Read this first
My Testament to Students Studying Critical Medical Anthropology
Mitzub'ixi Qu'q Ch'ij

Pictures
present from left to right; Rudolf Virchow, George Hunt, WHR Rivers,
and Michel Foucaut.
My Testament to Students Studying Critical Medical Anthropology
Mitzubixi IKEDA
Osaka University, Toyonaka JAPAN
(My_Testament240629_mikeda.pdf)
Dear friends,
■At the time to say good-bye for my students in medical anthropology, I
will confess sincerely my testament mentioned bellow. This document can
be divided two parts; the former mentions my own experience in rural
Honduras in mid-1980s, and the latter mentions my respectable heroes
when I was graduate student of public health and social medicine.
■In the mid-1980s, I joined in the Japan Overseas Cooperation
Volunteers, JOCVs, in Honduras, Central America. My work was an
assistance for public health education in rural areas in western
mountainous part of Honduras. I have researched how people think and
act about “health” through specific practices. The local people who
received our public health program understand “health” simply as the
absence from disease. They do not give the word “salud” (in Spanish,
that means “health”) the positive meaning that westerner can mention
sometime as "positive health". I think the concept of “health” of the
latter was newly introduced from outside the community. There existed
two concepts of “health,” one is traditional thought of conditions of
body that mention "there is no disease." The another was "positive
health" in modern westerner sense that we would try to introduce from
outside the community.
■Nonetheless, we have tried to introduce new “positive health” into
communities, the people did not accept and maintain old one. We
confront epistemological barrier of the local people. The one of
Honduran Ministry of Health officials used to say they were “ignorant.”
He said that because of local people's ignorance, our public health
program would be failed. He thought that the villagers were ignorant in
public health knowledge. However, this officer has completely forgotten
that his own concept of positive health also had been once educated.
■On the other hands, villagers, of course, did not consider themselves
ignorant. Nor are they aware that they are “resisting” against official
public health program. The village people expressed that the new public
health program was simply too difficult to understand. Consequently,
they were ironically labeled as “resisters” by the officials.
■Of course, the programs had attractive points for the villagers. If
they could attend a free seminar of our programs, they were offered
basic drugs, a notebook, a meal, or some snacks as reword by
registering their names. Also, there was an advantage such as to making
friends by attending the workshops. Once the project has been started,
villagers were benefited from being able to borrow free-loan money for
the installation of latrines. Small but new latrine can be strong
symbol of introducing new concept of positive health. Those who
accepted the project recognize themselves as “progressive,” while those
who did not accept it were as "being still ignorant." But the ones who
did not accept were criticized “progressive men” as those who had “sold
their souls” to the outsiders, such as government people. Then the
public health program had introduced the seed of discord into village.
The officers never express people who did not accept the program
“ignorance” in front of them. Unfortunately, this kind of insult
concepts also had been introduced into village through the public
health program. At the same time, in a village where various social
dynamics were functioning, informed consent does not always proceed
rationally.
■In so far, all villagers will not accept a new public health program.
Program supervisors were evaluating by yield rates and performance into
communities. Officers there participated explicit competition by
according their yield rates and performance among their own different
community's programs. For whom was the public health program? Naturally
for the common people, but also for the working officers who were
ordered by their project provide supervisors.
■Here, I would explain this case using the Foucauldian theory. For
instance, a person who had once studied these theories would interpret
it this way. Michel Foucault said that the power, especially political
power, does not only oppress the people but create them new subjects
that practice under social effects. In my case, to be a recipient of
public health program is to be a subject through acting on. However,
then the person who rejects the public health program coming into the
village must also “become another new subject.” These “resisters” who
oppose the program, and this is why the stereotypical adjectives,
“ignorant,” “conservative,” and “no progressive,” were attached by the
proponents of the program. When I participated in the health care
program in Honduras was in the world-wide Primary Health Care, the Alma
Ata Declaration in 1978. As above, I suppose that the Foucauldian
theory can be applied on the primary health care approach.
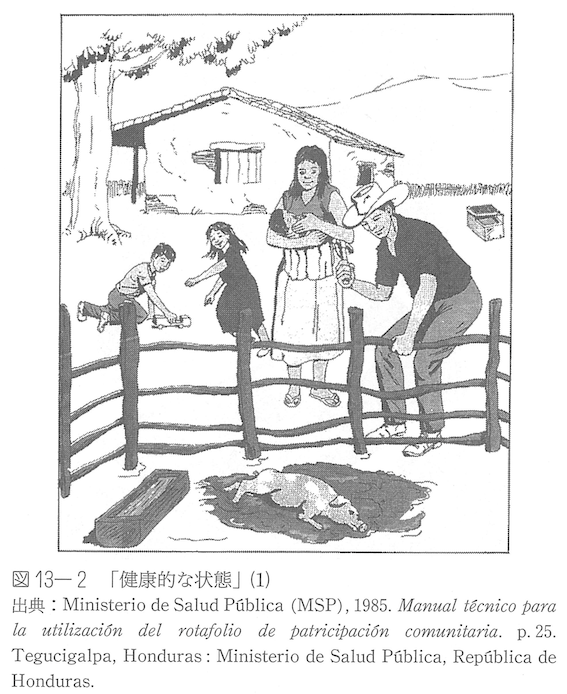
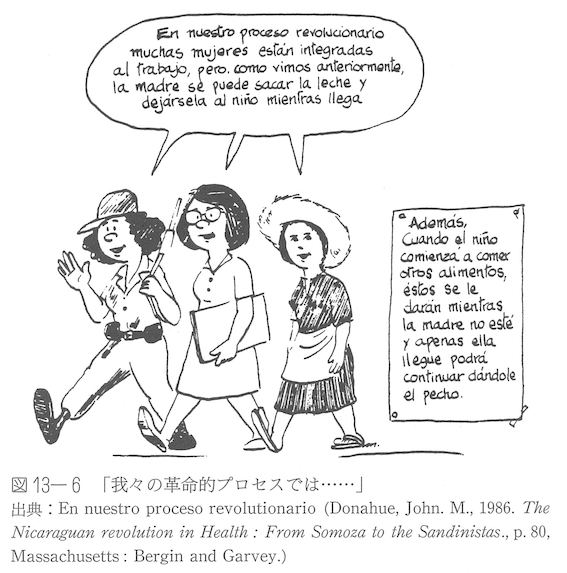
■Here there are two images of “good health” both Honduran in left and
of the Nicaraguan in right. These two images of good health were
different by depending on their governmental political ideology;
Honduras was an anti-communist country supported by former President
Ronald Regan of the United States, Nicaragua had Sandinista
Revolutionary Government which promoted the anti-capitalist good health
policy under the support by Cuba. The mid-1980s' figures demonstrate
the national differences between them.
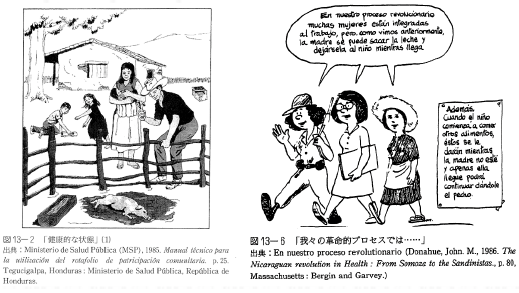
■Two figures
demonstrate the national difference of "good health or healthy lives"
between Honduras and Nicaragua in the mid-1980s.
■Then, even if “community-based” and “community’s participation” based
on informed consent are central, the self-determination of “resistance”
to the introduction of external programs might also be respected. I was
not very aware of this during my stay in Honduras. After leaving the
country, I learned about the Rural Appraisal by Dr. Robert Chambers,
the principle of the action research by Sol Tax, which has a long
history in anthropology, and the subsequent Community-Based
Participatory Research (CBPR), in which the option of “rejection” from
the peoples' point of view, rather than “resistance” from the side of
power holder, I found that it should be respect for accepting the
option of “refusal” as equal as for “accordance and/ or acceptance.”
Just as I have learned the peoples' autonomous spirits in public health
programs.
■When medical anthropologists have the “will” to change the
conservative or traditional things in a village, this is always
considered problematic as it violates the dogma or doctrine of
“cultural relativism” that anthropology has long accepted as discipline
to its work. On the other hand, in applied anthropology, it is
commonplace to identify malfunctions within a community and, through
discussions with the residents, to confirm the “will” of the community
to promote projects. Today, when the former term “applied anthropology”
has faded and become public anthropology and/ or engaged anthropology,
egalitarian dialogue within the community's autonomy is very important.
The cold-hearted word of “cultural relativism” has now receded in
medical anthropology, and the emphasis is now on “cultural
egalitarianism,” “dialogue under equal conditions,” and
“community-based autonomy.”
■Over there, in the 1980s, a project of communities’ total conversion
for modern public health based on paternalism, is not different from
the “medical missionary work/medical mission” of the colonial era. When
I was writing the paper about the story mentioned above, later entitled
“Health Promotion and Health Ideology,” I guess I had not yet arrived
at this perception of medical anthropology as “medical missionary
work.” There, I was probably stuck in the doxa that it is the residents
who change their ideas and actions through health and medical treatment
projects, not the medical anthropologists themselves who change their
own ideas and attitudes.
■
Pictures present from left to right; Rudolf Ludwig Carl Virchow
(1821-1902), George Hunt (1854-1933), W.H.R. Rivers (1864-1922), and
Michel Foucault (1926-1984)
■I began studying medical anthropology in 1981, and there were four
heroes for me at that time. In order of their birth dates, they are
Rudolf Ludwig Carl Virchow (1821-1902), George Hunt (1854-1933),
William Halse Rivers Rivers (1864-1922), and Paul-Michel Foucault
(1926-1984). Foucault was born in the same year as my mentor, Yonezo
Nakagawa (1926-1997). Virchow and Rivers are well known as the founders
of medical anthropology in the Anglo-American world. Each of them is a
unique and brilliant individual who has influenced my books and
articles in various ways.
■Yonezo Nakagawa (1926-1997)
■Virchow brought us a practical challenge at the roots of medical
anthropology with his dictum, “medicine is a social science to the
bone.” W.H.R. Rivers was the psychiatrist who, along with Sigmund
Freud, described war neuroses or shell shock (a kind of combat
fatigue), considered to be a related syndrome of Post Traumatic Stress
Disorder, PTSD. He also established the genealogical method, a
significant advance in kinship research. On the other hand, he
participated in the Cambridge University Torres Strait Expedition,
organized by Alfred Cort Haddon, and argued that, apart from their
capacity for acuity, the “savages” had no physiological differences in
their repertoire of sensibilities, and that language and metaphor
provided diversity in illness expression and classification. In
particular, he suggested that the classification of sickness was as
systematic in “uncivilized societies” as to be comparable to the
Western taxonomy of diseases or nosology. Foucault not only developed
the concept of bio-power, but also considered the concept of governing,
the term, governmentality, how to govern people and society through
biomedicine and demography. Today, the concept of governmentality has
become an essential analytical tool for many researchers analyzing the
public health and medical ethics.
■Many of you may not know George Hunt. However, he is called as
"Quesalid," a sorcerer or shaman who appears pseudonymously in Franz
Boas' “Ethnography of the Kwakiutl,” today as the Kwakwaka'wakw. In the
chapter of “The Sorcerer and His Magic” in Lévi-Strauss' monumental
book, entitled as “Structural Anthropology,” published in 1963
translated from French to English. Among many anthropologists it is
known the name of Quesalid but never known his real name George Hunt. I
learned that Quesalid was George Hunt from James Clifford's book, “The
Predicament of Culture” (1988). Hunt's genealogical origins were both
Tlingit and British, not Kwakwaka'wakw, and he grew up in Kwakwaka'wakw
territory with his parents and through intermarriage and adoption
became himself a native anthropologist familiar with Kwakwaka'wakw
language and culture. Franz Boas became friends with Gorge Hunt to
exhibit the Kwakwaka'wakw at the World’s Columbian Exposition in
Chicago in 1893. Boas taught Hunt linguistic anthropology and phonetic
notation, especially Kwakwaka'wakw orthograph. Hunt is said to have
written more than 10,000 pages of ethnographic notes of Kwakwaka'wakw
including his autobiographical experience for Franz Boas.
■When I still read the chapter, “The Sorcerer and His Magic” by
Lévi-Strauss, through his storytelling, I am still impressed by the
auto-ethnography of George Hunt, that is the things about Quesalid. It
seems to me that native anthropologists can reach the inner recesses of
cultural understanding without going through the dogma of “cultural
relativism.” It also seems to me that the technique for reading across
cultures is not to immerse oneself in the culture of the others. The
technique for reading across cultures is always to be “conscious” of
the fact that one's own culture dissolves in the culture of the others
by forgetting what one has learned. In other words, as an
anthropologist himself, George Hunt could dissolve his role as a
sorcerer because he analyzed other healers in the culture in question
by practice of his cross-cultural reading as reflexive process. The
important thing is not that he took epistemological relativism but that
he did understand what is to be powerful healer among the Kwakwaka'wakw
through his devious and an-ethical performance among Indians.
■Japanese social medicine from the 1920s onward, as described in the
proceedings of this meeting, tried to live up to Virchow's dictum that
“medicine is a social science to the bone.” Medical doctors, like
applied medical anthropologists today, tried to practice their social
medicine by spending time in rural villages and urban squatters.
However, in Japan from the 1930s to 1945, they were grabbed by thought
control policy, recruited by military soldiers (and even some of them
defected to the Soviet Union and were purged by dictator Joseph
Stalin). And young idealist medical doctor survivors were disappointed
by Japan's defeat in the war. After Japan's defeat, the occupied
military had introduced United States' public health policy instead of
pre-war German Sozialmedizin.
■Now we confront with dilemma of whether to change our mind or reform
our society. We are requested to behave with reflective criticism. It
can fall into another pitfall of reproducing unreflective criticism,
criticism for criticism's sake, and falling into “mere condemnation.”
Criticism is an act like walking a tightrope. But it worths to try
again and again.
■My last words, my testament, are as follows: We must not only hope
that through criticism, the future of the subject will change in a
favorable and appropriate manner, but we must also have the courage to
change ourselves as critics.
■Yours Sincerely,
■Mitzub'ixi Qu'q Ch'ij
Your good friend.
tiocaima7n@gmail.com is valid until the end of my life....
■P.S.
I would be annoying you with citated from Samuel Beckett’s poem…I love it!!!
■First the body. No. First the place. No. First both. Now either. Now
the other. Sick of the either try the other. Sick of it back sick of
the either. So on. Somehow on. Till sick of both. Throw up and go.
Where neither. Till sick of there. Throw up and back. The body again.
Where none. The place again. Where none. Try again. Fail again. Better
again. Or better worse. Fail worse again. Still worse again. Till sick
for good. Throw up for good. Go for good. Where neither for good. Good
and all. – “Worstward Ho,” 1983
■I quart my fever phrases of the passage on Heraclitus’ “All things change” by Quincy Jones and Ray Brown,
■Everything must change
Nothing stays the same
Everyone will change
No one stays the same
The young become the old
And mysteries do unfold
‘Cause that’s the way of time
Nothing and no one goes unchanged
-- Everything must change
■your notes:
|
Two figures demonstrate the
national difference of "good health or healthy lives" between Honduras
and Nicaragua in the mid 1980s.
|
|
Two figures demonstrate the
national difference of "good health or healthy lives" between Honduras
and Nicaragua in mid 1980s. |
Link
Bibliography
other
information
Copyleft,
CC, Mitzub'ixi Quq Chi'j, 1996-2099
☆
 ☆
☆