延命治療と功利主義
Life-prolonging Treatment and
Utilitarianism
☆ ヘア『道徳的に考えること』(10.4):ある末期癌の患者がいる。延命措置を講じないと、この患者はすぐ死ぬ。延命措置(ヘアの著作では「集中治療 intensive care」)をいまおこなえば、1か月後に苦 しみながら死ぬだろう。患者は、いま、延命治療の停止を強く望んでいる。医師は延命治療の手段を少しでも省くことには、嫌悪感を抱いている。ここでの医師 (=私)の選好は、患者のそれよりも弱い(ものとする)(佐藤 1994:67)。
| 合理的な道徳的推論 あるいは批判的思考(佐 藤 1994:67-68) | |
| 1)私は、延命治療をほどこされることを選好し、患者に延命治療をほど こすべきという判断に同意している。他方、患者は、延命治療をほどこされることを選好し、患者は延命治療をほどこすべきという判断には同意していない。私 の選好は、患者の選好よりも弱い。 | ・道徳的判断は指令的である(→それは普遍化可能である) |
| 2)私が患者の視点にたっても、両者がおかれている状況の普遍的性質に
関する差異は存在しない。したがって、普遍化可能性の論理の要請から、私はどちらの立場にいるにせよ、状況について同じ判断に同意できるのでなければなら
ない。 |
・価値判断は記述的 ・普遍的状況をかえずに、他者の立場に立つことを「私だったらどう思うのか?」と考えるのは誤りである。 ・普遍的状況をかえずに、他者の立場に立つことは、この要請はカントの定言命法と同じである。 ・つまり、私と他者が入れ替わっても、判断が変わる(→何が起こるか)といったことがあってはならない。 |
| 3)私が患者の立場にたてば、私は患者の選好を得るので、「患者は延命
治療を施されないこと」を選好する。 |
・条件的反省原理(conditional reflection
principle)にたつ(佐藤 1994:70) ・相手の立場に立つということは、相手を知るということだ。相手の経験や選好を想像し、現在の自分の中で再現するということだ。 ・延命措置にともなう「患者の嫌悪感」を等しく持つということ(Hare 1981:142,145)。 ・指令主義により、道徳的推論は規定される。それに反省原理がくわわり、選好功利主義が導かれる。 ・苦しんでいるひとが私自身であるかもしれないときに、私はある仮想的な指令を得る ・相手の立場にたつとは、相手を自分と同一視する |
| 4)司令説=司令主義の立場から、私は強く選好する事態がおこることを
指令する判断に同意するのでなければならない。 |
・価値判断は指令的である、その判断からはずれるとき、論理的に不誠実
である。 ・患者が「延命治療を施されないこと」を選好しているとき、患者は「それが最もよい」と判断し、私は、患者に同意しなければならない。 |
| 5)私の「患者が延命治療を施されること」に対する選好は、患者の視点
にたった私の「患者が延命治療を施されないこと」に対する選好よりも弱い。そのため、私は「患者は延命治療を施されるべきではない」という判断に同意しな
ければならない |
・論理的にみて、(普遍化に叶い)もっとも強い選好をえらぶべきという
判断が導かれる |
☆Advance care planning, ACP
| Advance care planning
is a process that enables individuals with decisional mental capacity
to make plans about their future health care.[1] Advance care plans
provide direction to healthcare professionals when a person is not in a
position to make and/or communicate their own healthcare choices.
Advance care planning is applicable to adults at all stages of life.[2] Participation in advance care planning has been shown to reduce stress and anxiety for patients and their families, and lead to improvements in end of life care.[3] Older adults are more directly concerned as they may experience a situation where advance care planning can be useful. However, only a small portion of elderly use them.[4][5] The main components of advance care planning include the nomination of a substitute decision maker, and the completion of an advance care directive. |
事前ケア計画(アドバンス・ケア・プランニング;ACP)とは、意思決
定能力を有する人格が将来の健康について計画を立てるプロセスである。[1]
事前ケア計画は、本人が自身の個人的な健康選択を決定・伝達できない状況において、医療従事者へ指針を提供する。事前ケア計画は人生のあらゆる段階にある
成人に適用可能である。[2] 事前ケア計画への参加は、患者とその家族のストレスや不安を軽減し、終末期ケアの改善につながることが示されている。[3] 高齢者は事前ケア計画が有用となる状況を経験する可能性が高いため、より直接的な関心事となる。しかし、高齢者のうち実際に利用する者はごく一部である。 [4][5] 事前ケア計画の主な構成要素には、代理意思決定者の指名と事前医療指示書の作成が含まれる。 |
| Definition Advance care planning was defined by an international white paper as involving individuals with decisional mental capacity at the outset, being able to be fully involved in plans and discussions about their health care.[1] This has led to some countries in the United Kingdom using 'Future Care Planning' [6][7] as an umbrella term, to include both advance care planning for those with capacity, and a planning for those with diminished or absent mental capacity (Best Interests decision making as defined by the UK Mental Capacity Act). Professor Mark Taubert, a palliative care consultant who is lead for Advance & Future Care Planning in Wales, published a position paper on this in 2022,[8] and NHS Scotland has also adopted Future Care Planning as an umbrella term, under which Advance Care Planning or Anticipatory Care planning are only a part-component. |
定義 事前ケア計画は、国際的な白書において、意思決定能力を有する個人が当初から関与し、自身の健康に関する計画や議論に完全に参加できるものと定義された。 [1] このため、英国の一部地域では「将来ケア計画」[6][7]を包括的用語として使用している。これは意思能力を有する者向けの事前ケア計画と、意思能力が 低下または喪失した者向けの計画(英国精神能力法で定義される最善の利益決定)の両方を包含する。ウェールズにおける事前・将来ケア計画の責任者である緩 和ケア専門医マーク・タウバート教授は2022年にこの件に関する見解書を公表した[8]。またNHSスコットランドも将来ケア計画を包括的用語として採 用しており、その下では事前ケア計画や予見的ケア計画は一部に過ぎない。 |
| Background Advance care planning may have relevance for adults at any stage of life.[2] Advance care planning typically involves a conversation between people, their families and carers and those looking after them about their future wishes and priorities for care.[9] However, notions of advance care planning vary internationally.[10] Advance care planning aims to allow people to live well, and when death approaches, die in accordance with their personal values.[11] Advance care planning is only applicable when the individual cannot make and/or communicate decisions about what they want in relation to their healthcare.[12] If advance care planning has occurred, patients who have lost capacity or the ability to communicate or both, are able to continue to have a say in their medical care.[13] This has been shown to improve end of life care, and provide improved outcomes for both patients and their surviving relatives.[3] While applicable to all stages of life, it is particularly applicable to perioperative planning and end-of-life care decision making, since approximately 1 in 4 people lose decision making capacity when approaching the end of their life.[14][15] Results of a systematic review indicate there are several prognostic indicators to help identify patients who may benefit from advance care planning discussions while still in the primary care setting.[16] Although ACP is potentially appropriate for nearly all adult patients, given the realities of a busy practice, it would be useful to have a system for identifying patients with a more limited prognosis. Federal and state legislation in the US,[17] Australia,[18] Canada[19] and the UK[20] supports the right of patients to refuse unwanted medical treatments. People can also express their preferences through written advance directives or by advising their appointed substitute decision maker about their wishes for when they are unable to make or communicate these decisions/wishes themselves. Increasingly digital approaches are emerging to support the documentation and sharing of advance care planning information, with the majority of approaches using electronic health record systems.[21] Whilst different approaches are emerging, there has been low uptake of digital advance care planning in countries including the UK.[22] Reasons for low uptake have been associated with implementation challenges experienced by health professionals, including interoperability challenges.[23] There is increasing recognition of the need for patients to have access to their own digital advance care plan to verify information stored about their care preferences.[24] |
背景 事前ケア計画は、人生のどの段階にある成人にも関連性がある。[2] 事前ケア計画は通常、本人、その家族や介護者、そしてケアを提供する者との間で、将来の希望やケアの優先順位について話し合うことを含む。[9] しかし、事前ケア計画の概念は国際的に異なる。[10] 事前ケア計画は、人民が良く生き、死が近づいた時には個人的な価値観に沿って死ぬことを可能にすることを目的とする。事前ケア計画は、個人が自身の医療に 関する意思決定や意思疎通ができなくなった場合にのみ適用される。[12] 事前ケア計画が実施されていれば、意思能力や意思疎通能力、あるいはその両方を失った患者も、医療ケアについて意見を表明し続けられる。[13] これは終末期ケアの質を向上させ、患者と遺族双方にとってより良い結果をもたらすことが示されている。[3] 人生の全段階に適用可能だが、特に周術期計画と終末期ケアの意思決定に有効である。なぜなら、人生の終末期に差し掛かる約4人のうち1人が意思決定能力を 失うからだ。[14][15] 系統的レビューの結果、一次医療現場において事前ケア計画の話し合いが有益な患者を特定する複数の予後指標が存在することが示されている。[16] ACPはほぼ全ての成人患者に適応し得るが、多忙な診療現場の現実を踏まえると、予後が限られている患者を特定するシステムの構築が有用である。 米国[17]、オーストラリア[18]、カナダ[19]、英国[20]の連邦・州法は、患者が望まない医療処置を拒否する権利を保障している。また、人民 は書面による事前指示書を通じて、あるいは自ら意思決定や意思伝達が不可能となった際の希望について、指名した代理意思決定者に伝えることで、自身の選好 を表明することもできる。 事前ケア計画情報の文書化と共有を支援するデジタル手法が台頭しつつあり、その大半は電子健康記録システムを利用している。[21] 異なる手法が生まれている一方で、英国を含む諸国ではデジタル事前ケア計画の導入率は低い。[22] 導入率の低さの背景には、医療従事者が直面する運用上の課題、特に相互運用性の問題が挙げられている。[23] 患者自身が自身のデジタル事前ケア計画にアクセスし、自身のケアに関する意思決定の希望が記録されている情報を確認できる必要性が、ますます認識されつつ ある。[24] |
| Components There are two methods by which the communication of an individual's preferences can be known. These are: the appointment of a substitute decision maker, and the completion of an advance care directive or similar document. Findings from a systematic review suggest the value and importance that various types of decision aids have for patients to use and help clarify their goals.[14] |
構成要素 個人の意思を伝える方法は二つある。それらは: 代理意思決定者の指名、および 事前医療指示書または類似の書類の作成である。 系統的レビューの結果は、様々な意思決定支援ツールが患者にとって有用であり、目標を明確化する上で重要であることを示唆している。[14] |
| Substitute decision maker Main article: Surrogate decision-maker A substitute decision maker makes decisions on behalf of an individual only when that individual does not have the capacity to make/communicate decisions for themselves.[25] There are a number of methods by which a substitute decision maker can be identified. The ideal method is the appointment of a person using a statutory document. In the absence of a statutory document the substitute decision maker may be a "person responsible" as listed in order of authority in legislation.[25] A substitute decision maker can be chosen by an individual following completion of relevant paperwork, can be assigned to the person by law in the absence of a chosen substitute decision maker (e.g. family member or carer), or can be appointed for the person (e.g. guardian appointed by a guardianship tribunal).[26] Substitute decision makers make decisions based on the principles of either substituted judgement or best interests.[2] Substituted judgement is when the substitute decision maker arrives at a decision based on the best approximation of what they believe the person would want. This decision should be informed by both the known wishes of the person and the best available healthcare advice.[27] Best interests decision making requires the substitute decision maker to focus on the patient's best interests. Many, but not all, jurisdictions have legislation supporting the appointment of a substitute decision maker through a statutory document. They have different names depending on the jurisdiction: 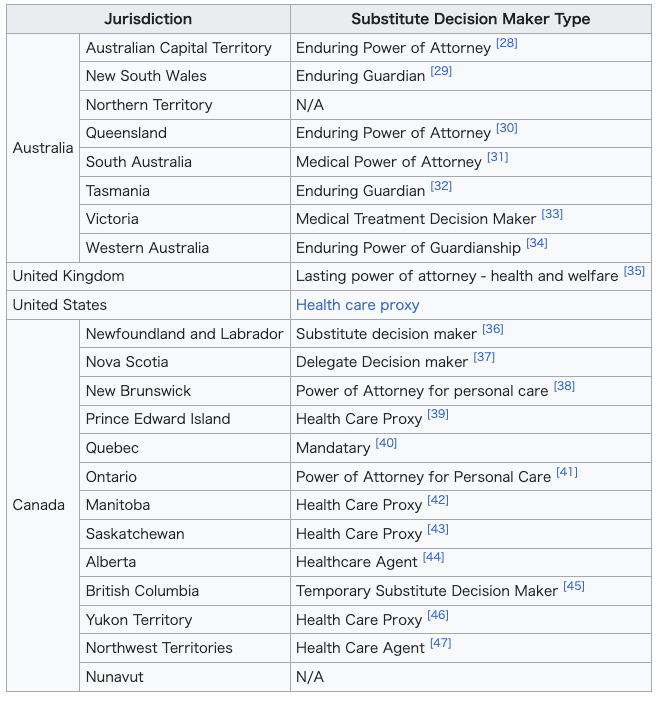 |
代理意思決定者 詳細な記事: 代理意思決定者 代理意思決定者は、本人が意思決定や意思伝達を行う能力を持たない場合に限り、本人に代わって意思決定を行う。[25] 代理意思決定者を特定する方法はいくつかある。理想的な方法は、法定文書を用いて人格を任命することだ。法定文書がない場合、代理意思決定者は法令に権限順に記載された「責任者」となる可能性がある。[25] 代理意思決定者は、本人が関連書類を完了した後に自ら選択することも、選択された代理意思決定者がいない場合に法律によって割り当てられることも(例:家族や介護者)、人格のために任命されることもある(例:後見人審判所によって任命された後見人)。[26] 代理意思決定者は、代替判断または最善の利益という原則に基づいて決定を行う。[2] 代替判断とは、代理意思決定者が人格が望むであろうことを最善に推測して決定を下す場合を指す。この決定は、人格の既知の意思と入手可能な最善の医療助言 の両方に基づいて行われるべきである。[27] 最善の利益に基づく意思決定では、代理意思決定者は患者の最善の利益に焦点を当てる必要がある。 多くの管轄区域では、法定文書による代理意思決定者の選任を支援する法律が存在するが、全てではない。管轄区域によって名称は異なる: |
| Advance care directives Main article: Advance health care directive An advance care directive is a document detailing an individual's health care preferences. This may include personal values and life goals, describe circumstances the person would find unacceptable, identify preferences relating to specific medical interventions, or a combination of these.[2] Advance care directives may be written on specifically designed forms, but can also take the form of a written letter or statement.[48] Inclusion of a doctor in the completion of an advance care directive will assist in ensuring that an individual's wishes are clear and written in a manner that is easy for substitute decision makers and/or medical staff to interpret and follow them in the future. Having a physician witness the document will reinforce this by showing future medical staff that the document contains information about informed decisions due to the assistance of a physician.[49] |
事前ケア指示書 詳細記事: 事前健康指示書 事前ケア指示書とは、個人の健康に関する希望を詳細に記した文書である。これには個人の個人的な価値観や人生の目標が含まれ、本人が受け入れられない状況の説明、特定の医療処置に関する希望の特定、あるいはこれらの組み合わせが含まれることがある。[2] 事前ケア指示書は専用の書式で作成されることもあるが、書面による手紙や声明の形を取ることも可能である。[48] 事前医療指示書の作成に医師を関与させることは、本人の意思が明確であり、将来的に代理意思決定者や医療スタッフが解釈・遵守しやすい形で記述されている ことを保証するのに役立つ。医師が文書に立会人として署名することは、将来の医療スタッフに対して、医師の支援による情報に基づいた意思決定の内容が文書 に含まれていることを示すことで、この効果を強化する。[49] |
| Advance Decisions to Refuse Treatment (United Kingdom) Some countries do not use the term 'directive', due to advance statements and/or advance care plans not usually having the legal standing to enforce a directive (for instance, a patient cannot direct a doctor to give him a specific treatment at a later time-point i.e. when she/he loses decisional capacity). In the United Kingdom, Advance Decisions, or Advance Decisions to Refuse Treatment (short: 'ADRT') have a legal standing under the UK Mental Capacity Act (2005). They can be written down and signed by patients. Such an ADRT must be specific about the treatment that is being refused and the circumstances in which the refusal will apply. To be valid, the person must have been competent and understood the decision when they signed the ADRT. Where the patient's advance decision relates to a refusal of potentially life-saving or life prolonging treatment, this must be recorded in writing and witnessed. Any advance refusal is legally binding, providing that the patient is an adult, the patient was competent and properly informed when reaching the prior decision. It is clearly applicable to the present circumstances and there is no reason to believe that the patient has changed their mind. If an advance decision does not meet these criteria but appears to set out a clear indication of the patient's wishes, it will not be legally binding but should be taken into consideration in determining the patient's best interests. An example of an ADRT is the national form and guidance published by NHS Wales on their Advance and Future Care Planning site.[50] |
治療拒否に関する事前決定(英国) 一部の国では「指示」という用語を使用しない。事前声明や事前ケア計画は通常、指示を強制する法的効力を有しないためである(例えば、患者は医師に対し、 特定の治療を後日(意思決定能力を失った時点など)に実施するよう指示することはできない)。英国では、事前決定、または治療拒否に関する事前決定(略 称:ADRT)は、英国精神能力法(2005年)の下で法的効力を有する。患者はこれを文書化し署名できる。このようなADRTは、拒否する治療内容と、 その拒否が適用される状況を具体的に明記しなければならない。有効であるためには、署名時点で人格が判断能力を有し、決定内容を理解していた必要がある。 患者の事前決定が生命維持・延命治療の拒否に関わる場合、書面による記録と立会人の署名が必要だ。事前拒否は、人格が成人であり、事前決定時に判断能力を 有し適切な説明を受けていた場合に限り法的拘束力を持つ。現在の状況に明らかに適用可能であり、患者が意思を変更したと信じる理由がない場合に限る。事前 決定がこれらの基準を満たさないが、患者の意思を明確に示すものと認められる場合、法的拘束力はないものの、患者の最善の利益を判断する際に考慮すべきで ある。ADRTの例としては、NHSウェールズが「事前・将来ケア計画」サイトで公開している全国共通様式とガイダンスがある。[50] |
| Benefits Research conducted in Switzerland with people aged 71 to 80 showed that better knowledge on advance care planning dispositions could improve the perception older people have of them. Communication on dispositions should take into account individual knowledge levels and address commonly enunciated barriers that seem to diminish with increased knowledge.[4] Adults with heart failure Advance care planning (ACP) may help to increase documentation by medical staff regarding discussions with participants, and improve an individual's depression.[51] This involves discussing an individual's future care plan in consideration of the individual's preferences and values. The findings are however, based on low-quality evidence as there is a need for further evidence from large studies to fully explore the effects of ACP for older adults.[51] Older people with frailty Advance care planning can effectively support older people with frailty to express what kind of healthcare they would prefer in the future. It can also improve the outcomes of healthcare received by elderly with frailty.[5][52] |
利点 スイスで71歳から80歳の人々を対象に行った研究では、事前ケア計画に関する知識が深まることで、高齢者の計画に対する認識が向上することが示された。 計画に関するコミュニケーションは、個人の知識レベルを考慮し、知識の増加に伴い減少する傾向にある障壁に対処すべきである。[4] 心不全の成人 事前ケア計画(ACP)は、医療スタッフによる参加者との話し合いの記録増加や、個人の抑うつ症状改善に寄与する可能性がある。[51] これは個人の希望や価値観を考慮した将来のケア計画について話し合うことを含む。ただし、高齢者に対するACPの効果を完全に解明するには大規模研究によ るさらなる証拠が必要であるため、この知見は低品質の証拠に基づくものである。[51] 虚弱な高齢者 事前ケア計画は、虚弱な高齢者が将来どのような医療を希望するかを表明する上で効果的に支援できる。また、虚弱な高齢者が受ける医療の成果を改善することもできる。[5][52] |
| References |
|
| https://en.wikipedia.org/wiki/Advance_care_planning |
|
★
☆ふろく:
★ 柏崎郁子『〈延命〉の倫理:医療と看護における』晃洋書房,2024年の検討
| 序章1 第一部 〈延命〉をめぐる医療と制度 |
|
| 第1章 〈延命〉と見做される医療 第1節 〈延命〉という概念、その起源と現代的用法 1)語義からみた〈延命〉 2)古典的vitalismからみた〈延命〉 3)あたらしいvitalismの趨勢 第2節 患者にとっての〈延命〉 1)不自然さへの嫌悪 2)医療化への抵抗 第3節 臨床では〈延命〉の何が問題とされるのか 1)〈延命〉の臨床 2)医療従事者は〈延命〉についてどう考えているか 第4節 小括 |
|
| 第2章 〈延命〉をめぐる争点 第1節 生命をめぐる争点―生命の神聖性と生命の質、生物学的生命と人格的生命 1)生命の神聖性と生命の質―カイザーリンク、クーゼ、ブロック 2)生物学的生命と人格的生命―エンゲルハート、トゥーリー、シンガー、ファインバーグ 第2節 「死の予期的状態」をめぐる争点 1)Dying―キャラハン 2)「死の予期的状態」は定義できない 3)厚生労働省における「死の予期的状態」の変遷 第3節 意思決定をめぐる争点―自律、自己決定、プライバシー 1)自律、自己決定、プライバシー―クインラン事件分析 2)自己決定の価値 第4節 小括 |
|
| 第3章 〈延命〉に対応する方法の展開 第1節 自己決定を実現するための方法―インフォームド・コンセント 1)インフォームド・コンセントの道徳原則と法 2)インフォームド・コンセントの歴史 3)インフォームド・コンセントの概念 第2節 自己決定ができなくなる事態に備える方法―事前指示 1)カトナーによるリビング・ウィルの提案 2)事前指示の問題点―SUPPORT研究 第3節 事前指示の欠点を克服する方法―ACP:権利から統治へ 1)国家のACPへの信頼と期待 2)日本のACP 3)医学的無益性 第4節 小括 |
|
| 第4章 〈延命〉という問題に応じるための保健医療福祉政策 第1節 介護保険制度 1)介護というカテゴリーの誕生 2)「福祉のターミナルケア」論争 第2節 「健康増進法」と「社会保障制度改革推進法」 1)健康寿命 2)社会保障制度の改革 第3節 あたらしい公衆衛生と「終末期」ケアの融合 1)緩和ケアの公衆衛生への包摂 2)地域包括ケアシステムとACP 第4節 小括 第二部 〈延命〉をめぐる看護とその倫理 |
|
| 第5章 看護実践のアイデンティティをめぐる争点 第1節 看護師が行う看護という概念の構築 1)米国における看護理論発展の背景 2)日本の看護史 3)ナイチンゲールの位置 4)〈延命〉の文脈で推奨される医療者の態度 第2節 看護における《ケアリング》の展開 1)ノディングスの《ケアリング》論 2)ワトソンの《ケアリング》論 第3節 ケアの《現象学》 1)ベナーの現象学的看護論 2)日本の《現象学》的ケア論 第4節 小括 |
|
| 第6章 クーゼにおける《ケアの倫理》批判 第1節 クーゼについて 第2節 クーゼは《ケアの倫理》をどのように批判したか 第3節 「健康」の曖昧さと功利主義的《ケアの倫理》 第4節 小括 |
|
| 第7章 〈延命〉の医療における看護の機能 第1節 看護師が行う「意思決定支援」 1)ADMへの看護師の関与―最近の研究から 2)「意思決定支援」への看護師の関与―日本の報告 第2節 「意思決定支援」の多角的分析 1)経済学からみた「意思決定支援」 2)モルの人類学からみた「意思決定支援」 3)中村の人類学からみた「意思決定支援」 第3節 〈延命〉のための看護 1)看護過程からの分析 2)「生理的欲求」の充足 第4節 小括 |
|
| 終章 〈延命〉の医療における看護の倫理 |
|
| 初出一覧 文献 |
|
| https://www.koyoshobo.co.jp/book/b642740.html |
|
★書評
■
医療と看護における延命の(倫理ではなくて)論理とはなんだろうということを評者に考えさせてくれた労作。日本でのアドバンス・ケア・プランニング
(ACP)という終末期の「処遇」の意思決定について、これまでのインフォームドコンセントを強化するという方法ではなく、全人的と称しながら一種の「社
会的アドバンスドディレクティブ」というエコシステムをつくろうという医師会や厚労省の流れのなかで、それに抗する主張はたのもしい。
■しかしながら、著者は延命の論理な生命倫理情報が満載されているわりには、著者がどのような倫理概念を構築するのかがいまひとつわかりにくい。
■また新しいACPの時代の医療と看護の延命の倫理とはなにかについても明言している発言を探すのは困難だ。
■はたして延命の倫理は生命操作技術のみならず人間観の変遷という社会環境のもとで変わるものなのか普遍的なものなのか?(あるいはそうあるべきなの
か?)。
■終章にとってつけたような「生理学的回帰を求める」という主張は、全体の流れを表象せずに唐突でり、ナンセンスな主張だ。フーコーのレイシズムの概念
も、本文冒頭と脚注に一度ほど登場し、終章でそれが人間のカテゴリカルな関係の倫理でどのように作動するかについての考察がないのは残念だ。
■私が博論の審査員なら、全文にわたり、著者が倫理という術語で何を訴えたいのかブラシュアップしなさいと指示を与えているところだろう。だから評者は本 書の読解中、患者に対峙する医療や看護の論理(それが倫理なのかもしれないが)とはなんだろうと考えてさせてくれた。多くの読者に問題を投げかける著作と してはすばらしいと思う。
★ACP の定義
「人生会議(アドバンス・ケア・プランニング)とは
もしものときのために、自らが望む医療やケアについて前もって考え、家族等や医療・ケアチームと繰り返し話し合い、共有する取り組みのことです。」令和6年度「人生会議」厚生労働省
☆余滴
看護師は(1)医療行為の圏外にある健康への回復という倫理的目的のために行動し(2)利他としてのケアに自己決定を尊重を主張するヘルガー・クーゼ(1997)のテーゼはケアが自己決定を優先すれば安楽死は正当化されると主張するがその筋は通っている
リ ンク
文 献
そ の他の情報
Copyleft, CC, Mitzub'ixi Quq Chi'j, 1996-2099
![]()
☆
 ☆
☆