Global
Aging
Global
Aging
☆「世界中で人々は長生きするようになっ
ている。今日では、ほとんどの人々が60代、あるいはそれ以降まで生きられると期待できる。世界中の国々で、高齢者の人口規模と割合の両方が増加してい
る。
2030年までに、世界の6人に1人が60歳以上となる。この時点で、60歳以上の人口の割合は、2020年の10億人から14億人に増加する。2050
年には、60歳以上の人口は2倍(21億人)に増加する。80歳以上の人口は、2020年から2050年の間に3倍に増加し、4億2600万人に達すると
予想されている。
この高齢化と呼ばれる人口分布の高齢化は、高所得国(例えば、日本の人口の30%はすでに60歳以上である)で始まったが、現在では低・中所得国が最も大
きな変化を経験している。2050年までに、60歳以上の世界の人口の3分の2が低・中所得国に住むことになる」(国連「」)。
★NIH(国立衛生研究所)の下部組織で あるNIA(国立エイジング研究所)のHPより
| Global Aging NIA supports research and resources to facilitate behavioral and social research on the life course, aging, and Alzheimer’s disease and Alzheimer’s disease-related dementias (AD/ADRD) globally. |
グローバルエイジング NIAは、ライフコース、老化、アルツハイマー病およびアルツハイマー病関連認知症(AD/ADRD)に関する行動および社会研究を世界的に促進するため の研究およびリソースを支援している。 |
| Global Aging Behavioral &
Social Research Overview Increasing longevity and declining fertility lead to population aging and a shift in the age distribution of a population. Such a shift has implications for individuals, families, and societies as governments and other institutions seek to answer questions related to health care, housing, pension programs, work and retirement, and caregiving. Research is needed to guide key program and policy decisions. The Division of Behavioral and Social Research (BSR) at NIA supports research on life course health and well-being, including AD/ADRD. Conducting research on aging and the life course in international settings provides opportunities to study geographic areas that vary socially, economically, and culturally. This type of research can help us better understand how aging in different institutional, policy, environmental, economic, social, and cultural contexts can lead to different health and welfare outcomes for individuals and populations, including those related to AD/ADRD. The cross-national laboratory provides opportunities to examine differences in national and regional policies in ways that studies of specific countries cannot. This information can inform interventions and policies in the United States and globally to improve population health. BSR has played a leadership role in global aging research through its work with partners in academia, government, foundations, and other research-supporting agencies. Notably, the NIA-funded Health and Retirement Study (HRS) has served as the model for large-scale nationally representative longitudinal studies in other countries. Key areas of research emphasis include, but are not limited to: Improve understanding of how aging in different international contexts mitigates or exacerbates health disparities in aging Comparative studies of how differences in institutional and policy features of health care provision and financing influence access, utilization, and health outcomes across the life course and at older ages Comparative dementia and dementia care research in different environmental, economic, social, and cultural contexts Development of multilevel, multidisciplinary, longitudinal data with cognitive measures coupled with biomarkers and administrative data to facilitate cross-national studies of aging and dementia Analyses of population-based data to inform improvements in informal and formal caregiving and dementia care These priorities are based on BSR’s broader research priorities, which are outlined in the NIA Strategic Directions for Research, 2020-2025 (PDF, 3M); NACA 2019 BSR Review Committee Report (PDF, 433K); AD & ADRD Research Implementation Epidemiology/Population Studies Milestones; and Understanding the Role of the Exposome in Brain Aging, AD & ADRD workshop summary (PDF, 661K). BSR is particularly committed to studies that help us improve our understanding in low- and middle-income countries because aging research in these countries has been limited. |
グローバル・エイジング 行動・社会研究の概要 長寿化と少子化は人口の高齢化と人口の年齢分布の変化につながる。このような変化は、政府やその他の機関が保健医療、住宅、年金制度、労働と退職、介護に 関する問題への対応を迫られるため、個人、家族、社会に影響を及ぼす。主要なプログラムや政策決定の指針となる研究が必要とされている。 NIAの行動・社会科学研究部(BSR)は、アルツハイマー病およびアルツハイマー病性認知症(AD/ADRD)を含む生涯の健康と幸福に関する研究を支 援している。国際的な環境における加齢と生涯の研究を実施することは、社会、経済、文化的に異なる地理的領域を研究する機会を提供する。この種の研究は、 異なる制度、政策、環境、経済、社会、文化的な背景における高齢化が、アルツハイマー病や認知症を含む個人や集団の保健や福祉にどのような影響をもたらす かをより深く理解するのに役立つ。 国際的な研究施設は、特定の国々を対象とした研究では不可能な方法で、国や地域ごとの政策の違いを調査する機会を提供する。 この情報は、米国および世界規模での介入や政策に役立てられ、国民の健康の改善に貢献する。 BSRは、学術界、政府、財団、その他の研究支援機関のパートナーとの協力により、世界的な高齢化研究において指導的役割を果たしてきた。特に、NIAが 資金提供する健康と退職に関する研究(HRS)は、他の国々における大規模な国民代表縦断的研究のモデルとなっている。 主な研究重点分野には、以下が含まれるが、これらに限定されるものではない。 異なる国際的背景における高齢化が、高齢化における健康格差を緩和または悪化させる仕組みについての理解を深める 医療提供と資金調達の制度や政策の特徴の違いが、生涯を通じて、また高齢期におけるアクセス、利用、健康結果にどのような影響を与えるかについての比較研 究 異なる環境、経済、社会、文化的な背景における認知症と認知症ケアの比較研究 認知機能測定とバイオマーカー、行政データを組み合わせた多層的、学際的、縦断的データの開発による、高齢化と認知症に関する国際比較研究の促進 非公式および公式の介護と認知症ケアの改善に役立てるための、人口ベースのデータの分析 これらの優先事項は、BSRのより広範な研究優先事項に基づいており、これらは「NIA Strategic Directions for Research, 2020-2025(PDF、3M)」、「NACA 2019 BSR Review Committee Report(PDF、433K)」、 AD & ADRD研究実施の疫学/人口学研究マイルストーン、および脳の老化、AD & ADRDワークショップのまとめ(PDF、661K)におけるエクスポソームの役割の理解。 BSRは、特に低・中所得国における理解を深める研究に力を入れている。なぜなら、これらの国々における老化研究は限られていたからだ。 |
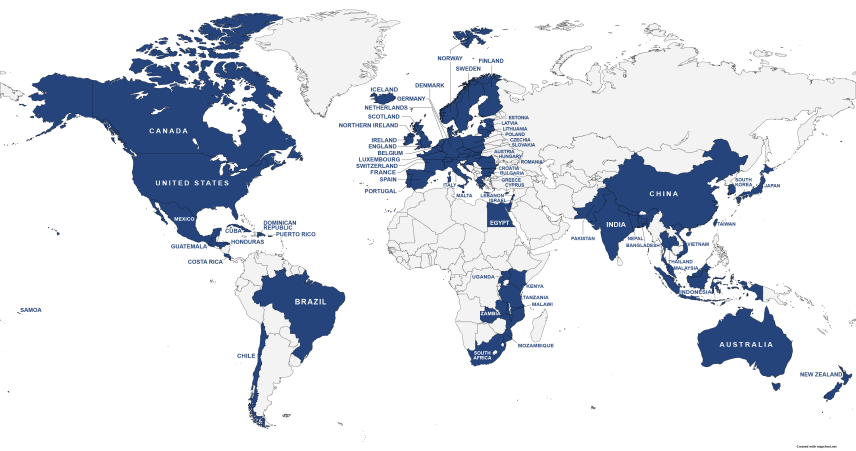 Please update the text underneath to the following: The map highlights countries in blue where NIA supports behavioral and social research including: United States, Australia, Austria, Bangladesh, Belgium, Bulgaria, Brazil, Canada, Chile, China, Costa Rica, Croatia, Cuba, Cyprus, Czechia, Denmark, Dominican Republic, Egypt, England, Estonia, Finland, France, Germany, Greece, Guatemala, Honduras, Hungary, Iceland, India, Indonesia, Ireland, Israel, Italy, Japan, Kenya, Latvia, Lebanon, Lithuania, Luxembourg, Malawi, Malaysia, Malta, Mexico, Mozambique, Nepal, Netherlands, New Zealand, Northern Ireland, Norway, Pakistan, Poland, Portugal, Puerto Rico, Romania, Samoa, Scotland, Slovakia, South Africa, South Korea, Spain, Sweden, Switzerland, Taiwan, Tanzania, Thailand, Uganda, Vietnam, Zambia. |
以下のテキストを以下の内容に更新する。地図では、NIAが支援する行動および社会研究を実施している国を青でハイライトしている。米国、オーストラリ ア、オーストリア、バングラデシュ、ベルギー、ブルガリア、ブラジル、カナダ、チリ、中国、コスタリカ、クロアチア、キューバ、キプロス、チェコ、デン マーク、ドミニカ共和国、エジプト、イングランド、エストニア、フィンランド、フランス、ドイツ、ギリシャ、グアテマラ、ホンジュラス、ハンガリー、アイ スランド、インド、インドネシア、アイルランド、イスラエル、イタリア、日本、ケニア、 ラトビア、レバノン、リトアニア、ルクセンブルク、マラウイ、マレーシア、マルタ、メキシコ、モザンビーク、ネパール、オランダ、ニュージーランド、北ア イルランド、ノルウェー、パキスタン、ポーランド、ポルトガル、プエルトリコ、ルーマニア、サモア、スコットランド、スロバキア、南アフリカ、韓国、スペ イン、スウェーデン、スイス、台湾、タンザニア、タイ、ウガンダ、ベトナム、ザンビア。 |
| https://www.nia.nih.gov/research/dbsr/global-aging |
★国連のグローバル・エイジングに対する 対応("Ageing and health"より)
| Key facts All countries face major challenges to ensure that their health and social systems are ready to make the most of this demographic shift. In 2050, 80% of older people will be living in low- and middle-income countries. The pace of population ageing is much faster than in the past. In 2020, the number of people aged 60 years and older outnumbered children younger than 5 years. Between 2015 and 2050, the proportion of the world's population over 60 years will nearly double from 12% to 22%. |
主な事実 すべての国が、この人口動態の変化を最大限に活用できるよう、保健・社会制度を整備するという大きな課題に直面している。 2050年には、高齢者の80%が低・中所得国で暮らすことになる。 人口の高齢化のペースは、過去よりもはるかに速い。 2020年には、60歳以上の人口が5歳未満の子供の人口を上回った。 2015年から2050年の間に、60歳以上の人口の割合は12%から22%へとほぼ倍増する。 |
| Overview People worldwide are living longer. Today most people can expect to live into their sixties and beyond. Every country in the world is experiencing growth in both the size and the proportion of older persons in the population. By 2030, 1 in 6 people in the world will be aged 60 years or over. At this time the share of the population aged 60 years and over will increase from 1 billion in 2020 to 1.4 billion. By 2050, the world’s population of people aged 60 years and older will double (2.1 billion). The number of persons aged 80 years or older is expected to triple between 2020 and 2050 to reach 426 million. While this shift in distribution of a country's population towards older ages – known as population ageing – started in high-income countries (for example in Japan 30% of the population is already over 60 years old), it is now low- and middle-income countries that are experiencing the greatest change. By 2050, two-thirds of the world’s population over 60 years will live in low- and middle-income countries. |
概要 世界中で人々は長生きするようになっている。今日では、ほとんどの人々が60代、あるいはそれ以降まで生きられると期待できる。世界中の国々で、高齢者の 人口規模と割合の両方が増加している。 2030年までに、世界の6人に1人が60歳以上となる。この時点で、60歳以上の人口の割合は、2020年の10億人から14億人に増加する。2050 年には、60歳以上の人口は2倍(21億人)に増加する。80歳以上の人口は、2020年から2050年の間に3倍に増加し、4億2600万人に達すると 予想されている。 この高齢化と呼ばれる人口分布の高齢化は、高所得国(例えば、日本の人口の30%はすでに60歳以上である)で始まったが、現在では低・中所得国が最も大 きな変化を経験している。2050年までに、60歳以上の世界の人口の3分の2が低・中所得国に住むことになる。 |
| Ageing explained At the biological level, ageing results from the impact of the accumulation of a wide variety of molecular and cellular damage over time. This leads to a gradual decrease in physical and mental capacity, a growing risk of disease and ultimately death. These changes are neither linear nor consistent, and they are only loosely associated with a person’s age in years. The diversity seen in older age is not random. Beyond biological changes, ageing is often associated with other life transitions such as retirement, relocation to more appropriate housing and the death of friends and partners. |
加齢について 生物学的レベルでは、加齢は長年にわたる多種多様な分子および細胞の損傷の蓄積による影響の結果である。その結果、身体的および精神的能力が徐々に低下 し、病気のリスクが高まり、最終的には死に至る。これらの変化は直線的でも一貫性があるわけでもなく、その人の年齢と緩やかにしか関連していない。高齢期 に見られる多様性は、無作為なものではない。生物学的変化を超えて、老いは退職、より適切な住居への移転、友人やパートナーの死など、他の人生の転機と関 連していることが多い。 |
| Common health conditions
associated with ageing Common conditions in older age include hearing loss, cataracts and refractive errors, back and neck pain and osteoarthritis, chronic obstructive pulmonary disease, diabetes, depression and dementia. As people age, they are more likely to experience several conditions at the same time. Older age is also characterized by the emergence of several complex health states commonly called geriatric syndromes. They are often the consequence of multiple underlying factors and include frailty, urinary incontinence, falls, delirium and pressure ulcers. |
加齢に伴う一般的な保健状態 高齢期に多い症状には、難聴、白内障、屈折異常、腰痛や首の痛み、変形性関節症、慢性閉塞性肺疾患、糖尿病、うつ病、認知症などがある。高齢になるにつ れ、複数の症状を同時に経験する可能性が高くなる。 高齢期には、一般的に老年症候群と呼ばれるいくつかの複雑な保健状態が現れることも特徴である。これらは多くの場合、複数の基礎疾患の結果として起こり、 虚弱、尿失禁、転倒、せん妄、褥瘡などが含まれる。 |
| Factors influencing healthy
ageing A longer life brings with it opportunities, not only for older people and their families, but also for societies as a whole. Additional years provide the chance to pursue new activities such as further education, a new career or a long-neglected passion. Older people also contribute in many ways to their families and communities. Yet the extent of these opportunities and contributions depends heavily on one factor: health. Evidence suggests that the proportion of life in good health has remained broadly constant, implying that the additional years are in poor health. If people can experience these extra years of life in good health and if they live in a supportive environment, their ability to do the things they value will be little different from that of a younger person. If these added years are dominated by declines in physical and mental capacity, the implications for older people and for society are more negative. Although some of the variations in older people’s health are genetic, most is due to people’s physical and social environments – including their homes, neighbourhoods, and communities, as well as their personal characteristics – such as their sex, ethnicity, or socioeconomic status. The environments that people live in as children – or even as developing fetuses – combined with their personal characteristics, have long-term effects on how they age. Physical and social environments can affect health directly or through barriers or incentives that affect opportunities, decisions and health behaviour. Maintaining healthy behaviours throughout life, particularly eating a balanced diet, engaging in regular physical activity and refraining from tobacco use, all contribute to reducing the risk of non-communicable diseases, improving physical and mental capacity and delaying care dependency. Supportive physical and social environments also enable people to do what is important to them, despite losses in capacity. The availability of safe and accessible public buildings and transport, and places that are easy to walk around, are examples of supportive environments. In developing a public-health response to ageing, it is important not just to consider individual and environmental approaches that ameliorate the losses associated with older age, but also those that may reinforce recovery, adaptation and psychosocial growth. |
健康な高齢期に影響を与える要因 寿命が延びることは、高齢者とその家族だけでなく、社会全体にとってもチャンスをもたらす。 余命が延びれば、さらなる教育や新たなキャリア、長年忘れていた情熱など、新たな活動に挑戦するチャンスが生まれる。 高齢者はまた、家族や地域社会にもさまざまな形で貢献している。 しかし、こうしたチャンスや貢献の度合いは、ある一つの要因に大きく左右される。 証拠によると、健康な状態で過ごす割合はほぼ一定であることが示唆されており、これは健康でない状態で過ごす年数が加わっていることを意味している。人々 が健康な状態で余命を過ごすことができ、支援的な環境で暮らすことができるのであれば、価値あることを行う能力は若い人とほとんど変わらないだろう。これ らの余命が身体的および精神的能力の低下によって占められるのであれば、高齢者および社会にとっての含意はより否定的なものとなる。 高齢者の健康状態の変化には遺伝的なものもあるが、大半は、家庭、近隣、地域社会などの物理的・社会的環境、および性別、民族、社会経済的地位などの個人 の特性に起因する。子供時代、あるいは胎児期に育った環境と個人の特性が組み合わさり、その人の加齢に長期的な影響を与える。 物理的および社会的環境は、機会、意思決定、健康行動に影響を与える障壁やインセンティブを通じて、あるいは直接的に、保健に影響を与える可能性がある。 生涯を通じて健康的な行動を維持すること、特にバランスのとれた食事、定期的な運動、禁煙は、すべて非感染性疾患のリスクを低減し、身体的および精神的機 能を向上させ、介護依存を遅らせることに貢献する。 また、身体面および社会面での支援的な環境は、能力の低下にもかかわらず、人々が自分にとって重要なことを行うことを可能にする。安全で利用しやすい公共 施設や交通機関、歩きやすい場所などが、支援的な環境の例である。高齢化に対する公衆衛生の対応策を講じるにあたっては、高齢化に伴う損失を改善する個人 および環境面のアプローチを検討するだけでなく、回復、適応、心理社会的成長を強化する可能性のあるアプローチも検討することが重要である。 |
| Challenges in responding to
population ageing There is no typical older person. Some 80-year-olds have physical and mental capacities similar to many 30-year-olds. Other people experience significant declines in capacities at much younger ages. A comprehensive public health response must address this wide range of older people’s experiences and needs. The diversity seen in older age is not random. A large part arises from people’s physical and social environments and the impact of these environments on their opportunities and health behaviour. The relationship we have with our environments is skewed by personal characteristics such as the family we were born into, our sex and our ethnicity, leading to inequalities in health. Older people are often assumed to be frail or dependent and a burden to society. Public health professionals, and society as a whole, need to address these and other ageist attitudes, which can lead to discrimination, affect the way policies are developed and the opportunities older people have to experience healthy aging. Globalization, technological developments (e.g., in transport and communication), urbanization, migration and changing gender norms are influencing the lives of older people in direct and indirect ways. A public health response must take stock of these current and projected trends and frame policies accordingly. |
高齢化への対応における課題 高齢者には典型的な人物はいない。80歳でも、心身ともに30歳と変わらない能力を持つ人もいる。一方で、はるかに若い年齢で著しく能力が低下する人もい る。包括的な公衆衛生対策では、こうした幅広い高齢者の経験やニーズに対応しなければならない。 高齢期に見られる多様性は、無作為に生じるものではない。その大部分は、人々の身体的および社会的環境、そしてそれらの環境が機会や健康行動に与える影響 から生じる。環境との関係は、出生時の家族、性別、民族性などの個人的特性によって歪められ、保健の不平等につながる。 高齢者はしばしば虚弱で依存的であり、社会の負担であると見なされる。公衆衛生の専門家や社会全体は、差別につながる可能性のある、こうした年齢差別的な 態度やその他の態度に対処する必要がある。また、政策の策定方法や高齢者が健康的に老後を過ごす機会にも影響を与える。 グローバル化、技術開発(輸送や通信など)、都市化、移住、ジェンダー規範の変化は、直接的・間接的に高齢者の生活に影響を与えている。公衆衛生対策で は、こうした現在の傾向と予測される傾向を把握し、それに応じて政策を策定する必要がある。 |
| WHO response The United Nations (UN) General Assembly declared 2021–2030 the UN Decade of Healthy Ageing and asked WHO to lead the implementation. The UN Decade of Healthy Ageing is a global collaboration bringing together governments, civil society, international agencies, professionals, academia, the media and the private sector for 10 years of concerted, catalytic and collaborative action to foster longer and healthier lives. The Decade builds on the WHO Global Strategy and Action Plan and the United Nations Madrid International Plan of Action on Ageing and supports the realization of the United Nations Agenda 2030 on Sustainable Development and the Sustainable Development Goals. The UN Decade of Healthy Ageing (2021–2030) seeks to reduce health inequities and improve the lives of older people, their families and communities through collective action in four areas: changing how we think, feel and act towards age and ageism; developing communities in ways that foster the abilities of older people; delivering person-centred integrated care and primary health services responsive to older people; and providing older people who need it with access to quality long-term care. |
WHOの対応 国連(UN)総会は、2021年から2030年を「健康な高齢化のための国連10年」と定め、その実施を主導するようWHOに要請した。健康な高齢化のた めの国連10年」は、より長く健康的な生活を促進するための10年間にわたる協調的、触媒的、協働的な行動を目的として、政府、市民社会、国際機関、専門 家、学術機関、メディア、民間部門を結集する世界的な取り組みである。 この10年は、WHOのグローバル戦略および行動計画、国連マドリード国際行動計画を基盤とし、国連持続可能な開発アジェンダ2030および持続可能な開 発目標の実現を支援する。 国連健康長寿の10年(2021年~2030年)は、以下の4つの分野における集団行動を通じて、保健格差の縮小と高齢者、その家族、地域社会の生活の改 善を目指す。高齢化や高齢者差別に対する考え方、感じ方、行動の変化、高齢者の能力を育む方法でのコミュニティ開発、高齢者に適した人格中心の統合ケアと プライマリーヘルスケアの提供、必要な高齢者への質の高い長期ケアへのアクセス提供、という4つの分野における集団行動を通じて、保健格差の縮小と高齢 者、その家族、コミュニティの生活改善を目指す。 |
| https://www.who.int/news-room/fact-sheets/detail/ageing-and-health |
★審問
【設問】あなたは、世界が直面している人 口集団の加齢現象(グローバル・エージング)において、まず、最初に取り組むべき課題はなんだと思いますか?また、その問題解決の見通しが見えた時点で の、次なる課題をどのように考えますか?
1.
2.
■クレジット:平成30年度グローバルエイジ
ング科研合同研究会、7月8日(日)1300-1800、首都大学東京・秋葉原サテライトキャンパス
リンク
サイト内リンク
文献
Mitzub'ixi Quq Chi'j
Copyleft, CC,
Mitzub'ixi Quq Chi'j, 1996-2099
Do not paste, but
[Re]Think our message for all undergraduate
students!!!
Copyleft, CC, Mitzub'ixi Quq Chi'j, 1996-2099
![]()
☆
 ☆
☆
{kind=link}