「人種と健康」について考える
Rethinking Race and health
☆ このページは、ウィキペディア(英語版)にある、問題の多い記事である”Race and health” の翻訳と解釈を通して、その主張の正当性を疑問に付し、なにが問題であるのかを検討するサイトである。このサイトは、以下の一点のみ指摘されて、その記述 を気にせずに読むと、あたかも「人種と健康」にはなんらかの因果関係があるように感じられるような記述になっている。はたして、本当だろうか?
★ 問題があるとされた項目は「Racial health disparities(人種的健康の格差)」であり、その警告は次のようなものである:「この記事の例や見解は、このテーマに関する世界的な見解を表 しているわけではない。適宜、この記事を改善したり、トークページで議論したり、新しい記事を作成したりしてもよい。(2021年4月) (このメッセージを削除する方法とタイミングを学ぶ)」
☆こ のページの採用する人種概念の問題点は、「人種と健康」に関する以下の項目のなかの「論争」の部分で詳述されている。その箇所を全文引用すると以下のよう になる:
「論
争
こちらも参照のこと: 人種(人間の分類)、人種と遺伝学、対象化
人間を分類する方法としての人種については論争がある。異なる情報源は、人種は純粋に社会的構築物[93]であるとか、平均的な遺伝的集団の違いを反映し
た生物学的現実であると主張している。ヒトの生物学的変異に対する新たな関心が、生物医学における人種の使用の復活をもたらした[94]。
この発展の主なきっかけは、表現型や人種的自認のような、より容易に確認できる特徴に基づいて、遺伝的に条件付けられた保健要因のような、確認が困難な要
因を予測することによって、特定の疾病の予防や治療を改善できる可能性があることである。医学的判断はしばしば不確実な条件下での意思決定を伴うため
[95]、多くの医師は疾病を治療する際に人種を考慮に入れることが有用であると考えている。以前考えられていたよりも多くの疾病が人種識別と相関してい
ることが発見され、生物地理的な祖先や遺伝的蓄積の代理として人種を用いることへの関心がさらに高まっている[96]。
医学における人種は、より特異的な遺伝的・環境的危険因子の近似値として用いられている。このように、人種は、保健に影響を与えることが知られている社会
経済的地位の差異のような環境要因の代用品である。また、祖先の地理的地域や、異なる祖先集団間の遺伝子頻度の違い、したがって保健に影響しうる遺伝子の
違いに対する不完全な代用品でもある。この近似は完全ではないが、病気の確率や好ましい治療法の近似を与えることができる[15]。
鎌状赤血球症を例にとると、救急治療室において、患者がこの疾患に適合する症状を呈した場合、患者の地理的起源を知ることは、初期診断を行う医師の助けに
なるかもしれない。鎌状赤血球症は、前述のように多くの異なる集団に存在し、一部の地中海ヨーロッパの集団にもその形質が見られることから、これは信頼で
きない証拠である。確定診断は患者の血液を調べることによって行われる。米国では、鎌状赤血球貧血のスクリーニングは人種に関係なくすべての新生児に対し
て行われている[95]。
人種分類の継続的な使用は批判されている。人種に関する一般的な論争とは別に、保健医療や危険因子として人種カテゴリーを使用し続けることは、社会や保健
サービスにおけるステレオタイプや差別を増大させる可能性があると主張する者もいる[15][97][98]。生物学的概念としての人種に批判的な者の中
には、人種は社会的に意味のある集団であり、格差を減らすために疫学的に研究することが重要であると考える者もいる[99]。
例えば、危険因子が評価された後でも、骨粗鬆症の適切な治療を受ける可能性が他の集団よりも低い人種がいる。19世紀以来、黒人は白人よりも骨が太く、加
齢に伴う骨量の減少が遅いと考えられてきた [100]
。また、女性に比べて男性の方が、治療を受ける可能性が有意に低かった。この不一致は、平均してアフリカ系アメリカ人は白人よりも骨粗鬆症のリスクが低い
という医師の知識によるものかもしれない。このような医師が、リスクの高いアフリカ系アメリカ人にこのデータを一般化し、これらの人々の骨粗鬆症の適切な
評価と管理を怠ることにつながっている可能性がある。黒人アメリカ人はまた、アメリカ心臓協会(AHA)がすべてのリスクを下げようと試みた後でも、心血
管疾患に関する死亡率が最も高く、白人アメリカ人よりも約30%高い[101]。
David Williams (1994)は、1966年から90年の間に雑誌『Health Services
Research』に掲載された論文を調査した結果、人種がどのように決定され定義されたかはほとんど記述されていないと主張した。少なくとも研究者は、
人種が自己申告、代理報告、記録からの抽出、または直接観察によって評価されたかどうかを記述すべきである。人種はまた、社会経済的地位の指標として使用
されるなど、疑問視されることも多かった[102]。人種的遺伝的説明が過度に強調され、環境との相互作用や環境の役割が無視されている可能性がある
[103]。」
| Race
and health , "race and health" refers to how being identified with a specific race
influences health. Race is a complex concept that has changed across
chronological eras and depends on both self-identification and social
recognition.[1] In the study of race and health, scientists organize
people in racial categories depending on different factors such as:
phenotype, ancestry, social identity, genetic makeup and lived
experience. Race and ethnicity often remain undifferentiated in health
research.[2][3] Differences in health status, health outcomes, life expectancy, and many other indicators of health in different racial and ethnic groups are well documented.[4] Epidemiological data indicate that racial groups are unequally affected by diseases, in terms or morbidity and mortality.[5] Some individuals in certain racial groups receive less care, have less access to resources, and live shorter lives in general.[6] Overall, racial health disparities appear to be rooted in social disadvantages associated with race such as implicit stereotyping and average differences in socioeconomic status.[7][8][9] Health disparities are defined as "preventable differences in the burden of disease, injury, violence, or opportunities to achieve optimal health that are experienced by socially disadvantaged populations".[10] According to the U.S. Centers for Disease Control and Prevention, they are intrinsically related to the "historical and current unequal distribution of social, political, economic and environmental resources".[10] The relationship between race and health has been studied from multidisciplinary perspectives, with increasing focus on how racism influences health disparities, and how environmental and physiological factors respond to one another and to genetics.[7][8] Research highlights a need for more race-conscious approaches in addressing social determinants, as current social needs interventions show limited adaptation to racial and ethnic disparities.[11][12] |
人種と保健とは、特
定の人種であることが保健にどのような影響を与えるかを指す。人種は複雑な概念であり、時代によって変化し、自認と社会的認知の両方に依存している。
[1]
人種と保健の研究において、社会科学者は、表現型、祖先、社会的アイデンティティ、遺伝的構成、生活経験などの異なる要因によって、人々を人種カテゴリー
に整理する。保健研究では、人種と民族はしばしば未分化のままである[2][3]。 異なる人種・民族集団における保健状態、健康アウトカム、平均余命、その他多くの健康指標における相違は、十分に文書化されている[4]。疫学的データ は、罹患率や死亡率の点で、人種集団が疾患によって不平等に影響を受けることを示している。 [5] ある種の人種集団では、より少ない医療しか受けられず、資源へのアクセスも少なく、一般的に短命である。6] 全体として、人種間の健康格差は、暗黙のステレオタイプや社会経済的地位の平均的な差など、人種に関連した社会的不利に根ざしているようである。 健康格差は、「社会的に不利な立場にある集団が経験する、疾病、傷害、暴力、または最適な健康を達成する機会の負担における予防可能な差異」と定義されて いる[10]。 米国疾病管理予防センターによると、これらは「社会的、政治的、経済的、環境的資源の歴史的かつ現在の不平等な分配」と本質的に関連している[10]。 人種と健康の関係は学際的な観点から研究されており、人種主義が保健格差にどのように影響するか、環境的・生理学的因子が互いに、また遺伝学にどのように 反応するかにますます焦点が当てられている[7][8]。現在の社会的ニーズへの介入が人種・民族的格差への適応に限界があることから、社会的決定要因へ の取り組みにおいて、より人種を意識したアプローチの必要性が研究によって強調されている[11][12]。 |
| Racial health disparities The examples and perspective in this article may not represent a worldwide view of the subject. You may improve this article, discuss the issue on the talk page, or create a new article, as appropriate. (April 2021) (Learn how and when to remove this message) Health disparities refer to gaps in the quality of health and health care across racial and ethnic groups.[13] The US Health Resources and Services Administration defines health disparities as "population-specific differences in the presence of disease, health outcomes, or access to health care".[14] Health is measured through variables such as life expectancy and incidence of diseases.[15] For racial and ethnic minorities in the United States, health disparities take on many forms, including higher rates of chronic disease, premature death, and maternal mortality compared to the rates among whites. For example, African Americans are 2–3 times more likely to die as a result of pregnancy-related complications than white Americans.[16] It is important to note that this pattern is not universal. Some minority groups—most notably, Hispanic immigrants—may have better health outcomes than whites when they arrive in the United States. However this appears to diminish with time spent in the United States.[17] For other indicators, disparities have shrunk, not because of improvements among minorities but because of declines in the health of majority groups. In the U.S., more than 133 million Americans (45% of the population) have one or more chronic diseases. One study has shown that between the ages of 60 and 70, racial/ethnic minorities are 1.5 to 2.0 times more likely than whites (Hispanic and non Hispanic) to have one of the four major chronic diseases specifically Diabetes, cancer, cardiovascular disease (CVD), and chronic lung disease. However, the greatest differences only occurred among people with single chronic diseases. Racial/ethnic differences were less distinct for some conditions including multiple diseases. Non-Hispanic whites trended toward a high prevalence for dyads of cardiovascular disease (CVD) with cancer or lung disease. Hispanics and African Americans had the greatest prevalence of diabetes, while non-Hispanic blacks had higher odds of having heart disease with cancer or chronic lung disease than non-Hispanic whites. Among non-Hispanic whites the prevalence of multimorbidities that include diabetes was low; however, non-Hispanic whites had a very high prevalence of multimorbidities that exclude diabetes. Non-Hispanic whites had the highest prevalence of cancer only or lung disease only.[18] Black Americans have an increased risk of death from COVID-19 compared to white Americans. In a study in Michigan in 2020 regarding COVID-19, it is shown that Black people are 3.6 times more likely to die due to COVID-19.[19] In the United States, the mental health of African Americans has been shown to be negatively impacted by systemic racism, contributing to increased risk of mortality from substance use disorders. This negative mental health can lead to reaching for substances to cope with the mental effects of systemic racism.[20] Structural racism, as outlined by Bailey et al., is a key driver of these disparities. It encompasses interconnected systems such as housing, healthcare, education, employment, and criminal justice that perpetuate racial discrimination and the unequal distribution of resources. For instance, housing discrimination and limited access to quality healthcare facilities in predominantly Black neighborhoods create barriers to effective care. These inequities, coupled with racially biased medical practices, result in higher rates of chronic diseases, greater mortality, and poorer health outcomes among African Americans. Addressing these structural issues is crucial for improving health equity and reducing the systemic disadvantages faced by racial and ethnic minorities.[21] Macias-Konstantopoulos et al. (2023) highlight how these factors disproportionately affect Black, Indigenous, and People of Color (BIPOC), leading to significant health-care inequities. Emergency medicine (EM) serves as a critical domain for examining these disparities, particularly in the treatment of infectious diseases such as HIV and COVID-19, noncommunicable diseases like diabetes and hypertension, and trauma cases like gunshot injuries. Systemic imbalances, rather than genetic differences, create longer wait times for Black patients in emergency departments and less effective pain management compared to their white counterparts. Such inequalities highlight the pervasive impact of institutional biases in health care.[citation needed] The study also emphasizes actionable steps for addressing these inequities, including fostering culturally sensitive practices and enhancing access to quality care for minority communities. This underscores the need for health-care professionals to understand the interplay between race, systemic determinants of health, and outcomes to foster equitable health care for all populations.[22] Between 1960 and 2005 the percentage of children with a chronic disease in the United States quadrupled with minority having higher likelihood for these disease. The most common major chronic biases of youth in the United States are asthma, diabetes mellitus, obesity, hypertension, dental disease, attention deficit hyperactivity disorder (ADHD), mental illness, cancers and others. This results in Black and Latin adult patients facing a disproportionate amount of health concerns, such as asthma, with treatment and management guidelines not developed with studies based on their populations and healthcare needs.[1] Although individuals from different environmental, continental, socioeconomic, and racial groups etc. have different levels of health, yet not all of these differences are always categorized or defined as health disparities. Some researchers separate definitions of health inequality from health disparity by preventability. Health inequalities are often categorized as being unavoidable i.e. due to age, while preventable unfair health outcomes are categorized as health inequities. These are seen as preventable because they are usually associated with income, education, race, ethnicity, gender, and more.[23] |
人種的健康の格差 「この記事の例や見解は、このテーマに関する世界的な見解を表している わけではない。適宜、この記事を改善したり、トークページで議論したり、新しい記事を作成したりしてもよい。(2021年4月) (このメッセージを削除する方法とタイミングを学ぶ)」 健康格差とは、人種や民族間の健康や医療の質における格差のことである[13]。米国保健資源サービス庁は、健康格差を「疾病の有無、健康アウトカム、医 療へのアクセスにおける集団特有の差異」と定義している[14]。 米国における人種的・民族的マイノリティの保健格差は、白人と比較して慢性疾患、早死、妊産婦死亡率が高いなど、様々な形で現れている。例えば、アフリカ 系アメリカ人は白人アメリカ人に比べて、妊娠関連の合併症の結果死亡する確率が2~3倍高い[16]。このパターンが普遍的ではないことに注意することが 重要である。一部のマイノリティ集団、とりわけヒスパニック系移民は、米国に到着した当初は白人よりも保健上の転帰が良好であったかもしれない。しかし、 これは米国に滞在する時間が長くなるにつれて減少するようである[17]。他の指標では、格差が縮小しているが、これはマイノリティの改善ではなく、マ ジョリティ集団の保健の低下によるものである。 米国では、1億3,300万人以上の米国人(人口の45%)が、1つ以上の慢性疾患を抱えている。ある研究によると、60歳から70歳の間に、人種的/民 族的マイノリティは、白人(ヒスパニック系、非ヒスパニック系)の1.5倍から2.0倍、4大慢性疾患、具体的には糖尿病、がん、心血管疾患(CVD)、 慢性肺疾患のいずれかに罹患する可能性が高い。しかし、最も大きな相違は、単一の慢性疾患を持つ人々の間でのみ生じた。複数の疾病を含むいくつかの疾患で は、人種・民族の差異はそれほど明確ではなかった。非ヒスパニック系白人は、心血管系疾患(CVD)と癌または肺疾患の二重有病率が高い傾向にあった。ヒ スパニック系とアフリカ系アメリカ人は糖尿病の有病率が最も高く、非ヒスパニック系黒人は非ヒスパニック系白人よりも癌や慢性肺疾患を伴う心臓病のオッズ が高かった。非ヒスパニック系白人では、糖尿病を含む多疾病の有病率は低かったが、非ヒスパニック系白人では糖尿病を除く多疾病の有病率が非常に高かっ た。非ヒスパニック系白人は癌のみ、または肺疾患のみの有病率が最も高かった[18] 。黒人アメリカ人は白人アメリカ人と比較してCOVID-19による死亡リスクが高い。2020年にミシガン州で行われたCOVID-19に関する調査で は、黒人はCOVID-19が原因で死亡する可能性が3.6倍高いことが示されている[19]。 米国では、アフリカ系アメリカ人の精神保健が体系的人種主義によって悪影響を受け、物質使用障害による死亡リスクの上昇に寄与していることが示されてい る。このような否定的な精神保健は、制度的人種差別の精神的影響に対処するために物質に手を伸ばすことにつながる[20]。これは、人種差別と資源の不平 等な分配を永続させる、住宅、医療、教育、雇用、刑事司法などの相互に関連したシステムを包含している。例えば、黒人が多く住む地域では、住宅差別や質の 高い医療施設へのアクセスが制限されており、効果的なケアを受けるための障壁となっている。こうした不公平は、人種的に偏った医療行為と相まって、アフリ カ系アメリカ人の慢性疾患罹患率の高さ、死亡率の高さ、保健上の転帰の悪さをもたらしている。これらの構造的問題に対処することは、保健の公平性を改善 し、人種的・民族的マイノリティが直面する制度的不利益を軽減するために極めて重要である [21] 。 Macias-Konstantopoulosら(2023年)は、これらの要因がいかに黒人、先住民、有色人種(BIPOC)に不釣り合いな影響を及ぼ し、保健医療の著しい不平等につながっているかを強調している。救急医療(EM)は、特にHIVやCOVID-19のような感染症、糖尿病や高血圧のよう な非感染性疾患、銃創のような外傷の治療において、このような格差を検討するための重要な領域となっている。遺伝的な差異よりもむしろ、全身的な不均衡 が、白人患者と比較して、黒人患者の救急外来での待ち時間の長さや、疼痛管理の効果の低さを生み出している。このような不平等は、保健医療における制度的 偏見が広く影響していることを浮き彫りにしている[要出典]。 この研究ではまた、これらの不公平に対処するための実行可能なステップを強調しており、これには文化的に配慮した診療の育成や、マイノリティコミュニティ のための質の高いケアへのアクセスの強化などが含まれる。このことは、保健医療の専門家が、すべての集団に対して公平な保健医療を育むために、人種、健康 の全身的決定因子、転帰の相互作用を理解する必要性を強調している[22]。 1960年から2005年の間に、米国では慢性疾患を持つ子どもの割合が4倍に増加しており、マイノリティはこれらの疾患の可能性が高い。米国で青少年に 多い主な慢性疾患は、喘息、糖尿病、肥満、高血圧、歯科疾患、注意欠陥多動性障害(ADHD)、精神疾患、がんなどである。その結果、黒人やラテン系の成 人患者は、喘息などの保健上の懸念に不釣り合いに直面することになり、治療や管理のガイドラインは、彼らの集団や医療ニーズに基づいた研究によって作成さ れていない[1]。 環境的、大陸的、社会経済的、人種的に異なる集団に属する個人は、それぞれ異なる保健レベルを有しているが、これらの差異のすべてが常に健康格差として分 類・定義されるわけではない。研究者の中には、保健の不平等と予防可能性による保健格差の定義を分けて考える人もいる。健康格差は、年齢によるものなど、 避けられないものとして分類されることが多いが、予防可能な不公平な保健結果は健康不平等と分類される。これらは通常、所得、教育、人種、民族、性別など に関連するため、予防可能であるとみなされる[23]。 |
| Defining race Main article: Race (human categorization) Definitions of race are ambiguous due to the various paradigms used to discuss race. These definitions are a direct result of biological and social views. Definitions have changed throughout history to yield a modern understanding of race that is complex and fluid. Moreover, there is no one definition that stands, as there are many competing and interlocking ways to look at race.[24] Due to its ambiguity, terms such as race, genetic population, ethnicity, geographic population, and ancestry are used interchangeably in everyday discourse involving race. Some researchers critique this interchangeability noting that the conceptual differences between race and ethnicity are not widely agreed upon.[25] Even though there is a broad scientific agreement that essentialist and typological conceptions of race are untenable,[26][27][28][29][30][31] scientists around the world continue to conceptualize race in widely differing ways.[32] Historically, biological definitions of race have encompassed both essentialist and anti-essentialist views. Essentialists have sought to show that racial groups are genetically distinct populations, describing "races as groups of people who share certain innate, inherited biological traits".[33] In contrast, anti-essentialists have used biological evidence to demonstrate that "race groupings do not reflect patterns of human biological variation, countering essentialist claims to the contrary".[34] Over the past 20 years, a consensus has emerged that, while race is partially based on physical similarities within groups, it does not have an inherent physical or biological meaning.[35][36][37] In response, researchers and social scientists have begun examining notions of race as constructed.[38] Racial groups are "constructed" from differing historical, political, and economic contexts, rather than corresponding to inherited, biological variations. Proponents of the constructionist view claim that biological definitions have been used to justify racism in the past and still have the potential to be used to encourage racist thinking in the future.[33] Since race is changing and often so loosely characterized on arbitrary phenotypes, and because it has no genetic basis, the only working definition we can assign it is a social construct. This is not to say race is imaginary or non-existent. It is an important social reality. However to say that the concept of race has any scientific merit or has a scientific foundation can lead to many issues in scientific research, and it may also lead to inherent racial bias.[39] Social interpretations of race explains that social views also better explain the ambiguity of racial definitions. An individual may self-identify as one race based on one set of determinants (for example, phenotype, culture, ancestry) while society may ascribe the person otherwise based on external forces and discrete racial standards. Dominant racial conceptions influence how individuals label both themselves and others within society.[citation needed] Modern human populations are becoming more difficult to define within traditional racial boundaries due to racial admixture. Most scientific studies, applications, and government documents ask individuals to self-identify race from a limited assortment of common racial categories.[40] The conflict between self-identification and societal ascription further complicates biomedical research and public health policies. However complex its sociological roots, race has real biological ramifications; the intersection of race, science, and society permeates everyday life and influences human health via genetics, access to medical care, diagnosis, and treatment. |
人種の定義 主な記事 人種(人間の分類)[→形質人類学における 人種理論] 人種の定義は、人種を論じるために使われる様々なパラダイムのために曖昧である。これらの定義は、生物学的および社会的見解の直接的な結果である。歴史を 通じて定義が変化してきた結果、複雑で流動的な現代の人種理解が生まれたのである。その曖昧さゆえに、人種、遺伝的集団、エスニシティ、地理的集団、祖先 などの用語は、人種に関わる日常的な言説において互換的に使用されている。一部の研究者は、人種とエスニシティ間の概念的な差異が広く合意されていないこ とを指摘し、この互換性を批判している[25]。 人種に関する本質論的、類型論的概念は成り立たないという広範な科学的合意があるにもかかわらず、[26][27][28][29][30][31]世界 中の科学者は広く異なる方法で人種を概念化し続けている。本質主義者は、人種集団が遺伝的に異なる集団であることを示そうとし、「人種とは、特定の生得 的、遺伝的な生物学的形質を共有する人々の集団である」と説明してきた[33]。対照的に、反本質主義者は生物学的証拠を用いて、「人種集団は人間の生物 学的変異のパターンを反映しておらず、本質主義者の主張に反している」ことを実証してきた[34]。 過去20年にわたり、人種は集団内の物理的類似性に部分的に基づくものの、固有の物理的・生物学的意味を持たないというコンセンサスが形成されてきた [35][36][37]。 これに対し、研究者や社会科学者は、構築されたものとしての人種の概念を検討し始めている[38]。人種集団は、遺伝的・生物学的変異に対応するのではな く、異なる歴史的・政治的・経済的文脈から「構築」されたものである。構築主義的見解の支持者は、生物学的定義は過去において人種主義を正当化するために 使用されてきたし、将来においても人種主義的思考を助長するために使用される可能性があると主張している。これは、人種が想像上のものであるとか、存在し ないということではない。それは重要な社会的現実である。しかし、人種という概念に科学的な利点があるとか、科学的な基盤があると言うことは、科学的研究 において多くの問題を引き起こす可能性があり、また人種的偏見を内在させる可能性もある[39]。 人種に関する社会的解釈は、社会的見解もまた人種定義の曖昧さをよりよく説明すると説明している。ある個人がある決定要因(例えば、表現型、文化、祖先) に基づいてある人種であると自認する一方で、社会は外的な力や個別の人種基準に基づいてその人格をそうでないとすることがある。支配的な人種概念は、個人 が社会内で自分自身と他者にどのようなレッテルを貼るかに影響を及ぼす[要出典]。現代人の集団は、人種的混血のために伝統的な人種の境界で定義すること が難しくなっている。ほとんどの科学的研究、申請書、政府文書は、一般的な人種分類の限られた品揃えから人種を自認するよう個人に求めている[40]。自 認と社会的帰属の間の対立は、生物医学研究と保健政策をさらに複雑にしている。人種、科学、社会の交差点は日常生活に浸透しており、遺伝学、医療へのアク セス、診断、治療を通じて人の保健に影響を及ぼしている。 |
| Race and disease Diseases affect racial groups differently, especially when they are co-related with class disparities.[4] As socioeconomic factors influence the access to care,[citation needed] the barriers to access healthcare systems can perpetuate different biological effects of diseases among racial groups that are not pre-determined by biology. Some researchers advocate for the use of self-reported race as a way to trace socioeconomic disparities and its effects in health.[41] For instance, a study conducted by the National Health Service checks program in the United Kingdom, which aims to increase diagnosis across demographics, noted that "the reported lower screening in specific black and minority ethnic communities... may increase inequalities in health."[42] In this specific case, the lack of attention to certain demographics can be seen as a cause of increased instances of disease from this lack of proper, equal preventive care. One must consider these external factors when evaluating statistics on the prevalence of disease in populations, even though genetic components can play a role in predispositions to contracting some illnesses. Individuals who share a similar genetic makeup can also share certain propensity or resistance to specific diseases. However, there are confronted positions in relation to the utility of using 'races' to talk about populations sharing a similar genetic makeup. Some geneticists argued that human variation is geographically structured and that genetic differences correlate with general conceptualizations of racial groups.[43] Others claimed that this correlation is too unstable and that the genetic differences are minimal and they are "distributed over the world in a discordant manner".[44] Therefore, race is regarded by some as a useful tool for the assessment of genetic epidemiological risk,[45] while others consider it can lead to an increased underdiagnosis in 'low risk' populations.[46] |
人種と疾病 社会経済的要因は医療へのアクセスに影響するため[要出典]、医療制度を利用するための障壁は、生物学によってあらかじめ決定されるわけではない、人種間 で異なる疾病の生物学的影響を永続させる可能性がある。 研究者の中には、社会経済的格差と保健におけるその影響を追跡する方法として、自己申告の人種を利用することを提唱する者もいる[41]。 例えば、国民保健サービス(National Health Service)チェックプログラム(National Health Service checks program in the United Kingdom)によって実施された研究では、「特定の黒人および少数民族コミュニティにおける検診の低さが報告されており、...保健における不平等を 増大させる可能性がある」と指摘している[42]。集団における疾病の有病率に関する統計を評価する際には、このような外的要因を考慮しなければならな い。 同じような遺伝的構成を持つ人々は、特定の病気に対する傾向や抵抗力を共有することもある。しかし、同じような遺伝的構成を共有する集団について語るのに 「人種」を用いることの有用性に関連して、対立する立場がある。一部の遺伝学者は、ヒトの変異は地理的に構造化されており、遺伝的差異は人種集団の一般的 概念と相関していると主張した[43]。また、この相関はあまりにも不安定であり、遺伝的差異はわずかであり、それらは「不和な形で世界中に分布してい る」と主張する者もいた[44]。 |
| Single-gene disorders See also: Genetic disorder There are many autosomal recessive single gene genetic disorders that differ in frequency between different populations due to the region and ancestry as well as the founder effect. Some examples of these disorders include: Cystic fibrosis, the most common life-limiting autosomal recessive disease among people of Northern European heritage Sickle-cell anemia, most prevalent in populations with sub-Saharan African ancestry but also common among Latin-American, Middle Eastern populations, as well as those people of South European regions such as Turkey, Greece, and Italy[47] Thalassemia, most prevalent in populations having Mediterranean ancestry, to the point that the disease's name is derived from Greek thalassa, "sea" Tay–Sachs disease, an autosomal recessive disorder most common among Ashkenazi Jews, French Canadians of Saguenay–Lac-Saint-Jean, Cajuns of Louisiana and Old Order Amish of Pennsylvania[48][49] Hereditary hemochromatosis, most common among persons having Northern European ancestry, in particular those people of Celtic descent Hermansky–Pudlak syndrome, most common among Puerto Ricans Finnish heritage diseases, autosomal recessive diseases that are far more common among Finns |
単一遺伝子疾患 こちらも参照のこと: 遺伝子疾患 常染色体劣性単遺伝子遺伝性疾患には、地域や祖先、創始者効果によって異なる集団間で頻度が異なるものが数多くある。これらの疾患の例をいくつか挙げる: 嚢胞性線維症は、北ヨーロッパの血を引く人々に最も多くみられる、生命を脅かす常染色体劣性遺伝性疾患である。 鎌状赤血球貧血:サハラ以南のアフリカに先祖を持つ集団に最も多くみられるが、ラテンアメリカ、中東、およびトルコ、ギリシャ、イタリアなどの南ヨーロッ パ地域の人々にもよくみられる[47]。 サラセミアは、地中海沿岸の祖先を持つ集団に最も多くみられ、その病名はギリシャ語のthalassa(海)に由来する。 テイ・サックス病は、アシュケナージ・ユダヤ人、サグネー=ラック=サン=ジャンのフランス系カナダ人、ルイジアナ州のケイジャン人、ペンシルベニア州の オールド・オーダー・アーミッシュに多くみられる常染色体劣性遺伝性疾患である[48][49]。 遺伝性ヘモクロマトーシス、北ヨーロッパの先祖を持つ人格、特にケルト系に多い。 Hermansky-Pudlak症候群、プエルトリコ人に多い。 フィンランド遺伝性疾患:常染色体劣性遺伝の疾患で、フィンランド人に多い。 |
| Multifactorial polygenic diseases Many diseases differ in frequency between different populations. However, complex diseases are affected by multiple factors, including genetic and environmental. There is controversy over the extent to which some of these conditions are influenced by genes, and ongoing research aims to identify which genetic loci, if any, are linked to these diseases. "Risk is the probability that an event will occur. In epidemiology, it is most often used to express the probability that a particular outcome will occur following a particular exposure."[50][51] Different populations are considered "high-risk" or "low-risk" groups for various diseases due to the probability of that particular population being more exposed to certain risk factors. Beyond genetic factors, history and culture, as well as current environmental and social conditions, influence a certain population's risk for specific diseases. |
多因子性多遺伝子疾患 多くの疾患は異なる集団間で頻度が異なる。しかし、複雑な疾患は遺伝的、環境的要因を含む複数の要因に影響される。これらの疾患のいくつかがどの程度遺伝 子の影響を受けているかについては議論があり、現在進行中の研究は、もしあるとすれば、どの遺伝子座がこれらの疾患と関連しているかを明らかにすることを 目的としている。「リスクとは、ある事象が起こる確率である。疫学では、特定の曝露の後に特定の結果が生じる確率を表すために最も頻繁に使用される" [50][51]。異なる集団は、特定の集団が特定の危険因子に曝露される確率が高いため、様々な疾患に対して「高リスク」または「低リスク」集団とみな される。遺伝的要因だけでなく、歴史や文化、現在の環境や社会的条件も、特定の集団の特定の疾患に対するリスクに影響を及ぼす。 |
| Disease progression Racial groups may differ in how a disease progresses. Different access to healthcare services, different living and working conditions influence how a disease progresses within racial groups.[52] However, the reasons for these differences are multiple, and should not be understood a consequence of genetic differences between races, but rather as effects of social and environmental factors affecting.[52] |
病気の進行 人種集団は疾患の進行の仕方において異なる場合がある。医療サービスへのアクセスの違い、生活・労働条件の違いは、人種集団内での疾患の進行に影響する。 しかしながら、このような違いの理由は複数あり、人種間の遺伝的な違いの結果として理解されるべきではなく、むしろ社会的・環境的要因の影響として理解さ れるべきである[52]。 |
| Prevention Genetics has been proven to be a strong predictor for common diseases such as cancer, cardiovascular disease (CVD), diabetes, autoimmune disorders, and psychiatric illnesses.[53] Some geneticists have determined that "human genetic variation is geographically structured" and that different geographic regions correlate with different races.[54] Meanwhile, others have claimed that the human genome is characterized by clinal changes across the globe, in relation with the "Out of Africa" theory and how migration to new environments cause changes in populations' genetics over time. Some diseases are more prevalent in some populations identified as races due to their common ancestry. Thus, people of African and Mediterranean descent are found to be more susceptible to sickle-cell disease while cystic fibrosis and hemochromatosis are more common among European populations.[54] Some physicians claim that race can be used as a proxy for the risk that the patient may be exposed to in relation to these diseases. However, racial self-identification only provides fragmentary information about the person's ancestry. Thus, racial profiling in medical services would also lead to the risk of underdiagnosis. While genetics plays a role in determining how susceptible a person is to specific diseases, environmental, structural, cultural, and communication messaging factors play a large role as well.[55][56] For this reason, it is impossible to discern exactly what causes a person to acquire a disease, but it is important to observe how many inter-related factors relate to each other. Each person's health is unique, as they have different genetic compositions and life histories. |
予防 遺伝学は、がん、心血管疾患(CVD)、糖尿病、自己免疫疾患、精神疾患などの一般的な疾患の強力な予測因子であることが証明されている[53]。一部の 遺伝学者は、「ヒトの遺伝的変異は地理的に構造化されている」と断定しており、異なる地理的地域は異なる人種と相関している[54]。 ある種の病気は、祖先が共通であるために、人種として特定される集団でより流行する。そのため、アフリカ系や地中海系の人々は鎌状赤血球症にかかりやす く、一方、嚢胞性線維症やヘモクロマトーシスはヨーロッパ系の人々に多いことが分かっている。しかし、人種の自認は人格の祖先に関する断片的な情報しか提 供しない。したがって、医療サービスにおける人種プロファイリングは、過小診断のリスクにもつながる。 人が特定の病気にかかりやすいかどうかを決定する上で、遺伝学が役割を果たす一方で、環境的、構造的、文化的、コミュニケーションメッセージ的な要因も大 きな役割を果たしている[55][56]。このため、人が病気にかかる原因を正確に特定することは不可能であるが、相互に関連する多くの要因がどのように 関連しているかを観察することは重要である。遺伝子構成や生活史が異なるため、人格の保健はそれぞれ異なる。 |
| Race-based treatment See also: Pharmacogenomics Racial groups, especially when defined as minorities or ethnic groups, often face structural and cultural barriers to access healthcare services. The development of culturally and structurally competent services and research that meet the specific health care needs of racial groups is still in its infancy.[57] In the United States, the Office of Minority Health The NIH (National institutes of health) and The WHO are organizations that provide useful links and support research that is targeted at the development of initiatives around minority communities and the health disparities they face. Similarly, In the United Kingdom, the National Health Service established a specialist collection on Ethnicity & Health.[58] This resource was supported by the National Institute for Health and Clinical Excellence (NICE) as part of the UK NHS Evidence initiative NHS Evidence.[citation needed] Similarly, there are growing numbers of resource and research centers which are seeking to provide this service for other national settings, such as Multicultural Mental Health Australia.[59] However, cultural competence has also been criticized for having the potential to create stereotypes. Scientific studies have shown the lack of efficacy of adapting pharmaceutical treatment to racial categories. "Race-based medicine" is the term for medicines that are targeted at specific racial clusters which are shown to have a propensity for a certain disorder. The first example of this in the U.S. was when BiDil, a medication for congestive heart failure, was licensed specifically for use in American patients that self-identify as black.[60] Previous studies had shown that African American patients with congestive heart failure generally respond less effectively to traditional treatments than white patients with similar conditions.[61] After two trials, BiDil was licensed exclusively for use in African American patients. Critics have argued that this particular licensing was unwarranted, since the trials did not in fact show that the drug was more effective in African Americans than in other groups, but merely that it was more effective in African Americans than other similar drugs. It was also only tested in African American males, but not in any other racial groups or among women. This peculiar trial and licensing procedure has prompted suggestions that the licensing was in fact used as a race-based advertising scheme.[62] Critics are concerned that the trend of research on race-specific pharmaceutical treatments will result in inequitable access to pharmaceutical innovation and smaller minority groups may be ignored. This has led to a call for regulatory approaches to be put in place to ensure scientific validity of racial disparity in pharmacological treatment.[63] Similarly, sexual orientation-based discrimination in healthcare has been shown to negatively impact health behaviors and outcomes, as demonstrated in a scoping review by Gioia and Rosenberger. The study highlights significant gaps in current data and illustrates how discrimination affects healthcare utilization behaviors, such as delaying care for cervical cancer screenings and contributing to poor health behaviors like substance abuse. The authors also emphasize the indirect effects of prejudice on health through medical distrust and poor patient-provider interactions. Recommendations include implementing LGBTQ-focused sensitivity training for healthcare personnel, addressing healthcare inequality through policy changes, and reducing medical mistrust to ensure equitable access to care for sexual minorities. These findings underscore that healthcare biases extend beyond race, encompassing sexual orientation and gender as significant factors influencing treatment outcomes.[64] An alternative to "race-based medicine" is personalized or precision medicine.[65] Precision medicine is a medical model that proposes the customization of healthcare, with medical decisions, treatments, practices, or products being tailored to the individual patient. It involves identifying genetic, genomic (i.e., genomic sequencing), and clinical information—as opposed to using race as a proxy for these data—to better predict a patient's predisposition to certain diseases.[66] In addition to issues surrounding race-based medications, discrimination in healthcare settings also plays a significant role in health outcomes. For example, a study by Turan et al. (2017)[67] demonstrated that perceived discrimination in healthcare settings negatively affected adherence to antiretroviral therapy (ART) among HIV-positive individuals. This was mediated by stigma and depressive symptoms, emphasizing the need for culturally competent care and efforts to address racism in healthcare to improve outcomes. This finding highlights the complex interplay between systemic racism, psychological factors, and treatment adherence in healthcare. |
人種に基づく処遇 こちらも参照のこと: ファーマコゲノミクス 人種集団は、特にマイノリティやエスニック集団と定義される場合、ヘルスケアサービスへのアクセスにおいて構造的・文化的障壁に直面することが多い。米国 では、NIH(国立衛生研究所)のOffice of Minority HealthとWHOが、マイノリティコミュニティと彼らが直面する保健格差をめぐるイニシアチブの開発に的を絞った有益なリンクを提供し、研究を支援し ている組織である[57]。同様に、英国では、国民保健サービス(National Health Service)が民族性と保健に関する専門家集団を設立した[58]。このリソースは、英国NHSエビデンス・イニシアチブNHS Evidenceの一環として、国立医療技術評価機構(National Institute for Health and Clinical Excellence:NICE)の支援を受けている[要出典]。同様に、多文化メンタルヘルス・オーストラリア(Multicultural Mental Health Australia)のように、このサービスを他の国家環境にも提供しようとするリソースや研究センターが増えている[59]。 科学的研究では、薬物治療を人種カテゴリーに適応させることの有効性の欠如が示されている。「人種に基づく医療」とは、ある疾患の傾向があるとされる特定 の人種集団を対象とした医薬品のことを指す。米国における最初の例は、うっ血性心不全の治療薬であるBiDilが、黒人と自認する米国人患者向けに特別に 認可されたことであった[60]。これまでの研究で、アフリカ系米国人のうっ血性心不全患者は、一般に、同様の疾患を持つ白人患者よりも従来の治療に対す る効果が低いことが示されていた[61]。 2回の臨床試験の後、BiDilはアフリカ系アメリカ人患者への使用に限定して認可された。批評家は、この個別主義的な認可は不当であると主張してきた。 というのも、試験では実際にこの薬が他のグループよりもアフリカ系アメリカ人に有効であることが示されたのではなく、単にアフリカ系アメリカ人に他の類似 薬よりも有効であることが示されたに過ぎなかったからである。また、この薬はアフリカ系アメリカ人の男性でのみテストされ、他の人種グループや女性ではテ ストされなかった。この特異な試験と認可の手順は、認可が実際に人種に基づく広告計画として使用されたという指摘を促した[62]。 批評家たちは、人種に特化した医薬品治療に関する研究の流れが、医薬品イノベーションへの不公平なアクセスをもたらし、より小さなマイノリティグループが 無視される可能性があることを懸念している。このため、薬理学的治療における人種間格差の科学的妥当性を確保するために、規制的アプローチを導入すること が求められている[63]。 同様に、医療における性的指向に基づく差別は、保健行動や転帰に悪影響を及ぼすことが、GioiaとRosenbergerによるスコープレビューで示さ れている。この研究では、現在のデータには大きなギャップがあることを強調し、差別が子宮頸がん検診の受診を遅らせたり、薬物乱用などの保健不良行動を助 長したりするなど、医療利用行動にどのような影響を及ぼすかを示している。著者らはまた、医療不信や患者と医療者の相互関係の悪化を通じて、偏見が保健に 及ぼす間接的な影響についても強調している。推奨事項としては、医療従事者に対するLGBTQに焦点を当てた感受性トレーニングの実施、政策変更による医 療格差への対応、性的マイノリティの医療への公平なアクセスを確保するための医療不信の軽減などが挙げられる。これらの知見は、医療の偏見が人種にとどま らず、性的指向や性別をも治療結果に影響を及ぼす重要な要因として包含していることを強調している[64]。 人種に基づく医療」に代わるものとして、個別化医療または精密医療がある[65]。精密医療とは、医療のカスタマイズを提案する医療モデルであり、医療上 の決定、治療、実践、または製品を個々の患者に合わせるものである。患者の特定の疾患に対する素因をよりよく予測するために、これらのデータの代理として 人種を用いるのとは対照的に、遺伝子、ゲノム(すなわち、ゲノム配列)、臨床情報を特定することが含まれる[66]。 人種に基づく薬物療法をめぐる問題に加えて、保健医療環境における差別もまた、保健アウトカムに重要な役割を果たしている。例えば、Turanら (2017)による研究[67]では、医療現場における差別の認知が、HIV陽性者の抗レトロウイルス療法(ART)のアドヒアランスに悪影響を及ぼすこ とが実証された。これはスティグマと抑うつ症状によって媒介されたものであり、転帰を改善するためには文化的に有能なケアと医療における人種主義に対処す る取り組みが必要であることが強調された。この知見は、制度的人種主義、心理的要因、医療における治療アドヒアランスの間の複雑な相互作用を浮き彫りにし ている。 |
| Environmental factors See also: Environmental racism and Race and health in the United States A positive correlation between minorities and a socioeconomic status of being low-income in industrialized and rural regions of the U.S. depict how low-income communities tend to include more individuals that have a lower educational background, most importantly in health. Income status, diet, and education all construct a higher burden for low-income minorities, to be conscious about their health. Research conducted by medical departments at universities in San Diego, Miami, Pennsylvania, and North Carolina suggested that minorities in regions where lower socioeconomic status is common, there was a direct relationship with unhealthy diets and greater distance of supermarkets.[68] Therefore, in areas where supermarkets are less accessible (food deserts) to impoverished areas, the more likely these groups are to purchase inexpensive fast food or just follow an unhealthy diet.[68] As a result, because food deserts are more prevalent in low income communities, minorities that reside in these areas are more prone to obesity, which can lead to diseases such as chronic kidney disease, hypertension, or diabetes.[68][69] Furthermore, this can also occur when minorities living in rural areas undergoing urbanization are introduced to fast food. A study completed in Thailand focused on urbanized metropolitan areas: students who participated were diagnosed as "non-obese" in their early life according to their BMI, however were increasingly at risk of developing type 2 diabetes, or obesity as adults, as opposed to young adults who lived in more rural areas during their early life.[70] Therefore, early exposure to urbanized regions can encourage unhealthy eating due to widespread presence of inexpensive fast food. Different racial populations that originate from more rural areas and then immigrate to the urbanized metropolitan areas can develop a fixation for a more westernized diet; this change in lifestyle typically occurs due to loss of traditional values when adapting to a new environment. For example, a 2009 study named CYKIDS was based on children from Cyprus, a country east of the Mediterranean Sea, who were evaluated by the KIDMED index to test their adherence to a Mediterranean diet after changing from a rural residence to an urban residence.[71] It was found that children in urban areas swapped their traditional dietary patterns for a diet favoring fast food. |
環境要因 こちらも参照のこと: 環境人種主義、米国における人種と保健 米国の先進工業地域や農村部では、マイノリティと低所得という社会経済的地位の間に正の相関関係があり、低所得のコミュニティには、保健上最も重要な教育 的背景の低い人々が多く含まれる傾向があることを示している。所得状況、食生活、教育のすべてが、低所得のマイノリティにとって、保健を意識するためのよ り高い負担を構築している。サンディエゴ、マイアミ、ペンシルバニア、ノースカロライナの大学の医学部で行われた研究では、社会経済的地位の低い地域のマ イノリティは、不健康な食生活とスーパーマーケットからの距離が遠いという直接的な関係があることが示唆された。 [68]したがって、貧困地域にとってスーパーマーケットへのアクセスが悪い地域(フードデザート)では、これらのグループが安価なファーストフードを購 入したり、不健康な食生活を送る可能性が高くなる[68]。その結果、フードデザートは低所得者層により多く見られるため、これらの地域に住むマイノリ ティは肥満になりやすく、慢性腎臓病、高血圧、糖尿病などの病気につながる可能性がある[68][69]。 さらに、都市化が進む農村部に住むマイノリティがファストフードを食べるようになった場合にも、このような現象が起こる可能性がある。タイで実施された研 究では、都市化された大都市圏に焦点が 当てられている。参加した学生は、幼少期にはBMIにより「非肥満」 と診断されたが、成人になると2型糖尿病や肥満を発症するリスクが高 まり、幼少期に農村部に住んでいた若年成人とは対照的であった[70]。 したがって、都市化された地域に早くから接していると、安価なファストフードが広く 存在するため、不健康な食生活を助長する可能性がある。農村部出身の異なる人種集団が、都市化された大都市圏に移住することで、より西洋化された食生活に 固執するようになることがある。このようなライフスタイルの変化は、新しい環境に適応する際に伝統的な価値観が失われるために起こるのが一般的である。例 えば、CYKIDSと名づけられた2009年の研究は、地中海の東に位置するキプロスの子どもたちを対象としたもので、農村部から都市部へと居住地を変え た後、地中海食の遵守度を調べるためにKIDMED指数によって評価された[71]。その結果、都市部の子どもたちは、伝統的な食事パターンをファスト フードを好む食事に置き換えていることが判明した。 |
| Genetic factors The fact that every human has a unique genetic code is the key to techniques such as genetic fingerprinting. Versions of genetic markers, known as alleles, occur at different frequencies in different human populations; populations that are more geographically and ancestrally remote tend to differ more. A phenotype is the "outward, physical manifestation" of an organism."[This quote needs a citation] For humans, phenotypic differences are most readily seen via skin color, eye color, hair color, or height; however, any observable structure, function, or behavior can be considered part of a phenotype. A genotype is the "internally coded, inheritable information" carried by all living organisms. The human genome is encoded in DNA.[citation needed] For any trait of interest, observed differences among individuals "may be due to differences in the genes" coding for a trait and "the result of variation in environmental condition". This variability is due to gene-environment interactions that influence genetic expression patterns and trait heritability.[72] For humans, there is "more genetic variation among individual people than between larger racial groups".[15] In general, an average of 80% of genetic variation exists within local populations, around 10% is between local populations within the same continent, and approximately 8% of variation occurs between large groups living on different continents.[73][74][75] Studies have found evidence of genetic differences between populations, but the distribution of genetic variants within and among human populations is impossible to describe succinctly because of the difficulty of defining a "population", the clinal nature of variation, and heterogeneity across the genome.[76] Thus, the racialization of science and medicine can lead to controversy when the term population and race are used interchangeably. |
遺伝的要因 すべての人間が固有の遺伝暗号を持っているという事実が、遺伝子指紋のような技術の鍵である。対立遺伝子として知られる遺伝子マーカーは、ヒトの集団に よって異なる頻度で出現する。 表現型とは、生物の 「外見上の、物理的な現れ 」のことである。遺伝子型とは、すべての生物が持っている「内部でコード化された遺伝可能な情報」である。ヒトゲノムはDNAにコード化されている。 関心のある形質について、個体間で観察される差異は、形質をコードする「遺伝子の違いによるもの」であり、「環境条件のばらつきの結果」である可能性があ る。この変動は、遺伝子の発現パターンや形質の遺伝率に影響を与える遺伝子-環境相互作用によるものである[72]。 一般的に、遺伝的変異の平均80%が地域集団内に存在し、約10%が同一大陸内の地域集団間に存在し、約8%が異なる大陸に住む大きな集団間に存在する。 [73][74][75]研究は集団間の遺伝的差異の証拠を発見しているが、「集団」を定義することの難しさ、変異のクリンナルな性質、ゲノム全体にわた る不均一性のため、ヒト集団内および集団間の遺伝的変異の分布を簡潔に記述することは不可能である[76]。したがって、科学と医学の人種化は、集団と人 種という用語が同じ意味で使用されると論争を引き起こす可能性がある。 |
| Evolutionary factors See also: Heterozygote advantage 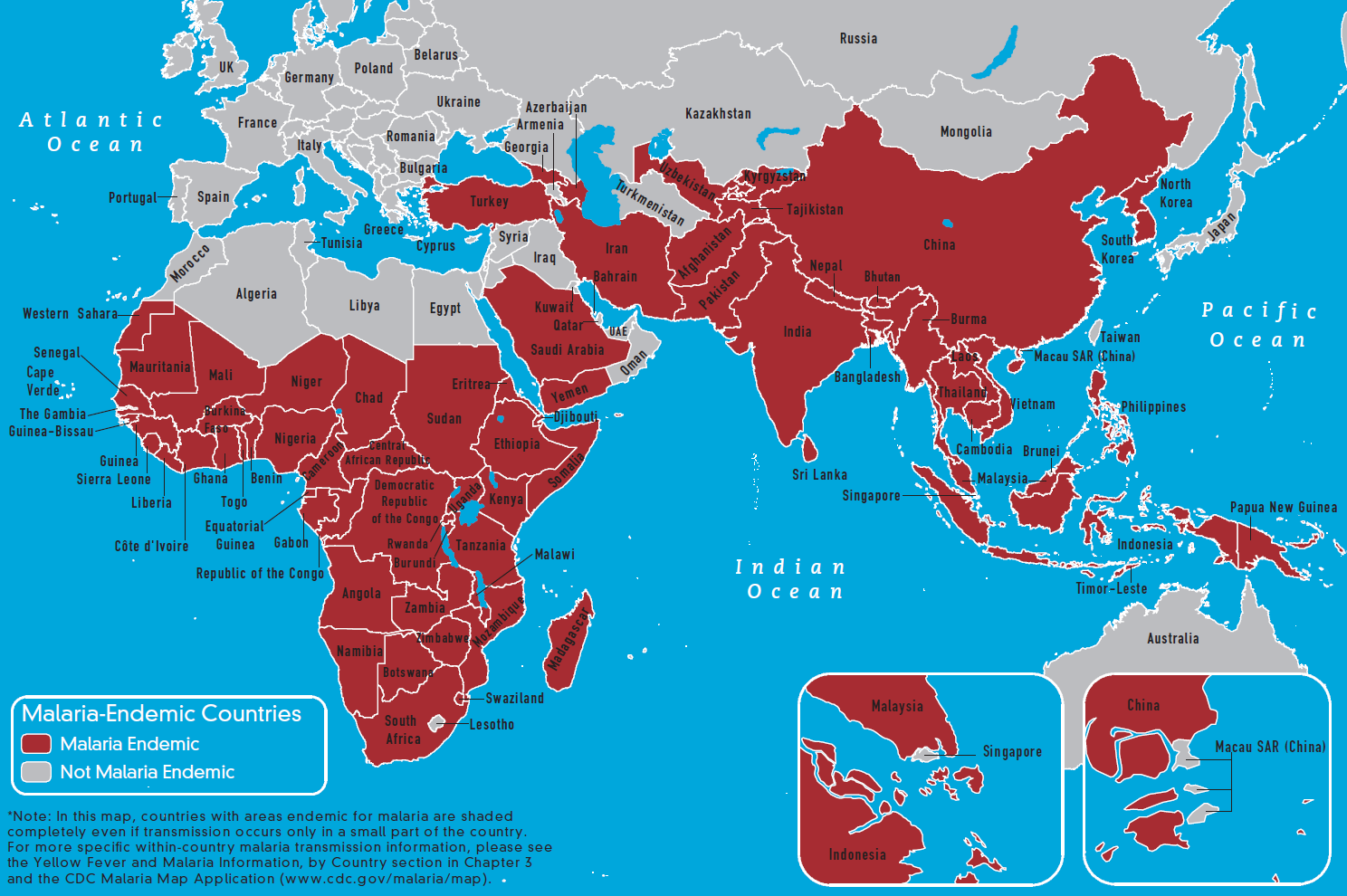 Currently malaria-endemic countries in the eastern hemisphere  Currently malaria-endemic countries in the western hemisphere Genes may be under strong selection in response to local diseases. For example, people who are duffy negative tend to have higher resistance to malaria. Most Africans are duffy negative and most non-Africans are duffy positive due to endemic transmission of malaria in Africa.[77] A number of genetic diseases more prevalent in malaria-affected areas may provide some genetic resistance to malaria including sickle cell disease, thalassaemias, glucose-6-phosphate dehydrogenase, and possibly others. Many theories about the origin of the cystic fibrosis have suggested that it provides a heterozygote advantage by giving resistance to diseases earlier common in Europe. In earlier research, a common theory was the "common disease-common variant" model. It argues that for common illnesses, the genetic contribution comes from the additive or multiplicative effects of gene variants that each one is common in the population. Each such gene variant is argued to cause only a small risk of disease and no single variant is sufficient or necessary to cause the disease. An individual must have many of these common gene variants in order for the risk of disease to be substantial.[78] More recent research indicates that the "common disease-rare variant" may be a better explanation for many common diseases. In this model, rare but higher-risk gene variants cause common diseases.[79] This model may be relevant for diseases that reduces fertility.[80] In contrast, for common genes associated with common disease to persist they must either have little effect during the reproductive period of life (like Alzheimer's disease) or provide some advantage in the original environment (like genes causing autoimmune diseases also providing resistance against infections). In either case varying frequencies of genes variants in different populations may be an explanation for health disparities.[78] Genetic variants associated with Alzheimer's disease, deep venous thrombosis, Crohn disease, and type 2 diabetes appear to adhere to "common disease-common variant" model.[81] |
進化的要因 こちらも参照のこと: ヘテロ接合体の優位性 東半球の現在のマラリア流行国 西半球の現在のマラリア流行国 遺伝子は、その地域の病気に対応して強い淘汰を受けている可能性がある。例えば、ダッフィー陰性の人はマラリアに対する抵抗性が高い傾向がある。アフリカ ではマラリアが流行しているため、アフリカ人のほとんどがダッフィー陰性であり、非アフリカ人のほとんどがダッフィー陽性である[77]。マラリア感染地 域でより流行している多くの遺伝性疾患は、鎌状赤血球症、タラセミア、グルコース-6-リン酸脱水素酵素、そしておそらくその他を含むマラリアに対する遺 伝的耐性をもたらす可能性がある。 子宮蓄膿症の起源に関する多くの説は、子宮蓄膿症がヨーロッパで一般的であった病気に対する耐性を与えることによって、ヘテロ接合体の利点をもたらすとい うものである。 以前の研究では、「共通疾患-共通変異体」モデルが一般的であった。これは、一般的な病気については、遺伝的な寄与は、それぞれが集団で一般的な遺伝子変 異の相加的または相乗的な影響によるものであると主張するものである。このような遺伝子変異は、それぞれわずかな疾病リスクを引き起こすだけであり、単一 の変異が疾病を引き起こすのに十分であったり必要であったりすることはないと主張する。疾患のリスクが相当なものになるためには、個体がこれらの共通遺伝 子変異を多く持っている必要がある[78]。 より最近の研究では、「一般的な疾患-まれなバリアント」が、多くの一般的な疾患に対するより良い説明である可能性が示されている。このモデルでは、希少 だがリスクの高い遺伝子変異が一般的な疾患を引き起こす[79]。対照的に、一般的な疾患と関連する一般的な遺伝子が存続するためには、生殖期にはほとん ど影響を及ぼさないか(アルツハイマー病のように)、あるいは元の環境において何らかの利点を提供しなければならない(自己免疫疾患の原因遺伝子が感染症 に対する抵抗性をも提供するように)。いずれにせよ、異なる集団における遺伝子変異の頻度の違いが、保健格差の説明となる可能性がある[78]。アルツハ イマー病、深部静脈血栓症、クローン病、2型糖尿病に関連する遺伝子変異は、「共通疾患-共通変異」モデルに準拠しているようである[81]。 |
| Gene flow Gene flow and admixture can also have an effect on relationships between race and race-linked disorders. Multiple sclerosis, for example, is typically associated with people of European descent, but due to admixture African Americans have elevated levels of the disorder relative to Africans.[82] Some diseases and physiological variables vary depending upon their admixture ratios. Examples include measures of insulin functioning[83] and obesity.[84] |
遺伝子の流れ 遺伝子の流れや混血は、人種と人種に関連する疾患との関係にも影響を及ぼすことがある。例えば、多発性硬化症は一般的にヨーロッパ系の人々と関連している が、混血によりアフリカ系アメリカ人はアフリカ系アメリカ人に比べてこの疾患のレベルが高い[82]。 混血比率によって変化する疾患や生理学的変数もある。例えば、インスリン機能[83]や肥満[84]などである。 |
| Gene interactions The same gene variant, or group of gene variants, may produce different effects in different populations depending on differences in the gene variants, or groups of gene variants, they interact with. One example is the rate of progression to AIDS and death in HIV–infected patients. In whites and Hispanics, HHC haplotypes were associated with disease retardation, particularly a delayed progression to death, while for African Americans, possession of HHC haplotypes was associated with disease acceleration. In contrast, while the disease-retarding effects of the CCR2-641 allele were found in African Americans, they were not found in whites.[85] |
遺伝子の相互作用 同じ遺伝子変異体、あるいは遺伝子変異体群が、相互作用する遺伝子変異体、あるいは遺伝子変異体群の違いによって、異なる集団で異なる効果をもたらすこと がある。その一例が、HIV感染者におけるAIDSへの進行と死亡の割合である。白人やヒスパニック系では、HHCハプロタイプは疾患の遅延、特に死亡へ の進行の遅延と関連していたが、アフリカ系アメリカ人ではHHCハプロタイプの保有は疾患の加速と関連していた。対照的に、CCR2-641対立遺伝子の 疾患抑制効果はアフリカ系アメリカ人では認められたが、白人では認められなかった[85]。 |
| Theoretical approaches in
addressing health and race disparities Public health researchers and policy makers are working to reduce health disparities. Health effects of racism are now a major area of research. In fact, these seem to be the primary research focus in biological and social sciences.[23] Interdisciplinary methods have been used to address how race affects health. according to published studies, many factors combine to affect the health of individuals and communities.[38] Whether people are healthy or not, is determined by their circumstances and environment. Factors that need to be addressed when looking at health and race include income and social status, education, physical environment, social support networks, genetics, health services, targeted instruction, and gender.[23][86][87][88] These determinants are often cited in public health, anthropology, and other social science disciplines. The WHO categorizes these determinants into three broader topics: the social and economic environment, the physical environment, and the person's individual characteristics and behaviors. Due to the diversity of factors that often attribute to health disparities outcomes, interdisciplinary approaches are often implemented.[86] For instance, Donna L. Washington and colleagues emphasize the importance of applying theoretical frameworks to reduce racial and ethnic disparities in healthcare. Their work highlights the ongoing inequalities in preventive, diagnostic, and therapeutic healthcare services for minority groups compared to white individuals, which contribute significantly to higher morbidity and mortality rates among these populations. To address these disparities, the authors recommend practical solutions such as improving communication between healthcare professionals and patients, adopting culturally and linguistically sensitive practices, implementing flexible payment options, and enrolling patients in financial assistance programs. These approaches align with interdisciplinary methods by combining cultural, economic, and social considerations to create actionable strategies that can be integrated into clinical practice. Such strategies exemplify how theoretical approaches can be translated into practical interventions to promote health equity.[89] |
保健と人種格差への理論的アプローチ 公衆衛生の研究者や政策立案者は、健康格差の是正に取り組んでいる。人種主義による保健への影響は、今や主要な研究分野となっている。実際、これらは生物 学や社会科学における主要な研究焦点となっているようである。[23] 人種が健康にどのような影響を及ぼすかを扱うために、学際的な方法が用いられてきた。発表された研究によると、多くの要因が組み合わさって個人や地域社会 の健康に影響を及ぼす。健康と人種を見る際に取り上げる必要のある要因には、所得や社会的地位、教育、物理的環境、社会的支援ネットワーク、遺伝、保健 サービス、対象を絞った指導、ジェンダーなどが含まれる[23][86][87][88]。これらの決定要因は、公衆衛生学、人類学、その他の社会科学の 分野でしばしば引用されている。WHOは、これらの決定因子を、社会的・経済的環境、物理的環境、人格の特性や行動の3つに分類している。保健医療格差の 結果をもたらす要因は多様であることが多いため、学際的なアプローチが実施されることが多い。 [86] 例えば、ドナ・L・ワシントン(Donna L. Washington)らは、保健医療における人種的・民族的格差を是正するために、理論的枠組みを適用することの重要性を強調している。彼らの研究は、 マイノリティ集団の予防、診断、治療におけるヘルスケアサービスの不平等が、白人集団に比べて進行中であることを強調しており、これらの集団における罹患 率や死亡率の上昇に大きく寄与している。 このような格差に対処するため、著者らは、医療従事者と患者間のコミュニケーションの改善、文化的・言語的に配慮した診療の採用、柔軟な支払い方法の導 入、経済的支援プログラムへの患者の登録といった実践的な解決策を推奨している。これらのアプローチは、文化的、経済的、社会的な考察を組み合わせること で、学際的な手法に合致し、臨床実践に統合可能な実行可能な戦略を生み出している。このような戦略は、理論的アプローチが保健の公平性を促進するための実 践的介入にどのように変換できるかを例証するものである [89] 。 |
| Interdisciplinarity or
interdisciplinary studies involves the combining of two or more
academic disciplines into one activity (e.g., a research project) The
term interdisciplinary is applied within education and training
pedagogies to describe studies that use methods and insights of several
established disciplines or traditional fields of study.
Interdisciplinarity involves researchers, students, and teachers in the
goals of connecting and integrating several academic schools of
thought, professions, or technologies—along with their specific
perspectives—in the pursuit of a common task. |
学際性(Interdisciplinarity)または学際的研究
(Interdisciplinary
Studies)とは、2つ以上の学問分野を1つの活動(研究プロジェクトなど)に融合させることを指す。学際的という用語は、教育や研修の教育学におい
て、確立された複数の学問分野や伝統的な研究分野の手法や見識を用いる研究を表すのに用いられる。学際性とは、研究者、学生、教師が、共通の課題を追求す
るために、複数の学問的な学派、専門職、あるいは技術を、それぞれの固有の視点とともに結びつけ、統合するという目標に関わることである。 |
| Biocultural approach Biocultural evolution was introduced and first used in the 1970s.[90] Biocultural methods focus on the interactions between humans and their environment to understand human biological adaptation and variation. These studies: "research on questions of human biology and medical ecology that specifically includes social, cultural, or behavioral variables in the research design, offer valuable models for studying the interface between biological and cultural factors affecting human well-being"[citation needed] This approach is useful in generating holistic viewpoints on human biological variation. There are two biocultural approach models. The first approach fuses biological, environmental, and cultural data. The second approach treats biological data as primary data and culture and environmental data as secondary. The salt sensitivity hypothesis is an example of implementing biocultural approaches in order to understand cardiovascular health disparities among African American populations. This theory, founded by Wilson and Grim, stems from the disproportional rates of salt sensitive high blood pressure seen between U.S. African American and White populations and between U.S. African American and West Africans as well. The researchers hypothesized that the patterns were in response to two events. One the trans-Atlantic slave trade, which resulted in massive death totals of Africans who were forced over, those who survived and made to the United States were more likely able to withstand the harsh conditions because they retained salt and water better. The selection continued once they were in the United States. African Americans who were able to withstand hard working conditions had better survival rates due to high water and salt retention. Second, today, because of different environmental conditions and increased salt intake with diets, water and salt retention are disadvantageous, leaving U.S. African Americans at disproportional risks because of their biological descent and culture.[91] |
生物文化的アプローチ 生物文化的進化は1970年代に導入され、最初に用いられた[90]。生物文化的手法は、ヒトの生物学的適応と変異を理解するために、ヒトとその環境との 相互作用に焦点を当てている。これらの研究は 「ヒトの生物学や医療生態学に関する問題で、特に社会的、文化的、あるいは行動的変数を研究デザインに含む研究は、人間の幸福に影響を与える生物学的要因 と文化的要因の接点を研究するための貴重なモデルを提供する」[要出典]。 このアプローチは、人間の生物学的変異に関する全体的な視点を生み出すのに有用である。生物文化的アプローチには2つのモデルがある。第一のアプローチ は、生物学的、環境的、文化的データを融合したものである。もう1つは、生物学的データを一次データとして扱い、文化や環境データを二次データとして扱う アプローチである。 塩感受性仮説は、アフリカ系アメリカ人集団の心血管保健格差を理解するために、生物文化的アプローチを導入した例である。WilsonとGrimによって 創始されたこの仮説は、米国のアフリカ系米国人と白人集団の間、および米国のアフリカ系米国人と西アフリカ人の間にも見られる食塩感受性高血圧の不釣り合 いな割合に由来する。研究者たちは、このパターンが2つの出来事に対応しているという仮説を立てた。ひとつは大西洋を横断する奴隷貿易で、強制的に連れて 行かれたアフリカ人が大量に死亡したこと、もうひとつは生き延びて米国に渡ったアフリカ人が、塩分や水分の保持力が高く、過酷な環境に耐えられる可能性が 高かったことである。アメリカに入ってからも、その選別は続いた。過酷な労働条件に耐えられるアフリカ系アメリカ人は、水分や塩分の保持力が高いため、生 存率が高かったのである。第二に、今日、異なる環境条件と食事による塩分摂取量の増加のため、保水力と塩分保持力は不利であり、米国のアフリカ系アメリカ 人は、その生物学的血統と文化のために、不釣り合いなリスクにさらされている[91]。 |
| Bio social inheritance model Similar to the biocultural approach, the bio social inheritance model also looks at biological and social methods in examining health disparities. Hoke et al. define Biosocial inheritance as "the process whereby social adversity in one generation is transmitted to the next through reinforcing biological and social mechanisms that impair health, exacerbating social and health disparities."[92] |
生物社会継承モデル 生物文化的アプローチと同様に、生物社会的継承モデルもまた、保健格差を検討する際に生物学的および社会的手法に注目する。Hokeらは、生物社会的継承 を「ある世代における社会的逆境が、健康を損なう生物学的・社会的メカニズムの強化を通じて次の世代に伝わり、社会的・健康的格差を悪化させるプロセス」 と定義している[92]。 |
| Controversy See also: Race (classification of humans), Race and genetics, and Objectification There is a controversy regarding race as a method for classifying humans. Different sources argue it is purely social construct[93] or a biological reality reflecting average genetic group differences. New interest in human biological variation has resulted in a resurgence of the use of race in biomedicine.[94] The main impetus for this development is the possibility of improving the prevention and treatment of certain diseases by predicting hard-to-ascertain factors, such as genetically conditioned health factors, based on more easily ascertained characteristics such as phenotype and racial self-identification. Since medical judgment often involves decision making under uncertain conditions,[95] many doctors consider it useful to take race into account when treating disease because diseases and treatment responses tend to cluster by geographic ancestry.[96] The discovery that more diseases than previously thought correlate with racial identification have further sparked the interest in using race as a proxy for bio-geographical ancestry and genetic buildup. Race in medicine is used as an approximation for more specific genetic and environmental risk factors. Race is thus partly a surrogate for environmental factors such as differences in socioeconomic status that are known to affect health. It is also an imperfect surrogate for ancestral geographic regions and differences in gene frequencies between different ancestral populations and thus differences in genes that can affect health. This can give an approximation of probability for disease or for preferred treatment, although the approximation is less than perfect.[15] Taking the example of sickle-cell disease, in an emergency room, knowing the geographic origin of a patient may help a doctor doing an initial diagnosis if a patient presents with symptoms compatible with this disease. This is unreliable evidence with the disease being present in many different groups as noted above with the trait also present in some Mediterranean European populations. Definitive diagnosis comes from examining the blood of the patient. In the US, screening for sickle cell anemia is done on all newborns regardless of race.[95] The continued use of racial categories has been criticized. Apart from the general controversy regarding race, some argue that the continued use of racial categories in health care and as risk factors could result in increased stereotyping and discrimination in society and health services.[15][97][98] Some of those who are critical of race as a biological concept see race as socially meaningful group that is important to study epidemiologically in order to reduce disparities.[99] For example, some racial groups are less likely than others to receive adequate treatment for osteoporosis, even after risk factors have been assessed. Since the 19th century, blacks have been thought to have thicker bones than whites have and to lose bone mass more slowly with age.[100] In a recent study, African Americans were shown to be substantially less likely to receive prescription osteoporosis medications than whites. Men were also significantly less likely to be treated compared with women. This discrepancy may be due to physicians' knowledge that, on average, African Americans are at lower risk for osteoporosis than whites. It may be possible that these physicians generalize this data to high-risk African-Americans, leading them to fail to appropriately assess and manage these individuals' osteoporosis.[100] On the other hand, some of those who are critical of race as a biological concept see race as socially meaningful group that is important to study epidemiologically in order to reduce disparities. Black Americans also have the highest mortality rate related to cardiovascular diseases, at about 30 percent higher than white Americans, even after the American Heart Association (AHA) has attempted to lower all risks.[101] David Williams (1994) argued, after an examination of articles in the journal Health Services Research during the 1966–90 period, that how race was determined and defined was seldom described. At a minimum, researchers should describe if race was assessed by self-report, proxy report, extraction from records, or direct observation. Race was also often used questionable, such as an indicator of socioeconomic status.[102] Racial genetic explanations may be overemphasized, ignoring the interaction with and the role of the environment.[103] |
論争 こちらも参照のこと: 人種(人間の分類)、人種と遺伝学、対象化 人間を分類する方法としての人種については論争がある。異なる情報源は、人種は純粋に社会的構築物[93]であるとか、平均的な遺伝的集団の違いを反映し た生物学的現実であると主張している。ヒトの生物学的変異に対する新たな関心が、生物医学における人種の使用の復活をもたらした[94]。 この発展の主なきっかけは、表現型や人種的自認のような、より容易に確認できる特徴に基づいて、遺伝的に条件付けられた保健要因のような、確認が困難な要 因を予測することによって、特定の疾病の予防や治療を改善できる可能性があることである。医学的判断はしばしば不確実な条件下での意思決定を伴うため [95]、多くの医師は疾病を治療する際に人種を考慮に入れることが有用であると考えている。以前考えられていたよりも多くの疾病が人種識別と相関してい ることが発見され、生物地理的な祖先や遺伝的蓄積の代理として人種を用いることへの関心がさらに高まっている[96]。 医学における人種は、より特異的な遺伝的・環境的危険因子の近似値として用いられている。このように、人種は、保健に影響を与えることが知られている社会 経済的地位の差異のような環境要因の代用品である。また、祖先の地理的地域や、異なる祖先集団間の遺伝子頻度の違い、したがって保健に影響しうる遺伝子の 違いに対する不完全な代用品でもある。この近似は完全ではないが、病気の確率や好ましい治療法の近似を与えることができる[15]。 鎌状赤血球症を例にとると、救急治療室において、患者がこの疾患に適合する症状を呈した場合、患者の地理的起源を知ることは、初期診断を行う医師の助けに なるかもしれない。鎌状赤血球症は、前述のように多くの異なる集団に存在し、一部の地中海ヨーロッパの集団にもその形質が見られることから、これは信頼で きない証拠である。確定診断は患者の血液を調べることによって行われる。米国では、鎌状赤血球貧血のスクリーニングは人種に関係なくすべての新生児に対し て行われている[95]。 人種分類の継続的な使用は批判されている。人種に関する一般的な論争とは別に、保健医療や危険因子として人種カテゴリーを使用し続けることは、社会や保健 サービスにおけるステレオタイプや差別を増大させる可能性があると主張する者もいる[15][97][98]。生物学的概念としての人種に批判的な者の中 には、人種は社会的に意味のある集団であり、格差を減らすために疫学的に研究することが重要であると考える者もいる[99]。 例えば、危険因子が評価された後でも、骨粗鬆症の適切な治療を受ける可能性が他の集団よりも低い人種がいる。19世紀以来、黒人は白人よりも骨が太く、加 齢に伴う骨量の減少が遅いと考えられてきた [100] 。また、女性に比べて男性の方が、治療を受ける可能性が有意に低かった。この不一致は、平均してアフリカ系アメリカ人は白人よりも骨粗鬆症のリスクが低い という医師の知識によるものかもしれない。このような医師が、リスクの高いアフリカ系アメリカ人にこのデータを一般化し、これらの人々の骨粗鬆症の適切な 評価と管理を怠ることにつながっている可能性がある。黒人アメリカ人はまた、アメリカ心臓協会(AHA)がすべてのリスクを下げようと試みた後でも、心血 管疾患に関する死亡率が最も高く、白人アメリカ人よりも約30%高い[101]。 David Williams (1994)は、1966年から90年の間に雑誌『Health Services Research』に掲載された論文を調査した結果、人種がどのように決定され定義されたかはほとんど記述されていないと主張した。少なくとも研究者は、 人種が自己申告、代理報告、記録からの抽出、または直接観察によって評価されたかどうかを記述すべきである。人種はまた、社会経済的地位の指標として使用 されるなど、疑問視されることも多かった[102]。人種的遺伝的説明が過度に強調され、環境との相互作用や環境の役割が無視されている可能性がある [103]。 |
| From concepts of race to ethnogenetic layering There is general agreement that a goal of health-related genetics should be to move past the weak surrogate relationships of racial health disparity and get to the root causes of health and disease. This includes research which strives to analyze human genetic variation in smaller groups than races across the world.[15] One such method is called ethnogenetic layering. It works by focusing on geographically identified microethnic groups. For example, in the Mississippi Delta region ethnogenetic layering might include such microethnic groups as the Cajun (as a subset of European Americans), the Creole and Black groups [with African origins in Senegambia, Central Africa and Bight of Benin] (as a subset of African Americans), and Choctaw, Houmas, Chickasaw, Coushatta, Caddo, Atakapa, Karankawa and Chitimacha peoples (as subsets of Native Americans).[104][105] Better still may be individual genetic assessment of relevant genes.[54] As genotyping and sequencing have become more accessible and affordable, avenues for determining individual genetic makeup have opened dramatically.[106] Even when such methods become commonly available, race will continue to be important when looking at groups instead of individuals such as in epidemiologic research.[54] Some doctors and scientists such as geneticist Neil Risch argue that using self-identified race as a proxy for ancestry is necessary to be able to get a sufficiently broad sample of different ancestral populations, and in turn to be able to provide health care that is tailored to the needs of minority groups.[43] |
人種概念から民族遺伝学的レイヤリングへ 保健に関連する遺伝学の目標は、人種による健康格差の弱い代理関係を乗り越え、健康と疾病の根本原因に迫ることであるという点で一般的な合意が得られている。これには、世界中の人種よりも小さな集団におけるヒトの遺伝的変異を分析しようとする研究も含まれる[15]。 そのような方法のひとつが、民族遺伝学的レイヤリングと呼ばれるものである。これは、地理的に特定されたミクロ民族集団に焦点を当てることで機能する。例 えば、ミシシッピ・デルタ地域では、(ヨーロッパ系アメリカ人のサブセットとしての)ケイジャン族、(アフリカ系アメリカ人のサブセットとしての)クレ オール族や黒人グループ[セネガンビア、中央アフリカ、ベナン湾にアフリカの起源を持つ]、(ネイティブ・アメリカンのサブセットとしての)チョクトー 族、ホウマ族、チカソー族、クシャッタ族、カド族、アタカパ族、カランカワ族、チチマチャ族などのミクロ民族グループが民族遺伝学的レイヤリングに含まれ る。 [104][105] 遺伝子型判定とシークエンシングがより利用しやすくなり、価格も手頃になったため、個人の遺伝的構成を決定する手段が劇的に開かれた[106]。 このような方法が一般的に利用できるようになったとしても、疫学調査など個人ではなく集団を調べる場合には、人種は引き続き重要である[54]。 遺伝学者のニール・リッシュのような一部の医師や科学者は、祖先の代理として自認する人種を使用することは、異なる祖先集団の十分な広範なサンプルを得る ために必要であり、ひいてはマイノリティ集団のニーズに合わせた保健医療を提供するために必要であると主張している[43]。 |
| Association studies See also: Genetic association One area in which population categories can be important considerations in genetics research is in controlling for confounding between population genetic substructure, environmental exposures, and health outcomes. Association studies can produce spurious results if cases and controls have differing allele frequencies for genes that are not related to the disease being studied,[107][108] although the magnitude of its problem in genetic association studies is subject to debate.[109][110] Various techniques detect and account for population substructure,[111][112] but these methods can be difficult to apply in practice.[113] Population genetic substructure also can aid genetic association studies. For example, populations that represent recent mixtures of separated ancestral groups can exhibit longer-range linkage disequilibrium between susceptibility alleles and genetic markers than is the case for other populations.[114][115][116][117] Genetic studies can use this disequilibrium to search for disease alleles with fewer markers than would be needed otherwise. Association studies also can take advantage of the contrasting experiences of racial or ethnic groups, including migrant groups, to search for interactions between particular alleles and environmental factors that might influence health.[118][119] |
関連研究 こちらも参照のこと: 遺伝的関連 遺伝学研究において集団カテゴリーが重要な考慮事項となりうる分野の一つは、集団の遺伝的下部構造、環境暴露、保健上の転帰の間の交絡をコントロールする ことである。しかし、遺伝的関連研究におけるこの問題の大きさについては議論の余地がある[109][110]。様々な手法が集団の部分構造を検出し、そ れを考慮する[111][112]が、これらの手法を実際に適用するのは困難である[113]。 集団遺伝的下部構造も遺伝的関連研究に役立つことがある。例えば、分離した祖先集団の最近の混合を示す集団は、他の集団の場合よりも長い範囲の連鎖不平衡 を感受性対立遺伝子と遺伝マーカーとの間に示すことがある[114][115][116][117]。遺伝学的研究はこの不平衡を利用して、他の方法で必 要とされるよりも少ないマーカーで疾患対立遺伝子を探索することができる。関連研究はまた、移民グループを含む人種または民族グループの対照的な経験を利 用して、個別対立遺伝子と保健に影響を及ぼす可能性のある環境因子との間の相互作用を探索することもできる[118][119]。 |
| Human genome projects |
ヒトゲノムプロジェクト(空欄) |
| Race and medical practice History Historically, race has been utilized in medicine in various ways, which continue to have enduring impacts today. The imposition of race on pulmonary function and the machinery used to conduct testing is a noteworthy example. Samuel Cartwright was a 19th-century physician and scientist who is known for his work on spirometry and respiratory physiology. Spirometry is a medical test that measures how much air a person can breathe in and out of their lungs, and how quickly they can do so. Cartwright used spirometry to compare Black enslaved people's lung function to white people's.[120] Cartwright, drawing on Thomas Jefferson's beliefs on pulmonary dysfunction, saw a 20% quantitative difference between Black and White people as proof of deficiency that necessitated the enslavement of Black individuals.[120] These findings of lower lung capacity by race are present in modern medicine through the correction of race in modern spirometry machines and within most textbooks for medical school.[121] When inputting race into the machine, patients either provide their self-identified race or it is determined by the provider. Spirometers in the US utilize population-specific standards or correction factors of 10% to 15% for Black persons and 4% to 6% for Asian people.[122] Thus, equations derived from Black populations will yield a higher percentage of predicted lung function values than those derived from White populations, which may underestimate lung disease severity and delay detection. However, applying an equation developed from White populations to other racial groups may lead to overdiagnosis and limited eligibility for treatment due to the increased perception of risk.[123] Research regarding the efficacy of race-based spirometry found that the race correction was only accurate for Black patients when their African ancestry was above the median between 81 and 100%.[124] As a result, opponents of race correction say it may cause misdiagnosis and perpetuate racial prejudices by encouraging biological race.[123][122] These race-based clinical decision support tools, such as pulmonary function testing with spirometry, were ended by a report published by the US House of Representatives Ways and Means Committee in October 2021.[125] |
人種と医療行為 歴史 歴史的に、人種はさまざまな形で医療に利用されてきた。肺機能や検査に使われる機械に人種を押し付けたのは、その顕著な例である。サミュエル・カートライ トは19世紀の医師であり科学者で、スパイロメトリーと呼吸生理学の研究で知られている。スパイロメトリーとは、人格が肺からどれだけの量の空気を吸った り吐いたりできるか、またどれだけの速さでそれができるかを測定する医学的検査である。カートライトはスパイロメトリーを使って、奴隷にされた黒人の肺機 能を白人の肺機能と比較した[120]。カートライトは、肺機能障害に関するトーマス・ジェファーソンの信念に基づいて、黒人と白人の間に20%の量的な 差があることを、黒人を奴隷にする必要がある欠乏の証拠であると考えた[120]。 人種によって肺活量が低いというこれらの知見は、現代のスパイロメトリー装置における人種の補正や、医学部の教科書のほとんどを通じて、現代医学の中に存 在している[121]。米国のスパイロメーターは、黒人については10%~15%、アジア人については4%~6%の集団固有の基準または補正係数を利用し ている[122] 。したがって、黒人の集団から得られた計算式は、白人の集団から得られた計算式よりも肺機能予測値の割合が高くなり、肺疾患の重症度を過小評価して発見を 遅らせる可能性がある。しかし、白人の集団から開発された式を他の人種集団に適用すると、リスクの認識が高まるため、過剰診断となり、治療の適格性が制限 される可能性がある [123] 。人種に基づくスパイロメトリーの有効性に関する研究では、人種補正が黒人患者に対して正確であったのは、アフリカ系の祖先が81~100%の間の中央値 を超えている場合のみであることが判明した。 [124] その結果、人種補正に反対する人々は、生物学的人種を奨励することによって誤診を引き起こし、人種的偏見を永続させる可能性があると述べている[123] [122]。スパイロメトリーによる肺機能検査などのこうした人種に基づく臨床判断支援ツールは、2021年10月に米国下院のWays and Means Committeeによって発表された報告書によって廃止された[125]。 |
| Sources of racial disparities in care In a report by the Institute of Medicine called Unequal Treatment, three major source categories are put forth as potential explanations for disparities in health care: patient-level variables, healthcare system-level factors, and care process-level variables.[126] |
ケアにおける人種間格差の原因 Unequal Treatmentと呼ばれる医学研究所の報告書では、保健医療における格差の潜在的な説明として、3つの主要な原因カテゴリーが提示されている:患者レベルの変数、医療システムレベルの要因、およびケアプロセスレベルの変数である[126]。 |
| Patient-level variables There are many individual factors that could explain the established differences in health care between different racial and ethnic groups. First, attitudes and behaviors of minority patients are different. They are more likely to refuse recommended services, adhere poorly to treatment regimens, and delay seeking care, yet despite this, these behaviors and attitudes are unlikely to explain the differences in health care.[126] In addition to behaviors and attitudes, biological based racial differences have been documented, but these also seem unlikely to explain the majority of observed disparities in care.[126] |
患者レベルの変数 人種や民族の異なるグループ間で保健医療に確立された差異を説明しうる多くの個人的要因がある。第一に、マイノリティ患者の態度や行動は異なる。彼らは、 推奨されるサービスを拒否したり、治療レジメンをあまり守らなかったり、受診を遅らせたりする傾向があるが、それにもかかわらず、これらの行動や態度が保 健ケアの差を説明するとは考えにくい[126]。行動や態度に加えて、生物学的根拠に基づく人種差も記録されているが、これらもまた、観察されたケアの格 差の大部分を説明するとは考えにくいようである[126]。 |
| Health system-level factors Health system-level factors include any aspects of health systems that can have different effects on patient outcomes. Some of these factors include different access to services, access to insurance or other means to pay for services, access to adequate language and interpretation services, and geographic availability of different services.[126] Many studies assert that these factors explain portions of the existing disparities in health of racial and ethnic minorities in the United States when compared to their white counterparts. |
保健システムレベルの要因 保健システムレベルの因子には、患者の転帰に異なる影響を及ぼしうる保健システムのあらゆる側面が含まれる。このような要因の中には、サービスへのアクセ スの違い、保険やその他のサービス費用の支払い手段へのアクセス、適切な言語や通訳サービスへのアクセス、地理的に異なるサービスを利用できることなどが ある [126] 。 |
| Care process-level variables Three major mechanisms are suggested by the Institute of Medicine that may contribute to healthcare disparities from the provider's side: bias (or prejudice) against racial and ethnic minorities; greater clinical uncertainty when interacting with minority patients; and beliefs held by the provider about the behavior or health of minorities.[126] While research in this area is ongoing, some exclusions within clinical trials themselves are also present. A recent systematic review of the literature relating to hearing loss in adults demonstrated that many studies fail to include aspects of racial or ethnic diversity, resulting in studies that do not necessarily represent the US population.[127] A 2023 scoping review of the literature found that in studies conducted in multiracial or multiethnic populations, the inclusion of race or ethnicity variables lacked thoughtful conceptualization and informative analysis regarding race or ethnicity as indicators of exposure to racialized social disadvantage, the systemic and structural barriers, discrimination, and social exclusion faced by individuals and communities based on their race or ethnicity, leading to disparities in access to resources, opportunities, and health outcomes.[12][11] |
ケア過程レベルの変数 人種的・民族的マイノリティに対する偏見(または偏見)、マイノリティ患者と接する際の臨床的不確実性の増大、マイノリティの行動や保健について医療提供 者が抱いている信念 [126] この分野の研究は現在も進行中であるが、臨床試験自体における除外も存在する。成人の難聴に関する文献の最近の系統的レビューでは、多くの研究が人種や民 族の多様性の側面を含んでおらず、その結果、研究が必ずしも米国人口を代表していないことが示された[127]。 2023年の文献のスコーピングレビューでは、多人種または多民族の集団で実施された研究において、人種または民族性の変数を含めることは、人種化された 社会的不利、すなわち人種または民族性に基づいて個人や地域社会が直面する制度的・構造的障壁、差別、社会的排除への曝露の指標としての人種または民族性 に関する思慮深い概念化と有益な分析を欠いており、資源、機会、保健結果へのアクセスにおける格差につながっていることが明らかにされた[12] [11]。 |
| Average human height by country Dark skin § Health implications Ethnic bioweapon Environmental racism French paradox HapMap[128] Hispanic paradox Mexican paradox Light skin § Health implications List of countries by life expectancy Social determinants of health in poverty § Ethnicity Ethnopsychopharmacology Cystic fibrosis and race United States: Center for Minority Health Environmental Racism in the United States Race and health in the United States |
国別平均身長 黒い肌 § 保健への影響 民族生物兵器 環境人種主義 フレンチ・パラドックス ハップマップ[128] ヒスパニックのパラドックス メキシコ人のパラドックス 明るい肌 § 保健への影響 平均寿命の国別リスト 貧困における保健の社会的決定要因 § エスニシティ 民族精神薬理学 嚢胞性線維症と人種 米国 マイノリティ保健センター 米国における環境人種主義 アメリカにおける人種と保健 |
| https://en.wikipedia.org/wiki/Race_and_health |
リ ンク
文 献
そ の他の情報
Copyleft,
CC, Mitzub'ixi Quq Chi'j, 1996-2099
Copyleft, CC, Mitzub'ixi Quq Chi'j, 1996-2099
![]()
☆
 ☆
☆