] Other drug abuse or dependence has a lifetime prevalence of 4.0% and a 12-month prevalence of 0.7%.[161] Substance use disorder is a term used interchangeably with a drug addiction.[162] In Ontario, Canada between 2009 and 2017, outpatient visits for mental health and addiction increased from 52.6 to 57.2 per 100 people, emergency department visits increased from 13.5 to 19.7 per 1000 people and the number of hospitalizations increased from 4.5 to 5.5 per 1000 people.[163] Prevalence of care needed increased the most among the 14–17 age group overall.[163] |
カナダ 2012年のカナダ統計局の調査によると、15歳以上の人々の物質使用障害の生涯有病率は21.6%、12ヶ月有病率は4.4%だった。[161] アルコール乱用または依存の生涯有病率は18.1%、12ヶ月有病率は3.2%だった。[161] 大麻の乱用または依存の生涯有病率は6.8%、12ヶ月有病率は3.2%でした。[161] その他の薬物乱用または依存の生涯有病率は4.0%、12ヶ月有病率は0.7%でした。[161] 物質使用障害は、薬物依存症と置き換えられる用語です。[162] 2009 年から 2017 年にかけて、カナダのオンタリオ州では、精神保健および依存症に関する外来受診が 52.6 人から 57.2 人に、救急外来の受診は 1000 人あたり 13.5 人から 19.7 人に、入院者数は 1000 人あたり 4.5 人から 5.5 人に増加した[163]。ケアの必要性の有病率は、14~17 歳の年齢層で全体として最も増加した[163]。 |
| South America The realities of opioid use and opioid use disorder in Latin America may be deceptive if observations are limited to epidemiological findings. In the United Nations Office on Drugs and Crime report,[164] although South America produced 3% of the world's morphine and heroin and 0.01% of its opium, prevalence of use is uneven. According to the Inter-American Commission on Drug Abuse Control, consumption of heroin is low in most Latin American countries, although Colombia is the area's largest opium producer. Mexico, because of its border with the United States, has the highest incidence of use.[165] |
南アメリカ ラテンアメリカにおけるオピオイドの使用およびオピオイド使用障害の現実は、疫学的知見のみに観察を限定すると、誤解を招くおそれがある。国連薬物犯罪事 務所(UNODC)の報告書[164]によると、南アメリカは世界全体のモルヒネおよびヘロインの 3%、アヘン生産量の 0.01% を生産しているが、使用の有病率は不均一である。米州薬物乱用対策委員会によると、コロンビアが地域最大のオピウム生産国であるにもかかわらず、ラテンア メリカの大多数の国ではヘロインの消費量は低い。メキシコはアメリカ合衆国との国境を接しているため、使用率が最も高い。[165] |
| Etymology The word addiction derives from the Latin "addico", meaning "giving over" with both positive connotations (devotion, dedication) and negative ones (being enslaved to a creditor in Roman law). This dual meaning persisted in traditional English dictionaries, encompassing both legal surrender and personal devotion to habits. Later, 19th century temperance movements narrowed the definition of addiction to just drug-related disease, ignoring behavioral addictions and the possibility of positive or neutral addictions. This restrictive view opposes the current understanding of addiction.[166] Addiction and addictive behavior are polysemes denoting a category of mental disorders, of neuropsychological symptoms, or of merely maladaptive/harmful habits and lifestyles.[167] A common use of the term addiction in medicine is for neuropsychological symptoms denoting pervasive/excessive and intense urges to engage in a category of behavioral compulsions or impulses towards sensory rewards (e.g., alcohol, betel quid, drugs, sex, gambling, video gaming).[168][169][170][171][121] Addictive disorders or addiction disorders are mental disorders involving high intensities of addictions (as neuropsychological symptoms) that induce functional disabilities (i.e., limit subjects' social/family and occupational activities); the two categories of such disorders are substance-use addictions and behavioral addictions.[172][167][171][121] The etymology of the term addiction throughout history has been misunderstood and has taken on various meanings associated with the word.[173] An example is the usage of the word in the religious landscape of early modern Europe.[174] "Addiction" at the time meant "to attach" to something, giving it both positive and negative connotations. The object of this attachment could be characterized as "good or bad".[175] The meaning of addiction during the early modern period was mostly associated with positivity and goodness;[174] during this early modern and highly religious era of Christian revivalism and Pietistic tendencies,[174] it was seen as a way of "devoting oneself to another".[175] |
語源 「依存症」という言葉は、ラテン語の「addico」に由来し、「委ねる」という意味で、肯定的な意味(献身、献身)と否定的な意味(ローマ法における債 権者に奴隷にされる)の両方があります。この二重の意味は、伝統的な英語辞書にも残っており、法的降伏と習慣に対する個人的な献身の両方を包含していま す。その後、19 世紀の禁酒運動により、依存症の定義は薬物関連疾患のみに狭められ、行動依存症や肯定的または中立的な依存症の可能性は無視された。この限定的な見解は、 現在の依存症の理解とは対立している。[166] 依存症および依存行動は、精神障害、神経心理学的症状、あるいは単に不適応/有害な習慣やライフスタイルのカテゴリーを示す多義語だ。[167] 医学における「依存症」という用語の一般的な使用法は、感覚的報酬(例:アルコール、ベテルナッツ、薬物、性行為、ギャンブル、ビデオゲーム)への行動的 強迫や衝動への広範で過剰かつ激しい欲求を示す神経心理学的症状を指す。[168][169][170][171][121] 依存症または依存障害は、機能障害(すなわち、対象者の社会的/家族的および職業的活動を制限する)を引き起こす高い強度の依存(神経心理学的症状とし て)を特徴とする精神障害で、この障害の2つのカテゴリーは、物質使用依存症と行動依存症です。[172][167][171][121] 「依存症」という用語の語源は歴史的に誤解され、言葉に関連する多様な意味を帯びてきた。[173] 例えば、近世ヨーロッパの宗教的文脈における用語の用法が挙げられる。[174] 当時の「依存症」は「何かにくっつく」という意味を持ち、ポジティブとネガティブな両方のニュアンスを含んでいた。この「結びつく」対象は「良いもの」ま たは「悪いもの」と特徴付けられた。[175] 近代初期の依存症の意味は主にポジティブで良いものと関連付けられていた。[174] このキリスト教の復興とピエティズムの傾向が強く、宗教的な時代において、依存症は「他者に自分を捧げる方法」と見なされていた。[175] |
| The suffixes "-holic" and "-holism" In contemporary modern English "-holic" is a suffix that can be added to a subject to denote an addiction to it. It was extracted from the word alcoholism (one of the first addictions to be widely identified both medically and socially) (correctly the root "alcohol" plus the suffix "-ism") by misdividing or rebracketing it into "alco" and "-holism". There are correct medico-legal terms for such addictions: dipsomania is the medico-legal term for alcoholism;[176] other examples are in this table:[citation needed] 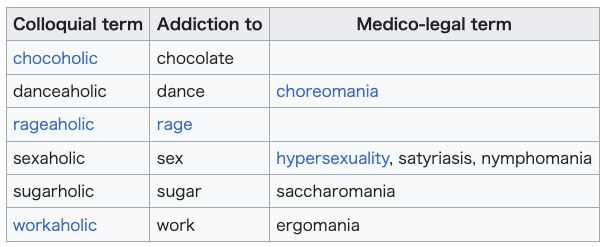 History Modern research on addiction has led to a better understanding of the disease with research on the topic dating back to 1875, specifically on morphine addiction.[177] This furthered the understanding of addiction being a medical condition. It was not until the 19th century that addiction was seen and acknowledged in the Western world as a disease, being both a physical condition and mental illness.[178] Today, addiction is understood both as a biopsychosocial and neurological disorder that negatively impacts those who are affected by it, most commonly associated with the use of drugs and excessive use of alcohol.[4] The understanding of addiction has changed throughout history, which has impacted and continues to impact the ways it is medically treated and diagnosed.[citation needed] |
接尾辞「-holic」と「-holism」 現代英語において「-holic」は、対象物への依存や中毒を表すために名詞に付加される接尾辞だ。これは、医学的・社会的に初めて広く認識された依存症 の一つである「アルコール依存症」(正確には「アルコール」という語根に「-ism」という接尾辞が付いたもの)から、誤って「alco」と「- holism」に分割または再括弧付けされることで抽出された。このような依存症には正しい医学的・法的用語がある。アルコール依存症の医学的・法的用語 は「ディプソマニア」[176] であり、他の例はこの表に示されている[出典必要]。 歴史 依存症に関する現代の研究は、1875年にモルヒネ依存症に関する研究が開始されて以来、この疾患の理解を深めてきた。[177] これにより、依存症が医学的疾患であるとの理解がさらに進んだ。依存症が、身体的状態および精神疾患の両方である疾患として西洋世界で認識され、認められ たのは19世紀に入ってからのことだった。[178] 現在、依存症は、生物心理社会的および神経学的障害として理解されており、影響を受ける人々に負の影響を及ぼす。最も一般的に、薬物の使用やアルコールの 過剰摂取と関連付けられている。[4] 依存症の理解は歴史を通じて変化し、その医療的治療法や診断方法に影響を与え続けています。[出典が必要] |
| Addiction and art The arts can be used in a variety of ways to address issues related to addiction. Art can be used as a form of therapy in the treatment of substance use disorders. Creative activities like painting, sculpting, music, and writing can help people express their feelings and experiences in safe and healthy ways. The arts can be used as an assessment tool to identify underlying issues that may be contributing to a person's substance use disorder. Through art, individuals can gain insights into their own motivations and behaviors that can be helpful in determining a course of treatment. Finally, the arts can be used to advocate for those suffering from a substance use disorder by raising awareness of the issue and promoting understanding and compassion. Through art, individuals can share their stories, increase awareness, and offer support and hope to those struggling with substance use disorders. |
依存症と芸術 芸術は、依存症に関連する問題に対処するためにさまざまな方法で活用することができます。芸術は、物質使用障害の治療における療法の一形態として活用する ことができます。絵画、彫刻、音楽、執筆などの創造的な活動は、人々が自分の感情や経験を安全かつ健全な方法で表現するのに役立ちます。芸術は、人の物質 使用障害の原因となっている根本的な問題を見極めるための評価ツールとしても活用することができます。芸術を通じて、個人は自分の動機や行動について洞察 を得ることができ、治療方針を決定するのに役立つ。最後に、芸術は、問題に対する認識を高め、理解と共感を促進することで、物質使用障害に苦しむ人々を支 援するために活用することができます。芸術を通じて、個人は自分の物語を共有し、認識を高め、物質使用障害に苦しむ人々に支援と希望を与えることができま す。 |
| As therapy Addiction treatment is complex and not always effective due to engagement and service availability concerns, so researchers prioritize efforts to improve treatment retention and decrease relapse rates.[179][180] Characteristics of substance abuse may include feelings of isolation, a lack of confidence, communication difficulties, and a perceived lack of control.[181] In a similar vein, people suffering from substance use disorders tend to be highly sensitive, creative, and as such, are likely able to express themselves meaningfully in creative arts such as dancing, painting, writing, music, and acting.[182] Further evidenced by Waller and Mahony (2002)[183] and Kaufman (1981),[184] the creative arts therapies can be a suitable treatment option for this population especially when verbal communication is ineffective. Primary advantages of art therapy in the treatment of addiction have been identified as:[185][186] Assess and characterize a client's substance use issues Bypassing a client's resistances, defenses, and denial Containing shame or anger Facilitating the expression of suppressed and/or complicated emotions Highlighting a client's strengths Providing an alternative to verbal communication (via use of symbols) and conventional forms of therapy Providing clients with a sense of control Tackling feelings of isolation Art therapy is an effective method of dealing with substance abuse in comprehensive treatment models. When included in psychoeducational programs, art therapy in a group setting can help clients internalize taught concepts in a more personalized manner.[187] During the course of treatment, by examining and comparing artwork created at different times, art therapists can be helpful in identifying and diagnosing issues, as well as charting the extent or direction of improvement as a person detoxifies.[187] Where increasing adherence to treatment regimes and maintaining abstinence is the target; art therapists can aid by customizing treatment directives (encourage the client to create collages that compare pros and cons, pictures that compare past and present and future, and drawings that depict what happened when a client went off medication).[187] Art therapy can function as a complementary therapy used in conjunction with more conventional therapies and can integrate with harm reduction protocols to minimize the negative effects of drug use.[188][186] An evaluation of art therapy incorporation within a pre-existing Addiction Treatment Programme based on the 12 step Minnesota Model endorsed by the Alcoholics Anonymous found that 66% of participants expressed the usefulness of art therapy as a part of treatment.[189][186] Within the weekly art therapy session, clients were able to reflect and process the intense emotions and cognitions evoked by the programme. In turn, the art therapy component of the programme fostered stronger self-awareness, exploration, and externalization of repressed and unconscious emotions of clients, promoting the development of a more integrated 'authentic self'.[190][186] Despite the large number of randomized control trials, clinical control trials, and anecdotal evidence supporting the effectiveness of art therapies for use in addiction treatment, a systematic review conducted in 2018 could not find enough evidence on visual art, drama, dance and movement therapy, or 'arts in health' methodologies to confirm their effectiveness as interventions for reducing substance misuse.[191] Music therapy was identified to have potentially strong beneficial effects in aiding contemplation and preparing those diagnosed with substance use for treatment.[191] |
治療として 依存症の治療は複雑であり、治療への参加やサービスの利用可能性に関する問題から、必ずしも効果的とは限らないため、研究者は治療の継続率の向上と再発率 の低下に重点を置いた取り組みを進めている。[179][180] 薬物乱用の特徴としては、孤立感、自信の欠如、コミュニケーションの困難、コントロールの欠如の認識などが挙げられる。[181] 同様に、物質使用障害に苦しむ人々は、非常に敏感で創造性が高く、そのため、ダンス、絵画、執筆、音楽、演技などの創造的な芸術で、自分自身を意味のある 形で表現できる傾向がある。[182] Waller と Mahony (2002)[183] および Kaufman (1981)[184] によってさらに証明されているように、創造的な芸術療法は、特に言葉によるコミュニケーションが効果的でない場合、この集団に適した治療選択肢となる可能 性があります。 依存症の治療におけるアートセラピーの主な利点は、次のように特定されています。[185][186] クライアントの物質使用の問題を評価し、特徴づける クライアントの抵抗、防御機制、否認を回避する 恥や怒りを抑える 抑圧された複雑な感情の表現を促進する クライアントの強みを強調する 言語コミュニケーションの代替手段(シンボルの使用)や伝統的な療法形態を提供する クライアントにコントロール感を与える 孤立感に対処する アートセラピーは、包括的な治療モデルにおける薬物乱用の対処に効果的な手法です。心理教育プログラムに組み込むと、グループでのアートセラピーは、クラ イアントが教えられた概念をより個人的な形で内面化するのに役立ちます。[187] 治療期間中、アートセラピストは、異なる時期に制作された作品を検証、比較することで、問題の特定と診断、および人格の解毒に伴う改善の程度や方向性の把 握に役立てることができます。[187] 治療計画への遵守率向上と禁断症状の維持が目標の場合、アートセラピストは治療指針をカスタマイズすることで支援できます(クライアントに、メリットとデ メリットを比較するコラージュを作成させたり、過去と現在と未来を比較する絵を描かせたり、薬物を服用しなかった時の状況を表現する絵を描かせたりす る)。[187] アートセラピーは、より従来の治療法と組み合わせて補完的な治療法として機能し、薬物使用の悪影響を最小限に抑えるためのハームリダクション(ハームリダ クション)プロトコルと統合することができる。[188][186] アルコール依存症者支援団体「アルコホーリクス・アノニマス」が推奨する 12 ステップのミネソタモデルに基づく、既存の依存症治療プログラムにアートセラピーを取り入れた評価では、参加者の 66% が、治療の一部としてアートセラピーの有用性を評価した。[189][186] 週1回のアートセラピーセッションにおいて、クライアントはプログラムによって引き起こされた強い感情や認知を反映し処理することができました。その結 果、プログラムのアートセラピー要素は、クライアントの抑圧された無意識の感情の自己認識、探求、外在化を促進し、より統合された「本物の自己」の発達を 促しました。[190][186] 依存症治療におけるアートセラピーの有効性を支持するランダム化比較試験、臨床対照試験、および事例報告は多数あるが、2018 年に実施された系統的レビューでは、視覚芸術、演劇、ダンス、運動療法、あるいは「保健における芸術」の手法について、薬物乱用を削減するための介入とし ての有効性を確認する十分な証拠は見つからなかった。[191] 音楽療法は、物質使用と診断された人々の治療準備を支援し、内省を促す点で、潜在的に強い有益な効果を有することが示された。[191] |
| As an assessment tool The Formal Elements Art Therapy Scale (FEATS) is an assessment tool used to evaluate drawings created by people suffering from substance use disorders by comparing them to drawings of a control group (consisting of individuals without SUDs).[192][186] FEATS consists of twelve elements, three of which were found to be particularly effective at distinguishing the drawings of those with SUDs from those without: Person, Realism, and Developmental. The Person element assesses the degree to which a human features are depicted realistically, the Realism element assesses the overall complexity of the artwork, and the Developmental element assesses "developmental age" of the artwork in relation to standardized drawings from children and adolescents.[192] By using the FEATS assessment tool, clinicians can gain valuable insight into the drawings of individuals with SUDs, and can compare them to those of the control group. Formal assessments such as FEATS provide healthcare providers with a means to quantify, standardize, and communicate abstract and visceral characteristics of SUDs to provide more accurate diagnoses and informed treatment decisions.[192] Other artistic assessment methods include the Bird's Nest Drawing: a useful tool for visualizing a client's attachment security.[193][186] This assessment method looks at the amount of color used in the drawing, with a lack of color indicating an 'insecure attachment', a factor that the client's therapist or recovery framework must take into account.[194] Art therapists working with children of parents suffering from alcoholism can use the Kinetic Family Drawings assessment tool to shed light on family dynamics and help children express and understand their family experiences.[195][186] The KFD can be used in family sessions to allow children to share their experiences and needs with parents who may be in recovery from alcohol use disorder. Depiction of isolation of self and isolation of other family members may be an indicator of parental alcoholism.[195] |
評価ツールとして 形式要素アートセラピースケール(FEATS)は、物質使用障害に苦しむ人々が描いた絵を、対照群(物質使用障害のない個人で構成される)の絵と比較する ことで評価するための評価ツールだ。[192][186] FEATS は 12 の要素で構成されており、そのうち 3 つは、物質使用障害のある人とない人の絵を区別するのに特に有効であることがわかった。人格要素は、人物の特徴がどれだけ現実的に描かれているかを評価 し、現実性要素は、作品の全体的な複雑さを評価し、発達要素は、子供や青少年の標準的な絵と比較して、作品の「発達年齢」を評価する。[192] FEATS 評価ツールを使用することで、臨床医は SUD 患者の絵について貴重な洞察を得ることができ、対照群の絵と比較することができる。FEATSのような形式的な評価は、医療従事者がSUDの抽象的で直感 的な特性を定量化、標準化、コミュニケーションする手段を提供し、より正確な診断と適切な治療決定を支援する。[192] 他の芸術的評価方法には、クライアントの愛着の安全性を可視化する有用なツールである「バード・ネスト・ドローイング」がある。[193][186] この評価方法は、絵に使用された色の量に注目し、色の不足は「不安定な愛着」を示し、クライアントのセラピストや回復枠組みが考慮すべき要因となる。 [194] アルコール依存症の親を持つ子供たちを支援するアートセラピストは、キネティック・ファミリー・ドローイング(KFD)という評価ツールを使用して、家族 の力学を明らかにし、子供たちが家族の経験を表現し、理解するのを助けることができる。[195][186] KFD は、子供たちがアルコール使用障害から回復中の親と自分の経験やニーズを共有するための家族セッションで使用することができる。自己の孤立や他の家族メン バーの孤立の描写は、親のアルコール依存症の指標となる可能性がある。[195] |
| Advocacy Stigma can lead to feelings of shame that can prevent people with substance use disorders from seeking help and interfere with provision of harm reduction services.[196][197][198] It can influence healthcare policy, making it difficult for these individuals to access treatment.[199] Artists attempt to change the societal perception of addiction from a punishable moral offense to instead a chronic illness necessitating treatment. This form of advocacy can help to relocate the fight of addiction from a judicial perspective to the public health system.[200] Artists who have personally lived with addiction or undergone recovery may use art to depict their experiences in a manner that uncovers the "human face of addiction". By bringing experiences of addiction and recovery to a personal level and breaking down the "us and them", the viewer may be more inclined to show compassion, forego stereotypes and stigma of addiction, and label addiction as a social rather than individual problem.[200] According to Santora[200] the main purposes in using art as a form of advocacy in the education and prevention of substance use disorders include: Addiction art exhibitions can come from a variety of sources, but the underlying message of these works is the same: to communicate through emotions without relying on intellectually demanding/gatekept facts and figures. These exhibitions can either stand alone, reinforce, or challenge facts. A powerful educational tool for increasing awareness and understanding of addiction as a medical illness. Exhibitions featuring personal stories and images can help to create lasting impressions on diverse audiences (including addiction scientists/researchers, family/friends of those affected by addiction etc.), highlighting the humanity of the problem and in turn encouraging compassion and understanding. A way to destigmatize substance use disorders and shift public perception from viewing them as a moral failing to understanding them as a chronic medical condition which requires treatment. Provide those who are struggling with addiction assurance and encouragement of healing, and let them know that they are not alone in their struggle. The use of visual arts can help bring attention to the lack of adequate substance use treatment, prevention, and education programs and services in a healthcare system. Messages can encourage policymakers to allocate more resources to addiction treatment and prevention from federal, state, and local levels. The Temple University College of Public Health department conducted a project to promote awareness around opioid use and reduce associated stigma by asking students to create art pieces that were displayed on a website they created and promoted via social media.[201] Quantitative and qualitative data was recorded to measure engagement, and the student artists were interviewed, which revealed a change in perspective and understanding, as well as greater appreciation of diverse experiences. Ultimately, the project found that art was an effective medium for empowering both the artist creating the work and the person interacting with it.[201] Another author critically examined works by contemporary Canadian artists that deal with addiction via the metaphor of a cultural landscape to "unmap" and "remap" ideologies related to Indigenous communities and addiction to demonstrate how colonial violence in Canada has drastically impacted the relationship between Indigenous peoples, their land, and substance abuse.[202] A project known as "Voice" was a collection of art, poetry and narratives created by women living with a history of addiction to explore women's understanding of harm reduction, challenge the effects of stigma and give voice to those who have historically been silenced or devalued.[203] In the project, nurses with knowledge of mainstream systems, aesthetic knowing, feminism and substance use organized weekly gatherings, wherein women with histories of substance use and addiction worked alongside a nurse to create artistic expressions. Creations were presented at several venues, including an International Conference on Drug Related Harm, a Nursing Conference and a local gallery to positive community response.[203] |
アドボカシー スティグマは、物質使用障害のある人々に恥の感情を抱かせ、助けを求めることを妨げ、ハームリダクションサービスの提供を妨げる要因となる。[196][197][198] また、医療政策にも影響を及ぼし、こうした人々が治療を受けることを困難にする。[199] アーティストたちは、依存症を罰すべき道徳的犯罪という社会の認識を変え、治療が必要な慢性疾患という認識に変えようとしています。この形のアドボカシーは、依存症との闘いを司法の観点から公衆衛生システムへと移すのに役立つ可能性があります。[200] 依存症を経験したり、回復を経験したアーティストは、芸術を用いて「依存症の人間的な側面」を明らかにする形で、自らの経験を表現することがあります。依 存症と回復の経験を個人的なレベルに引き下げ、「私たちと彼ら」という区分を打ち破ることで、鑑賞者は、依存症に対する思いやりを示し、依存症に対する固 定観念や偏見を捨て、依存症を個人ではなく社会の問題として捉えるようになる可能性があります。[200] サントラ[200]によると、薬物使用障害の教育と予防においてアートをアドボカシーの手段として使用する主な目的には、以下のものが含まれる: 依存症アート展は多様な出典から生まれるが、これらの作品の根本的なメッセージは同じだ:知的負担の大きい事実や数字に依存せず、感情を通じて伝えること。これらの展覧会は、単独で存在したり、事実を補強したり、挑戦したりする可能性がある。 依存症を医学的疾患として認識し、理解を深めるための強力な教育ツール。個人的な体験談や画像を紹介する展示会は、依存症の研究者、依存症患者の家族や友人など、さまざまな観客に深い印象を与え、この問題の人間性を浮き彫りにすることで、共感と理解を促すことができます。 物質使用障害の偏見を排除し、それを道徳的欠陥として見るという社会の認識を、治療が必要な慢性疾患として理解する方向に転換する方法。 依存症と闘う人々に癒しの確信と励ましを提供し、彼らが孤独ではないことを伝える。 視覚芸術の活用は、医療システムにおける適切な物質使用治療、予防、教育プログラムやサービスの不足に注目を集めるのに役立ちます。メッセージは、政策決定者が連邦、州、地方レベルで依存症治療と予防に更多的資源を配分するよう促すことができます。 テンプル大学公衆衛生学部は、学生たちに芸術作品を作成してもらい、その作品を学生たちが作成したウェブサイトに掲載し、ソーシャルメディアで宣伝するこ とで、オピオイドの使用に関する認識を高め、それに関連する偏見を軽減するプロジェクトを実施した[201]。参加の程度を測定するために定量的および定 性的データが記録され、学生アーティストたちがインタビューを受けた結果、視点や理解の変化、多様な経験に対する理解の深まりが明らかになった。結局、こ のプロジェクトでは、芸術は作品制作を行うアーティストと作品と関わる人々の双方をエンパワーする効果的な媒体であることがわかった。[201] 別の著者は、先住民コミュニティと依存症に関するイデオロギーを「解体」し、「再構築」するために、文化的な景観を隠喩として用いて依存症を扱った現代カ ナダ人アーティストの作品を批判的に考察し、カナダにおける植民地時代の暴力がいかに先住民、その土地、薬物乱用との関係に深刻な影響を与えたかを明らか にした。[202] 「Voice」というプロジェクトは、依存症の経験を持つ女性たちが、ハームリダクションに対する女性の理解を探求し、スティグマの影響に挑み、これまで 沈黙を強いられてきた、あるいは軽視されてきた人たちに発言の場を与えることを目的とした、アート、詩、物語のコレクションです。[203] このプロジェクトでは、主流のシステム、美的感覚、フェミニズム、薬物使用に関する知識を持つ看護師が、週に一度の集まりを組織し、薬物使用や依存症の経 験を持つ女性たちが看護師と共に芸術的な表現を作成した。作品は、国際薬物関連危害会議、看護学会、地元のギャラリーなど複数の会場で展示され、地域社会 からポジティブな反応を得た。[203] |
★
Social scientific models Acute confusional state caused by alcohol withdrawal, otherwise known as delirium tremens Biopsychosocial–cultural–spiritual While regarded biomedically as a neuropsychological disorder, addiction is multi-layered, with biological, psychological, social, cultural, and spiritual (biopsychosocial–cultural–spiritual) elements.[204][205] A biopsychosocial–cultural–spiritual approach fosters the crossing of disciplinary boundaries, and promotes holistic considerations of addiction.[206][207][208] A biopsychosocial–cultural–spiritual approach considers, for example, how physical environments influence experiences, habits, and patterns of addiction. Ethnographic engagements and developments in fields of knowledge have contributed to biopsychosocial–cultural–spiritual understandings of addiction, including the work of Philippe Bourgois, whose fieldwork with street-level drug dealers in East Harlem highlights correlations between drug use and structural oppression in the United States.[209] Prior models that have informed the prevailing biopsychosocial–cultural–spiritual consideration of addiction include: |
社会科学モデル アルコール離脱による急性錯乱状態、別名「振戦せん妄」 生物心理社会的・文化的・精神的 生物医学的には神経心理学的障害とみなされている依存症は、生物学的、心理的、社会的、文化的、精神的(生物心理社会的・文化的・精神的)要素が複雑に絡 み合った多層的な問題です。[204][205] 生物心理社会的・文化的・精神的アプローチは、学問分野の境界を越えた連携を促進し、依存症の包括的な検討を促進する。[206][207][208] 生物心理社会的・文化的・精神的アプローチは、例えば、物理的環境が経験、習慣、依存症のパターンにどのように影響するかを考慮する。 エスノグラフィによる取り組みや知識分野の発展は、依存症の生物心理社会的・文化的・精神的な理解に貢献している。その一例として、イーストハーレムで街 頭での麻薬売人を対象としたフィールドワークを行い、米国における薬物使用と構造的抑圧との相関関係を明らかにしたフィリップ・ブルゴワの研究がある。 [209] 依存症に関する一般的な生物心理社会的・文化的・精神的な考察に影響を与えたこれまでのモデルには、次のようなものがある。 |
| Cultural model The cultural model, an anthropological understanding of the emergence of drug use and abuse, was developed by Dwight Heath.[210] Heath undertook ethnographic research and fieldwork with the Camba people of Bolivia from June 1956 to August 1957.[211] Heath observed that adult members of society drank 'large quantities of rum and became intoxicated for several contiguous days at least twice a month'.[210] This frequent, heavy drinking from which intoxication followed was typically undertaken socially, during festivals.[211] Having returned in 1989, Heath observed that while much had changed, 'drinking parties' remained, as per his initial observations, and 'there appear to be no harmful consequences to anyone'.[212] Heath's observations and interactions reflected that this form of social behavior, the habitual heavy consumption of alcohol, was encouraged and valued, enforcing social bonds in the Camba community.[211] Despite frequent intoxication, "even to the point of unconsciousness", the Camba held no concept of alcoholism (a form of addiction), and no visible social problems associated with drunkenness, or addiction, were apparent.[210] As noted by Merrill Singer, Heath's findings, when considered alongside subsequent cross-cultural experiences, challenged the perception that intoxication is socially 'inherently disruptive'.[210] Following this fieldwork, Heath proposed the 'cultural model', suggesting that 'problems' associated with heavy drinking, such as alcoholism – a recognised form addiction – were cultural: that is, that alcoholism is determined by cultural beliefs, and therefore varies among cultures. Heath's findings challenged the notion that 'continued use [of alcohol] is inexorably addictive and damaging to the consumer's health'.[211][210] The cultural model did face criticism by Sociologist Robin Room and others, who felt anthropologists could "downgrade the severity of the problem".[210] Merrill Singer found it notable that the ethnographers working within the prominence of the cultural model were part of the 'wet generation': while not blind to the 'disruptive, dysfunctional and debilitating effects of alcohol consumption', they were products 'socialized to view alcohol consumption as normal'.[210] |
文化モデル 薬物使用と乱用の出現に関する人類学的理解である文化モデルは、ドワイト・ヒースによって開発された[210]。ヒースは、1956年6月から1957年 8月まで、ボリビアのカンバ族について民族誌的研究とフィールドワークを行った[211]。ヒースは、社会の成人メンバーは「大量のラム酒を飲み、少なく とも月に2回は数日間続けて酩酊状態になる」ことを観察した。[210] この頻繁で過度の飲酒は、通常、祭りの際に社会的行事として行われていました。[211] 1989年に再訪したヒースは、多くの変化があったものの、「飲酒パーティー」は当初の観察通り残っており、「誰にも有害な影響はなさそう」と報告してい ます。[212] ヒースの観察と交流は、この社会的行動形態——習慣的な過度のアルコール摂取——が奨励され、価値あるものとされ、カンバコミュニティの社会的絆を強化し ていることを反映していた。[211] 頻繁な酩酊状態——「意識を失うまで」——にもかかわらず、カンバにはアルコール依存症(依存症の一種)の概念はなく、酩酊や依存症に関連する目立った社 会的問題は認められなかった。[210] メリル・シンガーが指摘するように、ヒースの発見は、その後の文化間比較研究と併せて検討されると、酩酊が社会的に「本質的に破壊的」であるという認識に 疑問を投げかけた。[210] このフィールドワークの後、ヒースは「文化モデル」を提唱し、アルコール依存症(依存症の一形態として認識されている)を含む過度の飲酒に関連する「問 題」は文化的である、つまりアルコール依存症は文化的信念によって決定され、したがって文化間で異なるものだと主張した。ヒースの発見は、「(アルコール の)継続的な使用は、必然的に依存症を引き起こし、消費者の健康を損なう」という概念に異議を唱えた。[211][210] 文化モデルは、人類学者が「問題の深刻さを軽視している」と批判した社会学者ロビン・ルームらから批判を受けた。[210] メリル・シンガーは、文化モデルを支持するエスノグラファーたちが「ウェット世代」の一員である点を注目すべきだと指摘した。彼らは「アルコール消費の破 壊的、機能不全的、衰弱させる影響」に目をつぶっているわけではないが、「アルコール消費を正常とみなすように社会化された」産物である。[210] |
| Subcultural model Historically, addiction has been viewed from the etic perspective, defining users through the pathology of their condition.[213] As reports of drug use rapidly increased, the cultural model found application in anthropological research exploring western drug subculture practices.[210] The approach evolved from the ethnographic exploration into the lived experiences and subjectivities of 1960s and 1970s drug subcultures.[210] The seminal publication "Taking care of business", by Edward Preble and John J. Casey, documented the daily lives of New York street-based intravenous heroin users in rich detail, providing unique insight into the dynamic social worlds and activities that surrounded their drug use.[214] These findings challenge popular narratives of immorality and deviance, conceptualizing substance abuse as a social phenomenon. The prevailing culture can have a greater influence on drug taking behaviors than the physical and psychological effects of the drug itself.[215][better source needed] To marginalized individuals, drug subcultures can provide social connection, symbolic meaning, and socially constructed purpose that they may feel is unattainable through conventional means.[215] The subcultural model demonstrates the complexities of addiction, highlighting the need for an integrated approach. It contends that a biosocial approach is required to achieve a holistic understanding of addiction.[210] |
サブカルチャーモデル 歴史的に、依存症は、その状態の病理によって使用者を定義する、倫理的観点から捉えられてきました[213]。薬物使用に関する報告が急速に増加するにつれて、文化モデルは、西洋の薬物サブカルチャーの慣習を探求する人類学的研究に応用されるようになりました[210]。 このアプローチは、1960年代および1970年代の薬物サブカルチャーの生活体験や主観性に関する民族誌的探求から発展したものです。[210] エドワード・プレブルとジョン・J・ケイシーの画期的な著作『Taking care of business』は、ニューヨークの街頭で静脈注射によるヘロイン使用者の日常を詳細に記録し、彼らの薬物使用を取り巻く動的な社会世界と活動に関する 独自の洞察を提供した。[214] これらの発見は、道徳的欠如や逸脱といった一般的な物語を覆し、物質乱用を社会的現象として概念化した。一般的な文化は、薬物そのものの物理的および心理 的影響よりも、薬物使用行動に大きな影響を与える可能性がある。[215][より良い情報源が必要] 疎外された個人にとって、薬物サブカルチャーは、従来の手段では達成できないと感じるかもしれない社会的つながり、象徴的な意味、および社会的に構築され た目的を提供することができる。[215] サブカルチャーモデルは、依存症の複雑さを示し、統合的なアプローチの必要性を強調している。このモデルは、依存症の包括的な理解を達成するためには、生 物社会学的アプローチが必要であると主張している。[210] |
| Critical medical anthropology model Emerging in the early 1980s, the critical medical anthropology model was introduced, and as Merrill Singer offers 'was applied quickly to the analysis of drug use'.[210] Where the cultural model of the 1950s looked at the social body, the critical medical anthropology model revealed the body politic, considering drug use and addiction within the context of macro level structures including larger political systems, economic inequalities, and the institutional power held over social processes.[210] Highly relevant to addiction, the three issues emphasized in the model are: Self-medication The social production of suffering The political economy (Licit and Illicit Drugs)[210] These three key points highlight how drugs may come to be used to self-medicate the psychological trauma of socio-political disparity and injustice, intertwining with licit and illicit drug market politics.[210] Social suffering, "the misery among those on the weaker end of power relations in terms of physical health, mental health and lived experience", is used by anthropologists to analyze how individuals may have personal problems caused by political and economic power.[210] From the perspective of critical medical anthropology heavy drug use and addiction is a consequence of such larger scale unequal distributions of power.[210] The three models developed here – the cultural model, the subcultural model, and the Critical Medical Anthropology Model – display how addiction is not an experience to be considered only biomedically. Through consideration of addiction alongside the biological, psychological, social, cultural and spiritual (biopsychosocial–spiritual) elements which influence its experience, a holistic and comprehensive understanding can be built. |
批判的医療人類学モデル 1980年代初頭に登場した批判的医療人類学モデルは、メリル・シンガーが指摘するように、「薬物使用の分析に迅速に適用された」。[210] 1950年代の文化モデルが「社会的身体」に注目したのに対し、批判的医療人類学モデルは「政治的身体」を明らかにし、薬物使用と依存を、より大きな政治 システム、経済的不平等、社会プロセスに対する制度的権力を含むマクロレベルの構造の文脈の中で検討した。[210] 依存症と関連性の高い、このモデルで強調されている 3 つの問題は次のとおりです。 自己治療 苦悩の社会的生産 政治経済(合法薬物と違法薬物)[210] この 3 つの重要なポイントは、社会政治的格差や不正による心理的トラウマを自己治療するために薬物が使用され、合法薬物と違法薬物の市場政治と絡み合う仕組みを 浮き彫りにしています。[210] 社会的苦悩、「身体的健康、精神的健康、および生きた経験の面で、権力関係において弱い立場にある者たちの苦しみ」は、人類学者によって、個人が政治的・ 経済的権力によって引き起こされる個人的な問題を抱えるようになる仕組みを分析するために用いられている[210]。批判的医療人類学の観点からは、重度 の薬物使用および依存症は、このような大規模な権力の不平等な分配の結果である[210]。 ここで開発された3つのモデル——文化モデル、サブカルチャーモデル、批判的医療人類学モデル——は、依存症が生物医学的にのみ考慮すべき経験ではないこ とを示している。依存症の経験に影響を与える生物学的、心理的、社会的、文化的、精神的(生物心理社会的・精神的)要素を併せて考慮することで、包括的で 総合的な理解を構築することができる。 |
| Social learning models Social learning theory Main article: Social learning theory Albert Bandura's 1977 social learning theory posits that individuals acquire addictive behaviors by observing and imitating models in their social environment.[216][217] The likelihood of engaging in and sustaining similar addictive behaviors is influenced by the reinforcement and punishment observed in others. The principle of reciprocal determinism suggests that the functional relationships between personal, environmental, and behavioral factors act as determinants of addictive behavior.[218] Thus, effective treatment targets each dynamic facet of the biopsychosocial disorder. |
社会的学習モデル 社会的学習理論 主な記事:社会的学習理論 アルバート・バンデューラの 1977 年の社会的学習理論は、個人は社会的環境におけるモデルを観察し、模倣することで依存症的な行動を獲得すると提唱している。[216][217] 同様の依存症的な行動に従事し、それを維持する可能性は、他者に見られる強化や罰の影響を受ける。相互決定の原則は、人格、環境、行動の要因間の機能的関 係が、依存症行動の決定要因として機能することを示唆している。[218] したがって、効果的な治療は、生物心理社会的障害の動的な側面それぞれを対象とする必要がある。 |
| Transtheoretical model (stages of change model) Main article: Transtheoretical model The transtheoretical model of change suggests that overcoming an addiction is a stepwise process that occurs through several stages.[219] Precontemplation: This initial stage precedes individuals considering a change in their behavior. They might be oblivious to or in denial of their addiction, failing to recognize the need for change. Contemplation is the stage in which individuals become aware of the problems caused by their addiction and are considering change. Although they may not fully commit, they weigh the costs and benefits of making a shift. Preparation: Individuals in this stage are getting ready to change. They might have taken preliminary steps, like gathering information or making small commitments, in preparation for behavioral change. Action involves actively modifying behavior by making specific, observable changes to address the addictive behavior. The action stage requires significant effort and commitment. Maintenance: After successfully implementing a change, individuals enter the maintenance stage, where they work to sustain the new behavior and prevent relapse. This stage is characterized by ongoing effort and consolidation of gains. Termination/relapse prevention: Recognizing that relapse is a common part of the change process, this stage focuses on identifying and addressing factors that may lead to a return to old behaviors. Relapse is viewed as an opportunity for learning and strategy adjustment, with the ultimate goal of eliminating or terminating the targeted behavior. The transtheoretical model can be helpful in guiding development of tailored behavioral interventions that can promote lasting change. Progression through these stages may not always follow a linear path, as individuals may move back and forth between stages. Resistance to change is recognized as an expected part of the process. Addiction causes an "astoundingly high financial and human toll" on individuals and society as a whole.[220][153][156] In the United States, the total economic cost to society is greater than that of all types of diabetes and all cancers combined.[156] These costs arise from the direct adverse effects of drugs and associated healthcare costs (e.g., emergency medical services and outpatient and inpatient care), long-term complications (e.g., lung cancer from smoking tobacco products, liver cirrhosis and dementia from chronic alcohol consumption, and meth mouth from methamphetamine use), the loss of productivity and associated welfare costs, fatal and non-fatal accidents (e.g., traffic collisions), suicides, homicides, and incarceration, among others.[220][153][156][221] The US National Institute on Drug Abuse has found that overdose deaths in the US have almost tripled among males and females from 2002 to 2017, with 72,306 overdose deaths reported in 2017 in the US.[222] 2020 marked the year with the highest number of overdose deaths over a 12-month period, with 81,000 overdose deaths, exceeding the records set in 2017.[223] |
トランス理論的モデル(変化の段階モデル) 主な記事:トランス理論的モデル トランス理論的変化モデルは、依存症を克服することは、いくつかの段階を経て段階的に進行するプロセスであると示唆している。[219] 事前検討段階:この初期段階は、個人が行動の変化を検討する前に訪れる段階である。依存症に気づいていない、あるいは依存症を否定しており、変化の必要性を認識していない場合がある。 検討段階:この段階では、個人が依存症が引き起こす問題に気づき、変化を検討し始める。彼らは完全にコミットしていないかもしれないが、変化のコストと利益を天秤にかける。 準備段階:この段階の個人は、変化の準備を進めている。彼らは、行動変化の準備として、情報収集や小さなコミットメントなど、初期段階のステップを踏み出しているかもしれない。 行動段階では、依存行動に対処するために、具体的かつ観察可能な変化を起こし、積極的に行動を改めます。行動段階では、大きな努力とコミットメントが必要です。 維持段階:変化を成功裏に実施した後、個人は維持段階に入り、新しい行動を維持し、再発を防ぐための努力を続けます。この段階は、継続的な努力と成果の定着が特徴です。 終了/再発防止:再発は変化のプロセスでよくあることだと認識し、この段階では、古い行動に戻る原因となる要因を特定し、それに対処することに重点が置かれる。再発は、学習と戦略の調整の機会とみなされ、最終的な目標は、対象とする行動の排除または終了だ。 理論的モデル は、持続的な変化を促進する、個々に合わせた行動介入の開発を指導する上で役立つ。これらの段階の進行は必ずしも直線的ではなく、個人が段階の間を行き来する場合もある。変化への抵抗は、プロセスの一部として予想されるものと認識されている。 依存症は、個人および社会全体に「驚くべき高い経済的・人的コスト」をもたらす。[220][153][156] 米国では、社会全体の経済的コストは、すべての種類の糖尿病とすべての癌を合わせたものよりも大きい。[156] これらのコストは、薬物の直接的な有害影響と関連する医療費(例:救急医療サービス、外来・入院治療)、長期的な合併症(例:タバコ製品による肺がん、慢 性アルコール摂取による肝硬変と認知症、メタンフェタミン使用によるメタンフェタミン口内症)、生産性の喪失と関連する福祉コスト、致命的な事故と非致命 的な事故(例:[220][153][156][221] 米国国立薬物乱用研究所は、2002 年から 2017 年にかけて、米国の過剰摂取による死亡者数が男性、女性ともに 3 倍近くに増加しており、2017 年には 72,306 人の過剰摂取による死亡者が報告されていることを明らかにしている。[222] 2020年は、12ヶ月間の過剰摂取による死亡者数が最も多かった年で、81,000人の過剰摂取による死亡が報告され、2017年の記録を突破した。 [223] |
| Autonomic nervous system Binge drinking Binge eating disorder Cognitive liberty Darwinian hedonism Discrimination against drug addicts Dopaminergic pathways Pavlovian-instrumental transfer Philosophy of medicine Substance dependence |
自律神経系 過度の飲酒 過食症 認知の自由 ダーウィニアン快楽主義 薬物依存者に対する差別 ドーパミン作動経路 パブロフの道具的転移 医学哲学 物質依存 |
| Further reading Pelchat ML (March 2009). "Food Addiction in Humans". The Journal of Nutrition. 139 (3): 620–622. doi:10.3945/jn.108.097816. PMID 19176747. Gordon HW (April 2016). "Laterality of Brain Activation for Risk Factors of Addiction". Current Drug Abuse Reviews. 9 (1): 1–18. doi:10.2174/1874473709666151217121309. PMC 4811731. PMID 26674074. Szalavitz M (2016). Unbroken Brain. St. Martin's Press. ISBN 978-1-250-05582-8. Courtwright DT (2019). The Age of Addiction: How Bad Habits Became Big Business. Cambridge, Massachusetts: Harvard University Press. ISBN 9780674248229. |
さらに読む Pelchat ML (2009年3月). 「ヒトにおける食物依存症」. The Journal of Nutrition. 139 (3): 620–622. doi:10.3945/jn.108.097816. PMID 19176747. Gordon HW (2016年4月). 「依存症の危険因子に関する脳活動の左右差」. Current Drug Abuse Reviews. 9 (1): 1–18. doi:10.2174/1874473709666151217121309. PMC 4811731. PMID 26674074. Szalavitz M (2016). Unbroken Brain. セント・マーティンズ・プレス。ISBN 978-1-250-05582-8。 Courtwright DT (2019). The Age of Addiction: How Bad Habits Became Big Business. マサチューセッツ州ケンブリッジ: ハーバード大学出版局。ISBN 9780674248229。 |
| https://en.wikipedia.org/wiki/Addiction |
リ ンク
文 献
そ の他の情報
CC
Copyleft, CC, Mitzub'ixi Quq Chi'j, 1996-2099
![]()
☆
 ☆
☆