補完代替医療
Complementary and Alternative Medicine, CAM
解説:池田光穂
補完代替医療 (Complementary and Alternative Medicine, CAM)、補完代替医療には、代替補完医療(Alternative and Complimentary medicine)、補完医療(Complimentary medicine)、代替医療(aternative medicine)などの同義語がある。
| 代替医療(aternative medicine) | 文字通り近代医療あるいはコスモポリタン医療が十分に普及していない部分で、その医療の代わりにおこなわれる医療。あるいは、近代医療あるいはコスモポリタン医療は普及する「以前の」医療で、現時点では近代医療あるいはコスモポリタン医療の代わりに(aternative)に動員されている医療。 |
| 補完医療(Complimentary medicine) | 近代医療あるいはコスモポリタン医療が十分に普及しても、近代医療あるいはコスモポリタン医療から得られない利得(ベネフィット)を追求するために、使われている医療。 |
★補完代替医療の定義
米国の国立がん研究所 (National Cancer Intsitute)では、(がん患者のニーズの高い)補完代替医療は、「『標準的な医療ケア』の部分ではない、医療的産物と諸実践である(the term for medical products and practices that are not part of standard medical care)」と解説している。つまり、米国では、医師(M.D., medical doctor)と整骨治療医師(D.O., doctor of osteopathy)の学位をもつ専門家、ならびに「理学療法士、医療助手、臨床心理学者、そして看護師」がおこなう実践のみが「標準的な医療ケア」の範囲に含まれているのであり、それ以外は、実質的に全 部、補完代替医療 と呼ばれるのである。「標準的な医療ケア」 とは、生物医療、アロパシー、西洋起源の、主流をなしている、正統的な、あるいは通常の医療(biomedicine or allopathic, Western, mainstream, orthodox, or regular medicine)のことである。ここでアロパシー医療とは日本では馴染みのない言葉であるが、いわゆる西洋医学の主流の方法であり、それはホメオパシー 医療(同毒療法などといわれ一般に医学的根拠がないと証明された医療)ではないものを指している(→Complementary and Alternative Medicine, by NCI)。もっとも、北米大陸やヨーロッパ大陸では、ホメオパシー医療はとても人気があり、それは東アジアにお ける中国伝統医療と同じくらいであるということを忘れてはならない。
つまり、補完代替医療とは、主流派ではない非正統的医療のことであ る。米国の補完代替医療(CAM)と重なる部分があるにも関わらず(先に述べた)日本の統合医療は、日本の医学界にきちんと した地歩を持っているために、日本では正当性が与えられている違いがある(→Complementary and Alternative Medicine, by NCI)。
Complementary and Alternative Medicine, CAM =
Complementary medicine + Alternative medicine
Integrative medicine = (main) Integrative
medicine + effective CAM
ジョンズホプキンス大学のサイト では「伝統的代替医療」につぎの5つの療法を列挙している。つまり、(i)鍼[Acupuncture]、(ii)アーユルベーダー [Ayurveda]、(iii)ホメオパシー[Homeopathy]、(iv)ナチュロパシー[Naturopathy]、(v)中国あるいは東洋医療[Chinese or Oriental medicine]、である。これは日本の伝統的施術者にとっては噴飯物かもしれないが、米国の通常の人たちにはこのような理 解が一般的である、ということを日本の伝統的施術者はきちんと理解しておかねばならない(→Types of Complementary and Alternative Medicine, by Johns Hopkins Medicine)。
※以下に代替医療の一例を紹介する。
★非科学的信条体系(Unscientific belief systems)
| 提唱されたメカニズム |
問題点(イシュー) | |
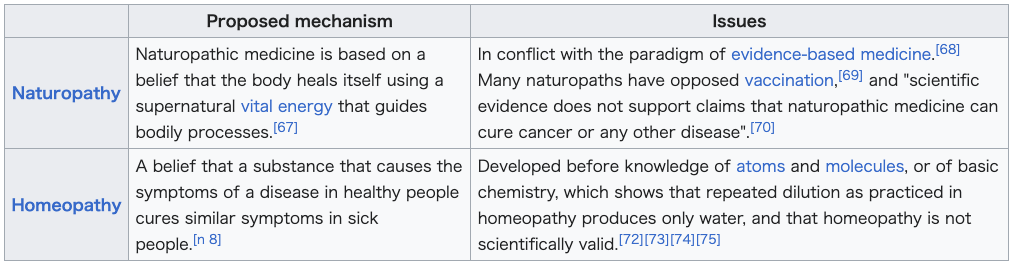
| ナチュロパシー(Naturopathy) |
自然療法(ナチュロパシー)は、身体が超自然的な生命エネルギーによって自らを癒し、身体のプロセスを導くという信念に基づいている。[67] |
エビデンスに基づく医療のパラダイムと矛盾している。[68]多くの自然療法医は予防接種に反対してきた。[69]そして「自然療法が癌やその他の病気を治せるとの主張を科学的な証拠は支持していない」。[70] |
| ホメオパシー(Homeopathy) |
同属療法(ホメオパシー)とは、ある物質が健康な人に病気の症状を引き起こす場合、その物質が病気の人の同様の症状を治すという考え。[n 8] |
原子や分子の知識、あるいは基礎化学の知識が確立される前に開発されたもので、ホメオパシーで実践されるような反復希釈は単なる水を生むだけであり、ホメオパシーは科学的に有効ではないことを示している。[72][73][74][75] |
☆
★伝統的民族体系(Traditional ethnic systems)
| その医学の内容(クレイム) |
問題点(イシュー) | |
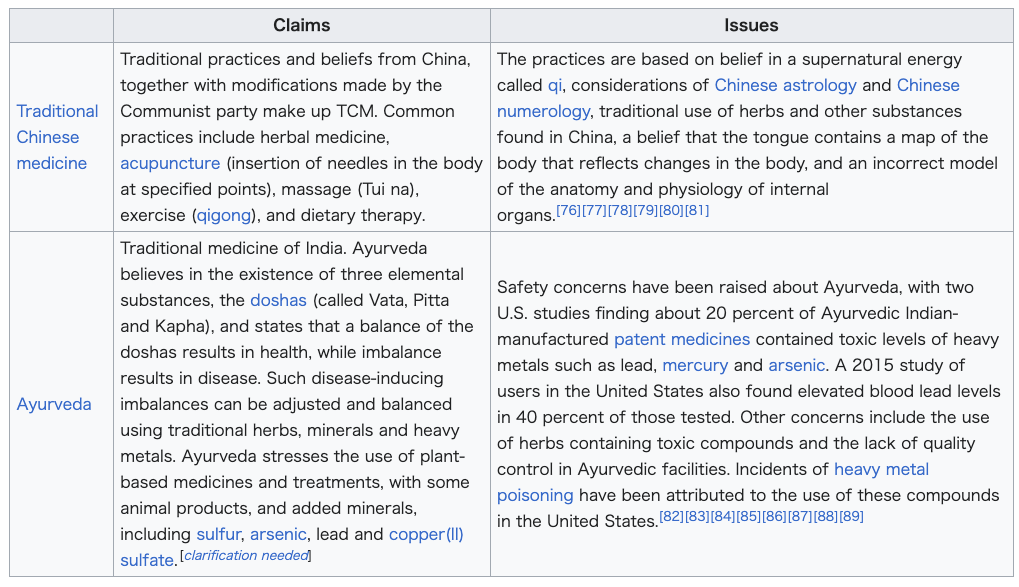
| 伝統的中国医学, TCM (Traditional Chinese medicine) |
中国の伝統的な医療行為と信仰、それに共産党による修正を加えたものが中医学である。一般的な治療法には、漢方薬、鍼治療(体の特定のポイントに針を刺す)、マッサージ(推拿)、運動療法(気功)、食事療法が含まれる。 |
これらの実践は、気と呼ばれる超自然的なエネルギーへの信
仰、中国占星術と中国数秘術の考察、中国で発見されたハーブやその他の物質の伝統的な使用、舌が身体の変化を反映する身体の地図を含んでいるという信念、
そして内臓の解剖学と生理学に関する誤ったモデルに基づいている。[76][77][78][79][80][81] |
| アーユルベーダ(Ayurveda) |
インドの伝統医学。アーユルヴェーダは三つの元素物質、
ドーシャ(ヴァータ、ピッタ、カパと呼ばれる)の存在を信じ、ドーシャの均衡が健康をもたらし、不均衡が病気を引き起こすと説く。こうした病気を誘発する
不均衡は、伝統的なハーブ、鉱物、重金属を用いて調整し均衡させることができる。アーユルヴェーダは植物由来の薬や治療法を重視し、一部の動物性製品や硫
黄、ヒ素、鉛、硫酸銅(II)などの鉱物を添加する。[くわしい説明が必要] |
アーユルヴェーダには安全性の懸念が指摘されている。米国
の2つの研究では、インド製アーユルヴェーダ特許医薬品の約20%に鉛、水銀、ヒ素などの有害なレベルの重金属が含まれていた。2015年の米国利用者調
査でも、検査対象者の40%で血中鉛濃度の上昇が確認された。その他の懸念事項には、有毒化合物を含むハーブの使用や、アーユルヴェーダ施設における品質
管理の欠如が含まれる。米国では、これらの化合物使用による重金属中毒事例が報告されている。[82][83][84][85][86][87][88]
[89] |
☆
☆
★超自然的エネルギー(Supernatural energies)
| その医学/療法の内容(クレイム) | 問題点(イシュー) | |
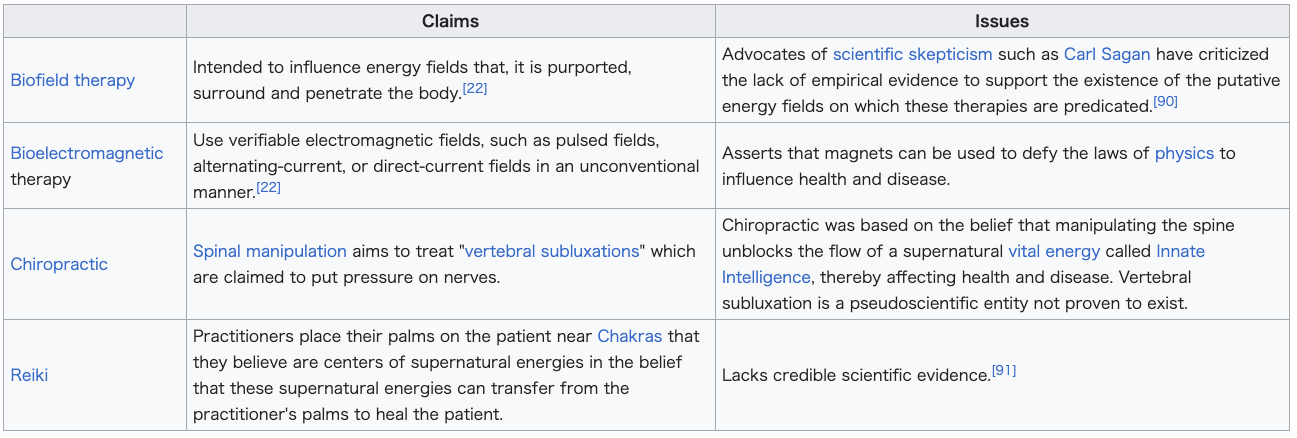
| バイオフィールド治療(Biofield therapy) |
身体を取り囲み、貫通していると言われるエネルギー場に影響を与えることを目的としている。[22] |
カール・セーガンのような科学的懐疑論の提唱者たちは、これらの療法の根拠となっているとされるエネルギー場の存在を裏付ける実証的証拠の欠如を批判している。[90] |
| 生体電磁気療法(Bioelectromagnetic therapy) |
パルス電磁場、交流電磁場、直流電磁場など、検証可能な電磁場を従来とは異なる方法で用いる。[22] |
磁石を使えば物理法則に逆らって健康や病気に影響を与えられると主張する。 |
| カイロプラクティック(Chiropractic) |
脊椎マニピュレーションは、神経に圧迫を与えるとされる「椎骨の亜脱臼」を治療することを目的としている。 |
カイロプラクティックは、脊椎を操作することで「生来の知性」と呼ばれる超自然的な生命エネルギーの流れが妨げられ、それによって健康や病気に影響を与えるという信念に基づいていた。椎骨の亜脱臼は、存在が証明されていない疑似科学的な概念である。 |
| 霊氣・レイキ(Reiki) |
施術者は、超自然的なエネルギーの中心点と信じているチャクラ付近に患者の体に掌を当てる。この超自然的なエネルギーが施術者の掌から患者に移り、治癒をもたらすと信じているからだ。 |
信頼できる科学的根拠が欠けている。[91] |
☆
★
| その医学/療法の内容(クレイム) | 問題点(イシュー) |
|
| クリスチャン信仰治療(Christian faith healing) |
癒しには神聖な、あるいは霊的な介入がある。 |
有効性を示す証拠がない。[95]
死亡や障害といった望ましくない結果が、「重傷や重病に対して医療ケアの代わりに信仰治療が選択された場合に発生した」。[96]
2001年の二重盲検試験(冠動脈手術後退院患者799名対象)では、「冠動脈ケアユニットでの入院後、執り成しの祈りが医療的転帰に有意な影響を与えな
かった」と報告されている。[97] |
☆

★
☆代替医療(Alternative
medicine)
| Alternative
medicine refers to practices that aim to achieve the healing
effects of conventional medicine, but that typically lack biological
plausibility, testability, repeatability, or supporting evidence of
effectiveness. Such practices are generally not part of evidence-based
medicine. Unlike modern medicine, which employs the scientific method
to test plausible therapies by way of responsible and ethical clinical
trials, producing repeatable evidence of either effect or of no effect,
alternative therapies reside outside of mainstream medicine[n 1][n 2]
and do not originate from using the scientific method, but instead rely
on testimonials, anecdotes, religion, tradition, superstition, belief
in supernatural "energies", pseudoscience, errors in reasoning,
propaganda, fraud, or other unscientific sources. Frequently used terms
for relevant practices are New Age medicine, pseudo-medicine,
unorthodox medicine, holistic medicine, fringe medicine, and
unconventional medicine, with little distinction from quackery. Some alternative practices are based on theories that contradict the established science of how the human body works; others appeal to the supernatural or superstitions to explain their effect or lack thereof. In others, the practice has plausibility but lacks a positive risk–benefit outcome probability. Research into alternative therapies often fails to follow proper research protocols (such as placebo-controlled trials, blind experiments and calculation of prior probability), providing invalid results. History has shown that if a method is proven to work, it eventually ceases to be alternative and becomes mainstream medicine. Much of the perceived effect of an alternative practice arises from a belief that it will be effective, the placebo effect, or from the treated condition resolving on its own (the natural course of disease). This is further exacerbated by the tendency to turn to alternative therapies upon the failure of medicine, at which point the condition will be at its worst and most likely to spontaneously improve. In the absence of this bias, especially for diseases that are not expected to get better by themselves such as cancer or HIV infection, multiple studies have shown significantly worse outcomes if patients turn to alternative therapies. While this may be because these patients avoid effective treatment, some alternative therapies are actively harmful (e.g. cyanide poisoning from amygdalin, or the intentional ingestion of hydrogen peroxide) or actively interfere with effective treatments. The alternative medicine sector is a highly profitable industry with a strong lobby,[1] and faces far less regulation over the use and marketing of unproven treatments. Complementary medicine (CM), complementary and alternative medicine (CAM), integrated medicine or integrative medicine (IM), and holistic medicine attempt to combine alternative practices with those of mainstream medicine. Traditional medicine practices become "alternative" when used outside their original settings and without proper scientific explanation and evidence. Alternative methods are often marketed as more "natural" or "holistic" than methods offered by medical science, that is sometimes derogatorily called "Big Pharma" by supporters of alternative medicine. Billions of dollars have been spent studying alternative medicine, with few or no positive results and many methods thoroughly disproven. |
代替医療とは、従来の医療と同等の治療効果を目的とするが、生物学的妥
当性、検証可能性、再現性、あるいは有効性を裏付ける証拠を通常欠いている実践を指す。こうした実践は一般的にエビデンスに基づく医療の一部ではない。現
代医学が科学的メソッドを用いて、責任ある倫理的な臨床試験によって妥当な治療法を検証し、効果の有無を再現可能な証拠として示すのとは異なり、代替療法
は主流の医学の外側に位置する[n 1][n
2]。科学的メソッドに基づくものではなく、体験談、逸話、宗教、伝統、迷信、超自然的な「エネルギー」への信仰、
疑似科学、推論の誤り、プロパガンダ、詐欺、その他の非科学的根拠に依拠している。関連する実践に対して頻繁に使用される用語には、ニューエイジ医療、疑
似医療、非正統医療、ホリスティック医療、フリンジ医療、非従来型医療などがあり、これらはペテン師的行為との区別がほとんどない。 一部の代替療法は、人体の働きに関する確立された科学と矛盾する理論に基づいている。また、その効果や無効性を説明するために超自然現象や迷信に訴えるも のもある。また、その実践には妥当性があるものの、リスクと利益のバランスがプラスとなる結果の確率が欠けている場合もある。代替療法の研究は、適切な研 究プロトコル(プラセボ対照試験、盲検化実験、事前確率の計算など)に従わないことが多く、無効な結果をもたらす。歴史が示すように、ある方法が有効であ ると証明されれば、それはやがて代替療法ではなくなり、主流の医療となる。 代替療法の効果の多くは、その有効性を信じるプラセボ効果、あるいは治療対象の病状が自然治癒する(自然経過)ことに起因している。この傾向は、医学的治 療が失敗した時点で代替療法に頼る傾向によってさらに悪化する。その時点では病状が最も深刻であり、自然治癒の可能性が最も高いのだ。このバイアスを除け ば、特にがんやHIV感染のように自然治癒が期待できない疾患において、代替療法を選択した患者は複数の研究で明らかに予後が悪化することが示されてい る。これは患者が有効な治療を回避するためかもしれないが、一部の代替療法は積極的に有害である(例:アミグダリンによるシアン化物中毒、過酸化水素の意 図的摂取)か、有効な治療を妨害する。 代替医療分野は強力なロビー活動[1]を持つ高収益産業であり、未検証治療の使用や販売に対する規制がはるかに緩い。補完医療(CM)、補完代替医療 (CAM)、統合医療(IM)、ホリスティック医療は、代替療法と主流医療を組み合わせようとするものだ。伝統医療の実践は、本来の環境外で使用され、適 切な科学的説明や証拠を伴わない場合、「代替」となる。代替療法は、医療科学が提供する手法よりも「自然」または「ホリスティック」であると宣伝されるこ とが多く、代替医療支持者からは時に「ビッグファーマ」と蔑称される。代替医療の研究には数十億ドルが費やされてきたが、肯定的な結果はほとんどなく、多 くの手法は完全に否定されている。 |
| Definitions and terminology See also: Terminology of alternative medicine  Marcia Angell: "There cannot be two kinds of medicine – conventional and alternative."[2] The terms alternative medicine, complementary medicine, integrative medicine, holistic medicine, natural medicine, unorthodox medicine, fringe medicine, unconventional medicine, and new age medicine are used interchangeably as having the same meaning and are almost synonymous in most contexts.[3][4][5][6] Terminology has shifted over time, reflecting the preferred branding of practitioners.[7] For example, the United States National Institutes of Health department studying alternative medicine, currently named the National Center for Complementary and Integrative Health (NCCIH), was established as the Office of Alternative Medicine (OAM) and was renamed the National Center for Complementary and Alternative Medicine (NCCAM) before obtaining its current name. Therapies are often framed as "natural" or "holistic", implicitly and intentionally suggesting that conventional medicine is "artificial" and "narrow in scope".[1][8] The meaning of the term "alternative" in the expression "alternative medicine", is not that it is an effective alternative to medical science (though some alternative medicine promoters may use the loose terminology to give the appearance of effectiveness).[9][10] Loose terminology may also be used to suggest meaning that a dichotomy exists when it does not (e.g., the use of the expressions "Western medicine" and "Eastern medicine" to suggest that the difference is a cultural difference between the Asian east and the European west, rather than that the difference is between evidence-based medicine and treatments that do not work).[9] |
定義と用語 関連項目:代替医療の用語 マーシア・アンジェル: 「医療に二種類——従来型と代替型——など存在しえない」[2] 代替医療、補完医療、統合医療、ホリスティック医療、自然療法、非正統医療、周辺医療、非従来型医療、ニューエイジ医療といった用語は、同じ意味を持つも のとして互換的に用いられ、ほとんどの文脈でほぼ同義である[3] [4][5][6] 用語は時代とともに変化し、施術者の好むブランディングを反映している。[7] 例えば、米国国立衛生研究所(NIH)の代替医療研究部門は、現在は国立補完統合医療センター(NCCIH)と命名されているが、設立当初は代替医療局 (OAM)と呼ばれ、その後国立補完代替医療センター(NCCAM)と改称され、現在の名称に至った。療法はしばしば「自然」または「ホリスティック」と 位置付けられ、暗黙的かつ意図的に、従来の医学が「人工的」で「視野が狭い」ことを示唆している。[1] [8] 「代替医療」という表現における「代替」の意味は、それが医学科学に代わる有効な選択肢であるということではない(ただし、一部の代替医療推進者は、効果 があるように見せかけるためにこの曖昧な用語を使うことがある)。[9][10] 曖昧な用語は、実際には存在しない二分法が存在するかのように示唆するためにも用いられる(例:「西洋医学」と「東洋医学」という表現を用いて、その差異 がアジアの東とヨーロッパの西という文化的差異であるかのように示唆し、実証に基づく医学と効果のない治療法との差異であることを隠す)。[9] |
| Alternative medicine Alternative medicine is defined loosely as a set of products, practices, and theories that are believed or perceived by their users to have the healing effects of medicine,[n 3][n 4] but whose effectiveness has not been established using scientific methods,[n 3][n 5][13][14][15][9] or whose theory and practice is not part of biomedicine,[n 4][n 1][n 2][n 6] or whose theories or practices are directly contradicted by scientific evidence or scientific principles used in biomedicine.[9][13][19] "Biomedicine" or "medicine" is that part of medical science that applies principles of biology, physiology, molecular biology, biophysics, and other natural sciences to clinical practice, using scientific methods to establish the effectiveness of that practice. Unlike medicine,[n 1] an alternative product or practice does not originate from using scientific methods, but may instead be based on hearsay, religion, tradition, superstition, belief in supernatural energies, pseudoscience, errors in reasoning, propaganda, fraud, or other unscientific sources.[n 5][9][11][13][19] Some other definitions seek to specify alternative medicine in terms of its social and political marginality to mainstream healthcare.[20] This can refer to the lack of support that alternative therapies receive from medical scientists regarding access to research funding, sympathetic coverage in the medical press, or inclusion in the standard medical curriculum.[20] For example, a widely used[21] definition devised by the US NCCIH calls it "a group of diverse medical and health care systems, practices, and products that are not generally considered part of conventional medicine".[22] However, these descriptive definitions are inadequate in the present-day when some conventional doctors offer alternative medical treatments and introductory courses or modules can be offered as part of standard undergraduate medical training;[23] alternative medicine is taught in more than half of US medical schools and US health insurers are increasingly willing to provide reimbursement for alternative therapies.[24] |
代替医療 代替医療とは、大まかに言えば、利用者が医療と同等の治療効果を持つと信じたり認識したりしている製品、施術、理論の集合体である[n 3][n 4]。しかしその有効性は科学的手法によって確立されていない[n 3][n 5][13]。[14][15][9] あるいはその理論や実践が生物医学の一部ではないもの[n 4][n 1][n 2][n 6]、あるいはその理論や実践が生物医学で使用される科学的証拠や科学的原理と直接矛盾するもの。[9][13][19] 「生物医学」または「医学」とは、生物学、生理学、分子生物学、生物物理学、その他の自然科学の原理を臨床実践に応用し、その実践の有効性を科学的方法を 用いて確立する医学科学の一分野である。医学とは異なり、代替製品や実践は科学的方法の使用に由来せず、代わりに伝聞、宗教、伝統、迷信、超自然的エネル ギーへの信仰、疑似科学、推論の誤り、プロパガンダ、詐欺、その他の非科学的根拠に基づいている場合がある。 他の定義では、代替医療を主流医療に対する社会的・政治的周縁性という観点から特定しようとする[20]。これは、代替療法が研究資金へのアクセス、医学 メディアにおける好意的な報道、標準的な医学カリキュラムへの組み込みに関して、医学研究者から十分な支援を得られていない状況を指す場合がある。 [20] 例えば、米国国立補完統合医療センター(NCCIH)が考案した広く用いられる[21]定義では、代替医療を「一般に従来型医療の一部とは見なされない多 様な医療・健康システム、実践、製品群」と位置付けている。[22] しかし、現代においてはこうした記述的定義は不十分である。なぜなら、一部の従来型医師が代替医療的治療を提供し、標準的な学部医学教育の一環として入門 コースやモジュールが提供される場合があるからだ[23]。米国の医学部の半数以上で代替医療が教えられており、米国の健康保険会社は代替療法に対する償 還を提供する意向を強めている[24]。 |
| Complementary or integrative
medicine Complementary medicine (CM) or integrative medicine (IM) is when alternative medicine is used together with mainstream medical treatment in a belief that it improves the effect of treatments.[n 7][11][26][27][28] For example, acupuncture (piercing the body with needles to influence the flow of a supernatural energy) might be believed to increase the effectiveness or "complement" science-based medicine when used at the same time.[29][30][31] Significant drug interactions caused by alternative therapies may make treatments less effective, notably in cancer therapy.[32][33][34] Several medical organizations differentiate between complementary and alternative medicine including the UK National Health Service (NHS),[35] Cancer Research UK,[36] and the US Center for Disease Control and Prevention (CDC), the latter of which states that "Complementary medicine is used in addition to standard treatments" whereas "Alternative medicine is used instead of standard treatments."[37] Complementary and integrative interventions are used to improve fatigue in adult cancer patients.[38][39] David Gorski has described integrative medicine as an attempt to bring pseudoscience into academic science-based medicine[40] with skeptics such as Gorski and David Colquhoun referring to this with the pejorative term "quackademia".[41] Robert Todd Carroll described Integrative medicine as "a synonym for 'alternative' medicine that, at its worst, integrates sense with nonsense. At its best, integrative medicine supports both consensus treatments of science-based medicine and treatments that the science, while promising perhaps, does not justify"[42] Rose Shapiro has criticized the field of alternative medicine for rebranding the same practices as integrative medicine.[3] CAM is an abbreviation of the phrase complementary and alternative medicine.[43][44][45] The 2019 World Health Organization (WHO) Global Report on Traditional and Complementary Medicine states that the terms complementary and alternative medicine "refer to a broad set of health care practices that are not part of that country's own traditional or conventional medicine and are not fully integrated into the dominant health care system. They are used interchangeably with traditional medicine in some countries."[46] In the 1990s, integrative medicine started to be marketed by a new term, "functional medicine".[47] The Integrative Medicine Exam by the American Board of Physician Specialties[48] includes the following subjects: Manual Therapies, Biofield Therapies, Acupuncture, Movement Therapies, Expressive Arts, Traditional Chinese Medicine, Ayurveda, Indigenous Medical Systems, Homeopathic Medicine, Naturopathic Medicine, Osteopathic Medicine, Chiropractic, and Functional Medicine.[48] |
補完医療または統合医療 補完医療(CM)または統合医療(IM)とは、代替医療を主流の医療治療と併用し、治療効果を高めるとの考えに基づくものである。[n 7][11][26][27] [28] 例えば、鍼治療(超自然的なエネルギーの流れに影響を与えるために体に針を刺すこと)は、同時に使用することで科学に基づく医療の効果を高めたり「補完」 したりすると信じられている場合がある。[29][30][31] 代替療法による重大な薬物相互作用は、特にがん治療において、治療の効果を低下させる可能性がある。[32][33][34] 英国国民保健サービス(NHS)[35]、英国がん研究機構[36]、米国疾病予防管理センター(CDC)など、複数の医療機関が補完医療と代替医療を区 別している。後者は「補完医療は標準治療に加えて使用される」のに対し、「代替医療は標準治療の代わりに用いられる」と定義している[37]。 補完・統合的介入は、成人がん患者の疲労改善に用いられる。[38][39] デイヴィッド・ゴースキは、統合医療を疑似科学を学術的科学に基づく医療に取り込もうとする試みと説明している。[40]ゴースキやデイヴィッド・コル クーンといった懐疑論者は、これを蔑称「クワッカデミア」と呼んでいる。[41] ロバート・トッド・キャロルは統合医療を「最悪の場合、理性を非理性と統合する『代替』医療の同義語。最良の場合でも、科学に基づく医療の合意治療と、科 学的には有望かもしれないが正当化されない治療の両方を支持するもの」と評した[42]。ローズ・シャピロは代替医療分野が同じ実践を統合医療と再ブラン ド化した点を批判している。[3] CAMは補完代替医療(complementary and alternative medicine)の略語である。[43][44][45] 2019年の世界保健機関(WHO)伝統的・補完医療グローバル報告書は、補完代替医療という用語が「当該国の伝統的・標準医療の一部ではなく、主流医療 システムに完全に統合されていない広範な健康実践を指す」と述べている。一部の国では伝統医療と交替的に使用される」。[46] 1990年代、統合医療は新たな用語「機能性医療」として市場展開され始めた。[47] 米国医師専門委員会による統合医療試験[48]では、以下の科目が含まれる:手技療法、バイオフィールド療法、鍼治療、運動療法、表現芸術療法、伝統中国 医学、アーユルヴェーダ、先住民医療体系、ホメオパシー医学、自然療法医学、オステオパシー医学、カイロプラクティック、機能医学。[48] |
| Other terms See also: Traditional medicine Traditional medicine (TM) refers to certain practices within a culture which have existed since before the advent of medical science,[49][50] Many TM practices are based on "holistic" approaches to disease and health, versus the scientific evidence-based methods in conventional medicine.[51][52] The 2019 WHO report defines traditional medicine as "the sum total of the knowledge, skill and practices based on the theories, beliefs and experiences indigenous to different cultures, whether explicable or not, used in the maintenance of health as well as in the prevention, diagnosis, improvement or treatment of physical and mental illness."[46] When used outside the original setting and in the absence of scientific evidence, TM practices are typically referred to as "alternative medicine".[53][54][55] Holistic medicine is another rebranding of alternative medicine. In this case, the words balance and holism are often used alongside complementary or integrative, claiming to take into fuller account the "whole" person, in contrast to the supposed reductionism of medicine.[56][57] |
その他の用語 関連項目: 伝統医療 伝統医療(TM)とは、医学が生まれる以前から文化の中で存在してきた特定の医療行為を指す[49][50]。多くの伝統医療は、従来の医学における科学 的根拠に基づく方法とは対照的に、病気と健康に対する「全体論的」アプローチに基づいている[51][52]。2019年のWHO報告書は伝統医学を「健 康維持ならびに身体的・精神的疾患の予防、診断、改善、治療に用いられる、異なる文化に固有の理論、信念、経験に基づく知識、技術、実践の総体。その説明 可能性の有無を問わない」と定義している[46]。本来の環境外で使用され、科学的根拠を欠く場合、伝統医学の実践は通常「代替医療」と呼ばれる。 [53][54][55] ホリスティック医療は代替医療の別名である。この場合、「バランス」や「ホリスティック」という言葉が「補完的」や「統合的」と併せて用いられ、医学の還 元主義的傾向に対抗し、人格を「全体」としてより包括的に捉えると主張される。[56][57] |
| Challenges in defining
alternative medicine Prominent members of the science[58][59] and biomedical science community[2] say that it is not meaningful to define an alternative medicine that is separate from a conventional medicine because the expressions "conventional medicine", "alternative medicine", "complementary medicine", "integrative medicine", and "holistic medicine" do not refer to any medicine at all.[2][58][59][55] Others say that alternative medicine cannot be precisely defined because of the diversity of theories and practices it includes, and because the boundaries between alternative and conventional medicine overlap, are porous, and change.[16][60] Healthcare practices categorized as alternative may differ in their historical origin, theoretical basis, diagnostic technique, therapeutic practice and in their relationship to the medical mainstream.[61] Under a definition of alternative medicine as "non-mainstream", treatments considered alternative in one location may be considered conventional in another.[62] Critics say the expression is deceptive because it implies there is an effective alternative to science-based medicine, and that complementary is deceptive because it implies that the treatment increases the effectiveness of (complements) science-based medicine, while alternative medicines that have been tested nearly always have no measurable positive effect compared to a placebo.[9][40][63][64] Journalist John Diamond wrote that "there is really no such thing as alternative medicine, just medicine that works and medicine that doesn't",[59][65] a notion later echoed by Paul Offit: "The truth is there's no such thing as conventional or alternative or complementary or integrative or holistic medicine. There's only medicine that works and medicine that doesn't. And the best way to sort it out is by carefully evaluating scientific studies—not by visiting Internet chat rooms, reading magazine articles, or talking to friends."[58] |
代替医療の定義における課題 科学界[58][59]および生物医学界[2]の著名な研究者らは、代替医療を従来の医療とは別個のものとして定義することは意味がないと述べている。な ぜなら「従来の医療」「代替医療」「補完医療」「統合医療」「ホリスティック医療」といった表現は、いずれも特定の医療を指すものではないからだ。[2] [58][59][55] 他には、代替医療は包含する理論や実践が多様であること、また代替医療と従来型医療の境界が重なり合い、浸透しやすく、変化するため、正確に定義できない と主張する者もいる。代替医療に分類される医療行為は、歴史的起源、理論的根拠、診断技術、治療実践、そして主流医療との関係において異なる場合がある。 代替医療を「非主流」と定義すると、ある地域では代替療法と見なされる治療法が、別の地域では従来療法と見なされる可能性がある。[62] 批判者は、この表現が科学に基づく医療に効果的な代替手段があるかのように誤解を招くと指摘する。また「補完」という表現も、その治療法が科学に基づく医 療の効果を高める(補完する)かのように誤解を招くとされる。実際、検証された代替医療のほとんどは、プラセボと比較して測定可能な効果を示さない。 [9][40][63][64] ジャーナリストのジョン・ダイアモンドは「代替医療など実際には存在せず、効果のある医療と効果のない医療があるだけだ」と記した[59][65]。この 考えは後にポール・オフィットも「真実は、従来型医療や代替医療、補完医療、統合医療、ホリスティック医療などというものは存在しないということだ。効果 のある医療と効果のない医療だけがある。そしてそれを区別する最善の方法は、インターネットの掲示板を見たり雑誌記事を読んだり友人と話したりすることで はなく、科学的研究を慎重に評価することだ」と述べている。[58] |
| Types See also: List of forms of alternative medicine Alternative medicine consists of a wide range of health care practices, products, and therapies. The shared feature is a claim to heal that is not based on the scientific method. Alternative medicine practices are diverse in their foundations and methodologies.[22] Alternative medicine practices may be classified by their cultural origins or by the types of beliefs upon which they are based.[11][9][19][22] Methods may incorporate or be based on traditional medicinal practices of a particular culture, folk knowledge, superstition,[66] spiritual beliefs, belief in supernatural energies (antiscience), pseudoscience, errors in reasoning, propaganda, fraud, new or different concepts of health and disease, and any bases other than being proven by scientific methods.[11][9][13][19] Different cultures may have their own unique traditional or belief based practices developed recently or over thousands of years, and specific practices or entire systems of practices. Unscientific belief systems "They told me if I took 1000 pills at night I should be quite another thing in the morning", an early 19th-century satire on Morison's Vegetable Pills, an alternative medicine supplement Alternative medicine, such as using naturopathy or homeopathy in place of conventional medicine, is based on belief systems not grounded in science.[22] |
代替医療の種類 関連項目: 代替医療の形態一覧 代替医療は、幅広い健康に関する行為、製品、療法から成る。共通点は、科学的根拠に基づかない治療効果を主張することだ。代替医療の実践は、その基盤や方 法論において多様である。[22] 代替医療の実践は、文化的起源や、その基盤となる信念の種類によって分類されることがある。[11][9][19][22] その手法は、特定の文化における伝統的な医療行為、民間知識、迷信[66]、精神的信念、超自然的なエネルギーへの信仰(反科学)、疑似科学、推論の誤 り、プロパガンダ、詐欺、健康と疾病に関する新たな概念や異なる概念、そして科学的方法によって証明されたもの以外のあらゆる根拠を取り入れたり、それら に基づいたりすることがある。[11][9][13][19] 異なる文化圏には、近年または数千年にわたり発展した独自の伝統的・信念に基づく実践、特定の施術法、あるいは施術体系全体が存在する。 非科学的な信念体系 「夜に1000錠飲めば朝にはすっかり別人のようになる」と彼らは言った──19世紀初頭の風刺文。モリソンの野菜錠剤(代替医療サプリメント)を揶揄し たもの 代替医療(例:自然療法やホメオパシーを従来の医療に代えて使用すること)は、科学に根ざさない信念体系に基づいている。[22] |
Traditional ethnic systems Ready-to-drink traditional Chinese medicine mixture  Acupuncture involves insertion of needles in the body. Alternative medical systems may be based on traditional medicine practices, such as traditional Chinese medicine (TCM), Ayurveda in India, or practices of other cultures around the world.[22] Some useful applications of traditional medicines have been researched and accepted within ordinary medicine, however the underlying belief systems are seldom scientific and are not accepted. Traditional medicine is considered alternative when it is used outside its home region; or when it is used together with or instead of known functional treatment; or when it can be reasonably expected that the patient or practitioner knows or should know that it will not work – such as knowing that the practice is based on superstition. |
伝統的な民族医療体系 飲用可能な漢方薬調合液 鍼治療は体に針を刺す行為である。 代替医療体系は、漢方医学(TCM)、インドのアーユルヴェーダ、あるいは世界各国の伝統医療実践に基づく場合がある[22]。伝統医療の有用な応用例は 一般医学内で研究・採用されているが、その根底にある信念体系は科学的根拠が乏しく、医学界で認められることは稀である。 伝統医療は、以下の場合に代替医療と見なされる:1. 発祥地域外で使用される場合2. 既知の有効な治療法と併用される、またはそれに代わる場合3. 患者や施術者がその効果が期待できないと知り、あるいは知るべき状況にある場合(例:その実践が迷信に基づいていると認識している場合) |
| Supernatural energies Bases of belief may include belief in existence of supernatural energies undetected by the science of physics, as in biofields, or in belief in properties of the energies of physics that are inconsistent with the laws of physics, as in energy medicine.[22] |
超自然的なエネルギー 信仰の基盤には、物理学の科学では検出されない超自然的なエネルギーの存在を信じるもの(例:生体エネルギー)や、物理学の法則と矛盾する物理エネルギーの性質を信じるもの(例:エネルギー医学)が含まれることがある。[22] |
| Herbal remedies and other substances Main article: Herbal medicine Substance based practices use substances found in nature such as herbs, foods, non-vitamin supplements and megavitamins, animal and fungal products, and minerals, including use of these products in traditional medical practices that may also incorporate other methods.[22][92][93] Examples include healing claims for non-vitamin supplements, fish oil, Omega-3 fatty acid, glucosamine, echinacea, flaxseed oil, and ginseng.[94] Herbal medicine, or phytotherapy, includes not just the use of plant products, but may also include the use of animal and mineral products.[92] It is among the most commercially successful branches of alternative medicine, and includes the tablets, powders and elixirs that are sold as "nutritional supplements".[92] Only a very small percentage of these have been shown to have any efficacy, and there is little regulation as to standards and safety of their contents.[92] |
ハーブ療法およびその他の物質 主な記事: ハーブ療法 物質に基づく療法は、ハーブ、食品、非ビタミン系サプリメントやメガビタミン、動物性・菌類由来製品、鉱物など自然界に存在する物質を用いる。これらは伝 統医療において他の手法と組み合わせて使用される場合もある。[22][92][93] 例としては、非ビタミン系サプリメント、魚油、オメガ3脂肪酸、グルコサミン、エキナセア、亜麻仁油、高麗人参に対する治療効果の主張がある。[94] ハーブ療法(フィトセラピー)は、植物製品の使用だけでなく、動物性・鉱物性製品の使用も含む場合がある。[92] これは代替医療の中でも商業的に最も成功している分野の一つであり、「栄養補助食品」として販売される錠剤、粉末、エリキシル剤などを含む。[92] これらの中で有効性が実証されているものはごく一部であり、内容物の基準や安全性に関する規制はほとんど存在しない。[92] |
| Religion, faith healing, and prayer See also: Shamanism |
宗教、信仰による癒し、そして祈り 関連項目:シャーマニズム |
 A chiropractor "adjusting" the spine |
カイロプラクターが背骨を「調整」している |
| NCCIH classification The United States agency National Center for Complementary and Integrative Health (NCCIH) has created a classification system for branches of complementary and alternative medicine that divides them into five major groups. These groups have some overlap, and distinguish two types of energy medicine: veritable which involves scientifically observable energy (including magnet therapy, colorpuncture and light therapy) and putative, which invokes physically undetectable or unverifiable energy.[98] None of these energies have any evidence to support that they affect the body in any positive or health promoting way.[1] 1. Whole medical systems: Cut across more than one of the other groups; examples include traditional Chinese medicine, naturopathy, homeopathy, and ayurveda. 2. Mind-body interventions: Explore the interconnection between the mind, body, and spirit, under the premise that they affect "bodily functions and symptoms". A connection between mind and body is conventional medical fact, and this classification does not include therapies with proven function such as cognitive behavioral therapy. 3. "Biology"-based practices: Use substances found in nature such as herbs, foods, vitamins, and other natural substances. (As used here, "biology" does not refer to the science of biology, but is a usage newly coined by NCCIH in the primary source used for this article. "Biology-based" as coined by NCCIH may refer to chemicals from a nonbiological source, such as use of the poison lead in traditional Chinese medicine, and to other nonbiological substances.) 4. Manipulative and body-based practices: feature manipulation or movement of body parts, such as is done in bodywork, chiropractic, and osteopathic manipulation. 5. Energy medicine: is a domain that deals with putative and verifiable energy fields: ・Biofield therapies are intended to influence energy fields that are purported to surround and penetrate the body. The existence of such energy fields have been disproven. ・Bioelectromagnetic-based therapies use verifiable electromagnetic fields, such as pulsed fields, alternating-current, or direct-current fields in a non-scientific manner. |
NCCIH分類 米国政府機関である国立補完統合医療センター(NCCIH)は、補完代替医療の分野を5つの主要グループに分類する体系を構築した。これらのグループには 一部重複があり、エネルギー医学を2種類に区別している。一つは科学的に観測可能なエネルギー(磁気療法、カラーパンクチャー、光療法を含む)を扱う「実 在型」、もう一つは物理的に検出不能または検証不能なエネルギーを扱う「仮説型」である[98]。いずれのエネルギーも、身体に何らかの有益な影響や健康 増進効果をもたらすことを裏付ける証拠は存在しない[1]。 1. 総合医療体系:他の複数のグループにまたがる。例として、伝統中国医学、自然療法、ホメオパシー、アーユルヴェーダがある。 2. 心身介入療法:心、身体、精神の相互関係を探求し、「身体機能や症状」に影響を与えるという前提のもとで行われる。心と身体の関連性は従来の医学的事実であり、認知行動療法など効果が証明されている療法はこの分類に含まれない。 3. 「生物学」に基づく実践:ハーブ、食品、ビタミン、その他の天然物質など、自然界に存在する物質を用いる。(ここでいう「生物学」は生物学の科学を指すの ではなく、本記事の主要情報源であるNCCIHが新たに造語した用法である。NCCIHが提唱する「生物学ベース」は、中国伝統医学における鉛毒の使用な ど非生物学的起源の化学物質や、その他の非生物学的物質を指す場合もある。) 4. 操作・身体ベース療法:身体部位の操作や移動を特徴とする。ボディワーク、カイロプラクティック、オステオパシー操作などが該当する。 5. エネルギー医療:実在が主張され検証可能なエネルギー場を扱う領域である: ・バイオフィールド療法は、身体を取り囲み浸透するとされるエネルギー場に影響を与えることを目的とする。このようなエネルギー場の存在は否定されている。 ・生体電磁気ベース療法は、パルス電磁場、交流電磁場、直流電磁場など検証可能な電磁場を非科学的な方法で使用する。 |
| History Main article: History of alternative medicine The history of alternative medicine may refer to the history of a group of diverse medical practices that were collectively promoted as "alternative medicine" beginning in the 1970s, to the collection of individual histories of members of that group, or to the history of western medical practices that were labeled "irregular practices" by the western medical establishment.[9][99][100][101][102] It includes the histories of complementary medicine and of integrative medicine. Before the 1970s, western practitioners that were not part of the increasingly science-based medical establishment were referred to "irregular practitioners", and were dismissed by the medical establishment as unscientific and as practicing quackery.[99][100] Until the 1970s, irregular practice became increasingly marginalized as quackery and fraud, as western medicine increasingly incorporated scientific methods and discoveries, and had a corresponding increase in success of its treatments.[102] In the 1970s, irregular practices were grouped with traditional practices of nonwestern cultures and with other unproven or disproven practices that were not part of biomedicine, with the entire group collectively marketed and promoted under the single expression "alternative medicine".[9][99][100][102][103] Use of alternative medicine in the west began to rise following the counterculture movement of the 1960s, as part of the rising new age movement of the 1970s.[9][104][105] This was due to misleading mass marketing of "alternative medicine" being an effective "alternative" to biomedicine, changing social attitudes about not using chemicals and challenging the establishment and authority of any kind, sensitivity to giving equal measure to beliefs and practices of other cultures (cultural relativism), and growing frustration and desperation by patients about limitations and side effects of science-based medicine.[9][100][102][101][103][105][106] At the same time, in 1975, the American Medical Association, which played the central role in fighting quackery in the United States, abolished its quackery committee and closed down its Department of Investigation.[99]: xxi [106] By the early to mid 1970s the expression "alternative medicine" came into widespread use, and the expression became mass marketed as a collection of "natural" and effective treatment "alternatives" to science-based biomedicine.[9][106][107][108] By 1983, mass marketing of "alternative medicine" was so pervasive that the British Medical Journal (BMJ) pointed to "an apparently endless stream of books, articles, and radio and television programmes urge on the public the virtues of (alternative medicine) treatments ranging from meditation to drilling a hole in the skull to let in more oxygen".[106] An analysis of trends in the criticism of complementary and alternative medicine (CAM) in five prestigious American medical journals during the period of reorganization within medicine (1965–1999) was reported as showing that the medical profession had responded to the growth of CAM in three phases, and that in each phase, changes in the medical marketplace had influenced the type of response in the journals.[109] Changes included relaxed medical licensing, the development of managed care, rising consumerism, and the establishment of the USA Office of Alternative Medicine (later National Center for Complementary and Alternative Medicine, currently National Center for Complementary and Integrative Health).[n 9] |
歴史 主な記事: 代替医療の歴史 代替医療の歴史とは、1970年代から「代替医療」として一括りに推進されてきた多様な医療行為群の歴史を指す場合もあれば、その構成要素となる個々の医 療行為の歴史を指す場合もある。あるいは西洋医学の権威によって「非正規医療」とレッテルを貼られた西洋医療行為の歴史を指す場合もある。[9][99] [100][101][102] これには補完医療と統合医療の歴史も含まれる。1970年代以前、科学に基づく医療体制に属さない西洋医療従事者は「非正規医療従事者」と呼ばれ、医療体 制から非科学的であり、偽医療を実践していると軽蔑されていた。[99][100] 1970年代まで、西洋医学が科学的技法や発見を次第に取り入れ、治療の成功率が相応に高まるにつれ、非正規医療は偽医療や詐欺としてますます周縁化され ていった。[102] 1970年代には、非正規医療は非西洋文化の伝統的医療や、生物医学に属さない他の未検証・反証された医療と一括りにされ、これら全体が「代替医療」とい う単一の表現で総称され、マーケティングや宣伝が行われるようになった。[9][99][100][102][103] 西洋における代替医療の利用は、1960年代のカウンターカルチャー運動に続き、1970年代に台頭したニューエイジ運動の一環として増加し始めた。 [9][104] [105] これは主に以下の要因による:- 「代替医療」が生物医学に代わる有効な選択肢であるという誤解を招く大衆向けマーケティング- 化学物質を使用しないという社会的態度の変化とあらゆる権威への挑戦- 他文化の信念や実践を平等に扱うべきだという感覚(文化的相対主義)- 科学に基づく医療の限界や副作用に対する患者の不満と絶望感の高まり[9] [100][102][101][103][105][106] 同時に1975年、米国における偽医療対策の中核的役割を担ってきた米国医師会(AMA)は、偽医療対策委員会を廃止し調査部門を閉鎖した。[99]: xxi [106] 1970年代前半から中盤にかけて、「代替医療」という表現が広く使われるようになり、科学に基づく生物医学への「自然」で効果的な治療法の「代替」とし て大衆向けに売り出されるようになった。[9] [106][107][108] 1983年までに「代替医療」の大衆向けマーケティングは極めて広範となり、英国医学雑誌(BMJ)は「瞑想から頭蓋骨に穴を開けて酸素を取り込む治療法 に至るまで、(代替医療の)効能を一般に推奨する書籍、記事、ラジオ・テレビ番組が絶え間なく流れ続けている」と指摘した。[106] 医学界の再編期(1965-1999年)における5つの権威ある米国医学雑誌での補完代替医療(CAM)批判の傾向分析は、医療専門職がCAMの成長に三 段階で対応したことを示した。各段階において、医療市場の変化が雑誌上の対応の性質に影響を与えていた。[109] 変化には、医師免許の緩和、マネージドケアの発展、消費者主義の高まり、米国代替医療局(後に国立補完代替医療センター、現在は国立補完統合医療セン ター)の設立が含まれた。[n 9] |
| Medical education Mainly as a result of reforms following the Flexner Report of 1910[111] medical education in established medical schools in the US has generally not included alternative medicine as a teaching topic.[n 10] Typically, their teaching is based on current practice and scientific knowledge about: anatomy, physiology, histology, embryology, neuroanatomy, pathology, pharmacology, microbiology and immunology.[113] Medical schools' teaching includes such topics as doctor-patient communication, ethics, the art of medicine,[114] and engaging in complex clinical reasoning (medical decision-making).[115] Writing in 2002, Snyderman and Weil remarked that by the early twentieth century the Flexner model had helped to create the 20th-century academic health center, in which education, research, and practice were inseparable. While this had much improved medical practice by defining with increasing certainty the pathophysiological basis of disease, a single-minded focus on the pathophysiological had diverted much of mainstream American medicine from clinical conditions that were not well understood in mechanistic terms, and were not effectively treated by conventional therapies.[116] By 2001 some form of CAM training was being offered by at least 75 out of 125 medical schools in the US.[117] Exceptionally, the School of Medicine of the University of Maryland, Baltimore, includes a research institute for integrative medicine (a member entity of the Cochrane Collaboration).[118][119] Medical schools are responsible for conferring medical degrees, but a physician typically may not legally practice medicine until licensed by the local government authority. Licensed physicians in the US who have attended one of the established medical schools there have usually graduated Doctor of Medicine (MD).[120] All states require that applicants for MD licensure be graduates of an approved medical school and complete the United States Medical Licensing Examination (USMLE).[120] |
医学教育 主に1910年のフレックスナー報告書[111]に続く改革の結果として、米国の既存医学部における医学教育は、代替医療を教育テーマとして含めてこな かった。通常、その教育内容は解剖学、生理学、組織学、発生学、神経解剖学、病理学、薬理学、微生物学、免疫学といった、現行の診療と科学的知見に基づい ている。[113] 医学部の教育には、医師と患者のコミュニケーション、倫理、医療の技術[114]、複雑な臨床推論(医療意思決定)の遂行[115]といった主題も含まれ る。2002年に執筆したスナイダーマンとウェイルは、20世紀初頭までにフレックスナー・モデルが教育、研究、実践が不可分な20世紀の学術医療セン ター創出に寄与したと指摘した。これは疾患の病態生理学的基盤を確固たるものとして定義することで医療実践を大きく改善したが、病態生理学への偏重は、メ カニズム的に十分に理解されておらず、従来の治療法では効果的に対処できなかった臨床症状から、主流のアメリカ医学の多くを遠ざける結果となった [116]。 2001年までに、米国の125の医学部のうち少なくとも75校が何らかの形で補完代替医療(CAM)の研修を提供していた[117]。特筆すべきは、メ リーランド大学ボルチモア校医学部が統合医療研究所(コクラン・コラボレーションの加盟機関)を設置している点である[118][119]。医学部は医学 学位を授与する責任を負うが、医師は通常、地方政府当局から免許を取得するまで合法的に医療行為を行えない。米国の認可医学校を卒業した免許取得医師は、 通常医学博士(MD)の学位を取得している。[120] 全州において、MD免許申請者は認可医学校の卒業生であり、米国医師免許試験(USMLE)を修了していることが要求される。[120] |
| Efficacy Edzard Ernst, an authority on scientific study of alternative therapies and diagnoses and the first university professor of CAM, in 2012 There is a general scientific consensus that alternative therapies lack the requisite scientific validation, and their effectiveness is either unproved or disproved.[11][9][121][122] Many of the claims regarding the efficacy of alternative medicines are controversial, since research on them is frequently of low quality and methodologically flawed.[123] Selective publication bias, marked differences in product quality and standardisation, and some companies making unsubstantiated claims call into question the claims of efficacy of isolated examples where there is evidence for alternative therapies.[124] The Scientific Review of Alternative Medicine points to confusions in the general population – a person may attribute symptomatic relief to an otherwise-ineffective therapy just because they are taking something (the placebo effect); the natural recovery from or the cyclical nature of an illness (the regression fallacy) gets misattributed to an alternative medicine being taken; a person not diagnosed with science-based medicine may never originally have had a true illness diagnosed as an alternative disease category.[125] Edzard Ernst, the first university professor of Complementary and Alternative Medicine, characterized the evidence for many alternative techniques as weak, nonexistent, or negative[126] and in 2011 published his estimate that about 7.4% were based on "sound evidence", although he believes that may be an overestimate.[127] Ernst has concluded that 95% of the alternative therapies he and his team studied, including acupuncture, herbal medicine, homeopathy, and reflexology, are "statistically indistinguishable from placebo treatments", but he also believes there is something that conventional doctors can usefully learn from the chiropractors and homeopath: this is the therapeutic value of the placebo effect, one of the strangest phenomena in medicine.[128][129] In 2003, a project funded by the CDC identified 208 condition-treatment pairs, of which 58% had been studied by at least one randomized controlled trial (RCT), and 23% had been assessed with a meta-analysis.[130] According to a 2005 book by a US Institute of Medicine panel, the number of RCTs focused on CAM has risen dramatically. As of 2005, the Cochrane Library had 145 CAM-related Cochrane systematic reviews and 340 non-Cochrane systematic reviews. An analysis of the conclusions of only the 145 Cochrane reviews was done by two readers. In 83% of the cases, the readers agreed. In the 17% in which they disagreed, a third reader agreed with one of the initial readers to set a rating. These studies found that, for CAM, 38.4% concluded positive effect or possibly positive (12.4%), 4.8% concluded no effect, 0.7% concluded harmful effect, and 56.6% concluded insufficient evidence. An assessment of conventional treatments found that 41.3% concluded positive or possibly positive effect, 20% concluded no effect, 8.1% concluded net harmful effects, and 21.3% concluded insufficient evidence. However, the CAM review used the more developed 2004 Cochrane database, while the conventional review used the initial 1998 Cochrane database.[131] Alternative therapies do not "complement" (improve the effect of, or mitigate the side effects of) functional medical treatment.[n 7][11][26][27][28] Significant drug interactions caused by alternative therapies may instead negatively impact functional treatment by making prescription drugs less effective, such as interference by herbal preparations with warfarin.[132][33] In the same way as for conventional therapies, drugs, and interventions, it can be difficult to test the efficacy of alternative medicine in clinical trials. In instances where an established, effective, treatment for a condition is already available, the Helsinki Declaration states that withholding such treatment is unethical in most circumstances. Use of standard-of-care treatment in addition to an alternative technique being tested may produce confounded or difficult-to-interpret results.[133] Cancer researcher Andrew J. Vickers has stated: Contrary to much popular and scientific writing, many alternative cancer treatments have been investigated in good-quality clinical trials, and they have been shown to be ineffective. The label "unproven" is inappropriate for such therapies; it is time to assert that many alternative cancer therapies have been "disproven".[134] |
有効性 代替療法と診断の科学的研究における権威であり、CAM(補完代替医療)の最初の大学教授であるエドザード・エルンストは、2012年に次のように述べている 代替療法には必要な科学的検証が欠けており、その有効性は証明されていないか、あるいは反証されているというのが、科学界の一般的な合意である。代替医療 の有効性に関する主張の多くは論争の的となっている。なぜなら、それらに関する研究は質が低く方法論的に欠陥がある場合が多いからだ。選択的出版バイア ス、製品品質と標準化における顕著な差異、根拠のない主張を行う企業などにより、代替療法に証拠がある孤立した事例の有効性主張は疑問視されている。 代替医療の科学的レビューは、一般市民における混乱を指摘している。例えば、症状の緩和を、単に何かを服用しているという理由だけで(プラセボ効果)、本 来は効果のない療法に帰属させることがある。病気の自然治癒や周期的な性質(回帰の誤謬)が、代替医療の服用によるものと誤って帰属されることもある。科 学に基づく医療で診断されていない人は、そもそも代替医療の疾患カテゴリーとして診断されるような真の病気を持っていなかった可能性がある。[125] 補完代替医療の初代大学教授であるエザード・エルンストは、多くの代替療法の証拠を「弱い」「存在しない」「否定的なもの」と特徴づけ[126]、 2011年には約7.4%が「確かな証拠」に基づくと推定したが、これは過大評価かもしれないとも述べている[127]。エルンストは、自身と研究チーム が調査した代替療法(鍼治療、漢方薬、ホメオパシー、リフレクソロジーを含む)の95%が「プラセボ治療と統計的に区別できない」と結論づけた。しかし同 時に、カイロプラクターやホメオパスから現代医師が学ぶべき点があると指摘している。それはプラセボ効果の治療的価値であり、医学上最も奇妙な現象の一つ である[128][129]。 2003年、CDCが資金提供したプロジェクトでは208の疾患-治療ペアを特定し、そのうち58%が少なくとも1つのランダム化比較試験(RCT)で研 究され、23%がメタ分析で評価されていた。[130] 米国医学研究所パネルによる2005年の書籍によれば、CAMに焦点を当てたRCTの数は劇的に増加している。 2005年時点で、コクラン・ライブラリーには145件のCAM関連コクラン系統的レビューと340件の非コクラン系統的レビューが収録されていた。2名 の読者が、この145件のコクランレビューの結論のみを分析した。83%のケースで読者の見解は一致した。17%の意見不一致事例では、第三の読者が当初 の読者のいずれか一方の見解に同意し評価を確定した。これらの研究では、CAMについて38.4%が「肯定的効果」または「おそらく肯定的効果」と結論付 け、4.8%が「効果なし」、0.7%が「有害効果」、56.6%が「証拠不十分」と結論付けた。従来療法の評価では、41.3%が肯定的またはおそらく 肯定的効果、20%が効果なし、8.1%が純粋な有害効果、21.3%が証拠不十分と結論づけた。ただし代替医療のレビューではより発展した2004年版 コクラン・データベースを使用し、従来療法のレビューでは初期の1998年版コクラン・データベースを使用した。[131] 代替療法は機能的医療治療を「補完」(効果を高めたり副作用を軽減したり)しない。[n 7][11][26][27][28] むしろ代替療法による重大な薬物相互作用は、処方薬の効果を低下させることで機能的治療に悪影響を及ぼす可能性がある。例えばハーブ製剤がワルファリンに 干渉する事例が挙げられる。[132][33] 従来の治療法、薬物、介入と同様に、代替医療の有効性を臨床試験で検証することは難しい場合がある。ある疾患に対して確立された効果的な治療法がすでに利 用可能な場合、ヘルシンキ宣言は、そのような治療を差し控えることは、ほとんどの場合、非倫理的であると述べている。検証中の代替療法に加えて標準治療を 使用すると、結果が混乱したり、解釈が困難になったりする可能性がある。[133] がん研究者のアンドルー・J・ヴィッカースは次のように述べている。 多くの大衆向けや科学的な文献とは対照的に、多くの代替がん治療は質の高い臨床試験で調査されており、その効果がないことが証明されている。「未証明」と いうレッテルは、こうした治療法には不適切である。多くの代替がん治療は「反証された」と断言すべき時が来ている。[134] |
| Perceived mechanism of effect Anything classified as alternative medicine by definition does not have a proven healing or medical effect.[2][9][13][14][15] However, there are different mechanisms through which it can be perceived to "work". The common denominator of these mechanisms is that effects are mis-attributed to the alternative treatment. 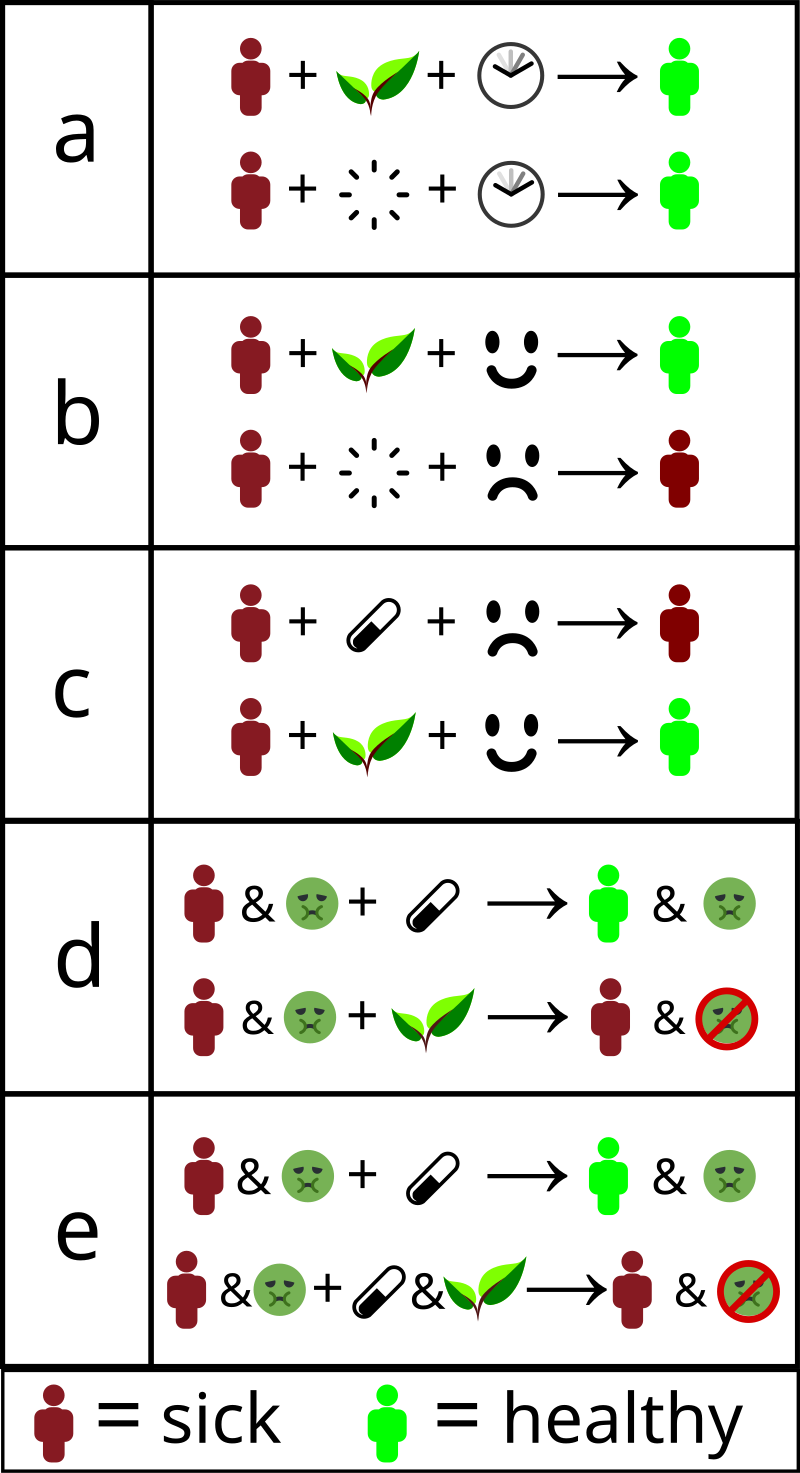 How alternative therapies "work": a) Misinterpreted natural course – the individual gets better without treatment. b) Placebo effect or false treatment effect – an individual receives "alternative therapy" and is convinced it will help. The conviction makes them more likely to get better. c) Nocebo effect – an individual is convinced that standard treatment will not work, and that alternative therapies will work. This decreases the likelihood standard treatment will work, while the placebo effect of the "alternative" remains. d) No adverse effects – Standard treatment is replaced with "alternative" treatment, getting rid of adverse effects, but also of improvement. e) Interference – Standard treatment is "complemented" with something that interferes with its effect. This can both cause worse effect, but also decreased (or even increased) side effects, which may be interpreted as "helping". Researchers, such as epidemiologists, clinical statisticians and pharmacologists, use clinical trials to reveal such effects, allowing physicians to offer a therapeutic solution best known to work. "Alternative treatments" often refuse to use trials or make it deliberately hard to do so. Placebo effect A placebo is a treatment with no intended therapeutic value. An example of a placebo is an inert pill, but it can include more dramatic interventions like sham surgery. The placebo effect is the concept that patients will perceive an improvement after being treated with an inert treatment. The opposite of the placebo effect is the nocebo effect, when patients who expect a treatment to be harmful will perceive harmful effects after taking it. Placebos do not have a physical effect on diseases or improve overall outcomes, but patients may report improvements in subjective outcomes such as pain and nausea.[135] A 1955 study suggested that a substantial part of a medicine's impact was due to the placebo effect.[136][135] However, reassessments found the study to have flawed methodology.[136][137] This and other modern reviews suggest that other factors like natural recovery and reporting bias should also be considered.[135][137] All of these are reasons why alternative therapies may be credited for improving a patient's condition even though the objective effect is non-existent, or even harmful.[132][40][64] David Gorski argues that alternative treatments should be treated as a placebo, rather than as medicine.[40] Almost none have performed significantly better than a placebo in clinical trials.[76][63][138][92] Furthermore, distrust of conventional medicine may lead to patients experiencing the nocebo effect when taking effective medication.[132] |
効果の認識されるメカニズム 代替医療と定義されるものは、その定義上、証明された治療効果や医学的効果を持たない。[2][9][13][14][15] しかし、それらが「効く」と認識されるメカニズムは様々である。これらのメカニズムに共通するのは、効果が代替療法に誤って帰属される点だ。 代替療法が「効く」とされる仕組み: a) 自然経過の誤解 – 治療を受けなくても個人が回復する。 b) プラセボ効果または偽治療効果 – 個人が「代替療法」を受け、それが効くと確信する。その確信が回復の可能性を高める。 c) ノセボ効果 – 標準治療は効かず代替療法が効くと個人が確信する。これにより標準治療の効果が低下する一方、「代替」療法のプラセボ効果は持続する。 d) 副作用の排除 – 標準治療を「代替」療法に置き換えることで副作用はなくなるが、同時に改善効果も失われる。 e) 干渉効果 – 標準治療にその効果を妨げるものが「補完」される。これにより効果が悪化する一方、副作用が減る(あるいは増える)こともあり、これが「効果がある」と解 釈されることがある。疫学者、臨床統計学者、薬理学者などの研究者は、臨床試験を通じてこうした効果を明らかにし、医師が最も効果があると知られている治 療法を提供できるようにしている。「代替療法」はしばしば試験の実施を拒否するか、意図的に困難にする。 プラセボ効果 プラセボとは、治療的価値を持たない治療法である。無効な錠剤がその例だが、偽手術のような劇的な介入も含む。プラセボ効果とは、無効な治療を受けた患者 が改善を実感するという概念である。プラセボ効果の反対はノセボ効果であり、治療が有害であると予期する患者が、治療後に有害な効果を実感する現象を指 す。 プラセボは疾患に物理的な効果をもたらさず、全体的な治療成績を改善しない。しかし患者は痛みや吐き気といった主観的症状の改善を報告することがある [135]。1955年の研究では、薬効の相当部分がプラセボ効果によるものだと示唆された。[136][135] しかし再評価により、この研究には方法論上の欠陥があったことが判明した。[136][137] この研究や他の現代的なレビューは、自然回復や報告バイアスなどの他の要因も考慮すべきだと示唆している。[135][137] これら全てが、代替療法が客観的な効果が存在しない、あるいは有害であるにもかかわらず、患者の状態改善に寄与していると評価される理由である。 [132][40][64] デイビッド・ゴーシキは、代替療法は医療ではなくプラセボとして扱うべきだと主張している。[40] 臨床試験においてプラセボより有意に優れた効果を示したものはほとんどない。[76][63][138][92] さらに、従来の医療への不信感は、有効な薬を服用する患者にノセボ効果を引き起こす可能性がある。[132] |
| Regression to the mean A patient who receives an inert treatment may report improvements afterwards that it did not cause.[135][137] Assuming it was the cause without evidence is an example of the regression fallacy. This may be due to a natural recovery from the illness, or a fluctuation in the symptoms of a long-term condition.[137] The concept of regression toward the mean implies that an extreme result is more likely to be followed by a less extreme result. |
平均への回帰 無効な治療を受けた患者は、その治療が原因ではないにもかかわらず、後に改善を報告することがある。[135][137] 証拠なしにそれが原因だと仮定するのは回帰の誤謬の一例である。これは病気からの自然回復、あるいは慢性疾患の症状の変動による可能性がある。[137] 平均への回帰という概念は、極端な結果の後に、より極端でない結果が続く可能性が高いことを示唆している。 |
| Other factors There are also reasons why a placebo treatment group may outperform a "no-treatment" group in a test which are not related to a patient's experience. These include patients reporting more favourable results than they really felt due to politeness or "experimental subordination", observer bias, and misleading wording of questions.[137] In their 2010 systematic review of studies into placebos, Asbjørn Hróbjartsson and Peter C. Gøtzsche write that "even if there were no true effect of placebo, one would expect to record differences between placebo and no-treatment groups due to bias associated with lack of blinding."[135] Alternative therapies may also be credited for perceived improvement through decreased use or effect of medical treatment, and therefore either decreased side effects or nocebo effects towards standard treatment.[132] |
その他の要因 試験においてプラセボ治療群が「無治療」群を上回る結果を示す理由は、患者の体験とは無関係なものもある。これには、礼儀や「実験的従属」による実際の感 覚よりも良好な結果を報告する患者、観察者バイアス、誤解を招く質問の表現などが含まれる。[137] 2010年のプラセボ研究の系統的レビューにおいて、アスビョルン・フロビャルトソンとピーター・C・ゲッツェは「仮にプラセボに真の効果がない場合で も、盲検化不足に伴うバイアスにより、プラセボ群と無治療群の間に差異が記録されることが予想される」と記している。[135] 代替療法は、医療処置の使用量や効果の減少を通じて知覚された改善の要因とみなされることもあり、その結果、標準治療に対する副作用の減少またはノセボ効 果が生じる可能性がある。[132] |
| Use and regulation Appeal Practitioners of complementary medicine usually discuss and advise patients as to available alternative therapies. Patients often express interest in mind-body complementary therapies because they offer a non-drug approach to treating some health conditions.[139] In addition to the social-cultural underpinnings of the popularity of alternative medicine, there are several psychological issues that are critical to its growth, notably psychological effects, such as the will to believe,[140] cognitive biases that help maintain self-esteem and promote harmonious social functioning,[140] and the post hoc, ergo propter hoc fallacy.[140] In a 2018 interview with The BMJ, Edzard Ernst stated: "The present popularity of complementary and alternative medicine is also inviting criticism of what we are doing in mainstream medicine. It shows that we aren't fulfilling a certain need-we are not giving patients enough time, compassion, or empathy. These are things that complementary practitioners are very good at. Mainstream medicine could learn something from complementary medicine."[141] Marketing Alternative medicine is a profitable industry with large media advertising expenditures. Accordingly, alternative practices are often portrayed positively and compared favorably to "big pharma".[1] The popularity of complementary & alternative medicine (CAM) may be related to other factors that Ernst mentioned in a 2008 interview in The Independent: Why is it so popular, then? Ernst blames the providers, customers and the doctors whose neglect, he says, has created the opening into which alternative therapists have stepped. "People are told lies. There are 40 million websites and 39.9 million tell lies, sometimes outrageous lies. They mislead cancer patients, who are encouraged not only to pay their last penny but to be treated with something that shortens their lives." At the same time, people are gullible. It needs gullibility for the industry to succeed. It doesn't make me popular with the public, but it's the truth.[142] Paul Offit proposed that "alternative medicine becomes quackery" in four ways: by recommending against conventional therapies that are helpful, promoting potentially harmful therapies without adequate warning, draining patients' bank accounts, or by promoting "magical thinking".[58] Promoting alternative medicine has been called dangerous and unethical.[n 11][144]  Friendly and colorful images of herbal treatments may look less threatening or dangerous when compared to conventional medicine. This is an intentional marketing strategy.[145][146] Social factors Authors have speculated on the socio-cultural and psychological reasons for the appeal of alternative medicines among the minority using them in lieu of conventional medicine. There are several socio-cultural reasons for the interest in these treatments centered on the low level of scientific literacy among the public at large and a concomitant increase in antiscientific attitudes and new age mysticism.[140] Related to this are vigorous marketing[147] of extravagant claims by the alternative medical community combined with inadequate media scrutiny and attacks on critics.[140][148] Alternative medicine is criticized for taking advantage of the least fortunate members of society.[1] There is also an increase in conspiracy theories toward conventional medicine and pharmaceutical companies,[34] mistrust of traditional authority figures, such as the physician, and a dislike of the current delivery methods of scientific biomedicine, all of which have led patients to seek out alternative medicine to treat a variety of ailments.[148] Many patients lack access to contemporary medicine, due to a lack of private or public health insurance, which leads them to seek out lower-cost alternative medicine.[149] Medical doctors are also aggressively marketing alternative medicine to profit from this market.[147] Patients can be averse to the painful, unpleasant, and sometimes-dangerous side effects of biomedical treatments. Treatments for severe diseases such as cancer and HIV infection have well-known, significant side-effects. Even low-risk medications such as antibiotics can have potential to cause life-threatening anaphylactic reactions in a very few individuals. Many medications may cause minor but bothersome symptoms such as cough or upset stomach. In all of these cases, patients may be seeking out alternative therapies to avoid the adverse effects of conventional treatments.[140][148] |
使用と規制 訴求力 補完医療の施術者は通常、利用可能な代替療法について患者と話し合い、助言する。患者はしばしば心身療法への関心を示す。なぜならそれらは特定の健康状態を治療する非薬物療法を提供するためだ。[139] 代替医療の普及には社会文化的背景に加え、その成長に重要な心理的要因がいくつか存在する。特に「信じたいという意志」[140]、自尊心の維持や調和的 な社会機能を促進する認知バイアス[140]、事後性誤謬(post hoc, ergo propter hoc)[140]といった心理的効果が挙げられる。 2018年のBMJ誌インタビューでエドザード・エルンストは次のように述べている:「補完代替医療の現在の人気は、主流医療の在り方への批判も招いてい る。これは我々が特定のニーズを満たせていないことを示している——患者に十分な時間、思いやり、共感を注いでいないのだ。これらは補完医療実践者が非常 に得意とする分野である。主流医療は補完医療から学ぶべき点がある」[141] マーケティング 代替医療は収益性の高い産業であり、メディア広告費も多額である。したがって、代替医療の実践はしばしば肯定的に描かれ、「大手製薬会社」と比べて好意的に比較される。[1] 補完代替医療(CAM)の人気は、アーンストが2008年のインディペンデント紙インタビューで言及した他の要因とも関連している可能性がある: ではなぜこれほど人気があるのか?アーンストは提供者、顧客、そして医師の怠慢が原因だと指摘する。その怠慢が隙間を生み、代替療法師が入り込む余地を 作ったのだと彼は言う。「人々は嘘を吹き込まれている。4000万のウェブサイトのうち3990万が嘘を流布し、時にはとんでもない嘘だ。癌患者を誤導 し、最後の1円まで払わせると同時に、寿命を縮める治療を受けさせるよう促している」。同時に人々は騙されやすい。この産業が成功するには騙されやすさが 必要だ。大衆に好かれる発言ではないが、これが真実だ。[142] ポール・オフィットは「代替医療がペテン師的行為となる」四つのパターンを提唱した:有益な従来療法を否定すること、十分な警告なしに有害な可能性のある 療法を推奨すること、患者の銀行口座を枯渇させること、あるいは「魔法的思考」を助長することである。[58] 代替医療の推進は危険かつ非倫理的と評されてきた。[n 11] [144] ハーブ療法の親しみやすくカラフルなイメージは、従来の医療と比較すると脅威や危険性が少なく見える。これは意図的なマーケティング戦略だ。[145][146] 社会的要因 著者らは、従来の医療の代わりに代替医療を利用する少数派におけるその魅力の背景にある社会文化的・心理的要因について推測している。こうした治療法への 関心には、一般大衆の科学的リテラシーの低さと、それに伴う反科学的態度やニューエイジ神秘主義の台頭を中心とした、いくつかの社会文化的理由がある。 [140] これに関連して、代替医療コミュニティによる誇大広告の積極的な展開[147]、不十分なメディアの検証、批判者への攻撃が挙げられる。[140] [148] 代替医療は社会の恵まれない層を搾取していると批判されている。[1] さらに、従来の医療や製薬企業に対する陰謀論の増加[34]、医師などの伝統的権威者への不信感、科学的バイオメディシンの現行提供方法への嫌悪感などが あり、これら全てが患者を様々な疾患の治療に代替医療を求めるように導いている。[148] 多くの患者は、民間・公的医療保険の不足により現代医療へのアクセスが制限され、低コストの代替医療を求めるようになる。[149] 医師もまた、この市場から利益を得るため、代替医療を積極的に販売している。[147] 患者は、生物医学的治療の痛みを伴う、不快で、時に危険な副作用を嫌うことがある。がんやHIV感染症などの重篤な疾患に対する治療法には、よく知られた 重大な副作用がある。抗生物質のような低リスクの薬剤でさえ、ごく少数の個人において生命を脅かすアナフィラキシー反応を引き起こす可能性がある。多くの 薬剤は、咳や胃の不快感といった軽度だが煩わしい症状を引き起こすことがある。こうした全てのケースにおいて、患者は従来の治療法の有害な副作用を避ける ために代替療法を求めることがある。[140][148] |
| Prevalence of use According to research published in 2015, the increasing popularity of CAM needs to be explained by moral convictions or lifestyle choices rather than by economic reasoning.[150] In developing nations, access to essential medicines is severely restricted by lack of resources and poverty. Traditional remedies, often closely resembling or forming the basis for alternative remedies, may comprise primary healthcare or be integrated into the healthcare system. In Africa, traditional medicine is used for 80% of primary healthcare, and in developing nations as a whole over one-third of the population lack access to essential medicines.[151] In Latin America, inequities against BIPOC communities keep them tied to their traditional practices and therefore, it is often these communities that constitute the majority of users of alternative medicine. Racist attitudes towards certain communities disable them from accessing more urbanized modes of care. In a study that assessed access to care in rural communities of Latin America, it was found that discrimination is a huge barrier to the ability of citizens to access care; more specifically, women of Indigenous and African descent, and lower-income families were especially hurt.[152] Such exclusion exacerbates the inequities that minorities in Latin America already face. Consistently excluded from many systems of westernized care for socioeconomic and other reasons, low-income communities of color often turn to traditional medicine for care as it has proved reliable to them across generations. Commentators including David Horrobin have proposed adopting a prize system to reward medical research.[153] This stands in opposition to the current mechanism for funding research proposals in most countries around the world. In the US, the NCCIH provides public research funding for alternative medicine. The NCCIH has spent more than US$2.5 billion on such research since 1992 and this research has not demonstrated the efficacy of alternative therapies.[138][154][155][156][157][158] As of 2011, the NCCIH's sister organization in the NIC Office of Cancer Complementary and Alternative Medicine had given out grants of around $105 million each year for several years.[159] Testing alternative medicine that has no scientific basis (as in the aforementioned grants) has been called a waste of scarce research resources.[160][161] That alternative medicine has been on the rise "in countries where Western science and scientific method generally are accepted as the major foundations for healthcare, and 'evidence-based' practice is the dominant paradigm" was described as an "enigma" in the Medical Journal of Australia.[162] A 15-year systematic review published in 2022 on the global acceptance and use of CAM among medical specialists found the overall acceptance of CAM at 52% and the overall use at 45%.[163] In the United States In the United States, the 1974 Child Abuse Prevention and Treatment Act (CAPTA) required that for states to receive federal money, they had to grant religious exemptions to child neglect and abuse laws regarding religion-based healing practices.[164] Thirty-one states have child-abuse religious exemptions.[165] The use of alternative medicine in the US has increased,[11][166] with a 50 percent increase in expenditures and a 25 percent increase in the use of alternative therapies between 1990 and 1997 in America.[166] According to a national survey conducted in 2002, "36 percent of U.S. adults aged 18 years and over use some form of complementary and alternative medicine."[167] Americans spend many billions on the therapies annually.[166] Most Americans used CAM to treat and/or prevent musculoskeletal conditions or other conditions associated with chronic or recurring pain.[149] In America, women were more likely than men to use CAM, with the biggest difference in use of mind-body therapies including prayer specifically for health reasons".[149] In 2008, more than 37% of American hospitals offered alternative therapies, up from 27 percent in 2005, and 25% in 2004.[168] More than 70% of the hospitals offering CAM were in urban areas.[citation needed] A survey of Americans found that 88 percent thought that "there are some good ways of treating sickness that medical science does not recognize".[11] Use of magnets was the most common tool in energy medicine in America, and among users of it, 58 percent described it as at least "sort of scientific", when it is not at all scientific.[11] In 2002, at least 60 percent of US medical schools have at least some class time spent teaching alternative therapies.[11] "Therapeutic touch" was taught at more than 100 colleges and universities in 75 countries before the practice was debunked by a nine-year-old child for a school science project.[11][91] Prevalence of use of specific therapies The most common CAM therapies used in the US in 2002 were prayer (45%), herbalism (19%), breathing meditation (12%), meditation (8%), chiropractic medicine (8%), yoga (5–6%), body work (5%), diet-based therapy (4%), progressive relaxation (3%), mega-vitamin therapy (3%) and visualization (2%).[149][169] In Britain, the most often used alternative therapies were Alexander technique, aromatherapy, Bach and other flower remedies, body work therapies including massage, Counseling stress therapies, hypnotherapy, meditation, reflexology, Shiatsu, Ayurvedic medicine, nutritional medicine, and yoga.[170] Ayurvedic medicine remedies are mainly plant based with some use of animal materials.[171] Safety concerns include the use of herbs containing toxic compounds and the lack of quality control in Ayurvedic facilities.[85][87] According to the National Health Service (England), the most commonly used complementary and alternative medicines (CAM) supported by the NHS in the UK are: acupuncture, aromatherapy, chiropractic, homeopathy, massage, osteopathy and clinical hypnotherapy.[172] In palliative care Complementary therapies are often used in palliative care or by practitioners attempting to manage chronic pain in patients. Integrative medicine is considered more acceptable in the interdisciplinary approach used in palliative care than in other areas of medicine. "From its early experiences of care for the dying, palliative care took for granted the necessity of placing patient values and lifestyle habits at the core of any design and delivery of quality care at the end of life. If the patient desired complementary therapies, and as long as such treatments provided additional support and did not endanger the patient, they were considered acceptable."[173] The non-pharmacologic interventions of complementary medicine can employ mind-body interventions designed to "reduce pain and concomitant mood disturbance and increase quality of life."[174] |
使用の普及率 2015年に発表された研究によれば、代替医療(CAM)の普及拡大は、経済的理由ではなく、道徳的信念や生活様式の選択によって説明される必要がある。[150] 発展途上国では、資源不足と貧困により必須医薬品へのアクセスが著しく制限されている。伝統療法は、しばしば代替療法と酷似しているか、その基礎を形成し ており、一次医療を構成したり、医療システムに統合されたりする可能性がある。アフリカでは一次医療の80%が伝統医療に依存し、発展途上国全体では人口 の3分の1以上が必須医薬品を利用できない状況にある。[151] ラテンアメリカでは、BIPOCコミュニティに対する不平等が彼らを伝統的慣行に縛り付け、結果として代替医療利用者の大半をこれらのコミュニティが占め ることが多い。特定のコミュニティに対する人種差別的な態度は、彼らがより都市化された医療形態を利用することを妨げている。ラテンアメリカの農村地域に おける医療アクセスを評価した研究では、差別が市民の医療アクセス能力に対する巨大な障壁であることが判明した。具体的には、先住民やアフリカ系女性、低 所得世帯が特に深刻な影響を受けている。[152] このような排除は、ラテンアメリカの少数派が既に直面している不平等をさらに悪化させる。低所得の有色人種コミュニティは、社会経済的理由などから西洋化 された医療システムの多くから一貫して排除されているため、世代を超えて信頼性が証明されている伝統医療に頼ることが多い。 デイヴィッド・ホロビンら論者は、医学研究を奨励する賞金制度の導入を提案している[153]。これは世界中のほとんどの国で研究提案に資金を提供する現 行の仕組みとは対立する。米国では、NCCIHが代替医療への公的研究資金を提供している。NCCIHは1992年以降、この種の研究に25億米ドル以上 を費やしたが、代替療法の有効性は実証されていない。[138][154][155][156][157] [158] 2011年時点で、NCCIHの姉妹組織である国立がん研究所(NIC)傘下の補完代替医療部門は、数年にわたり年間約1億500万ドルの助成金を交付し ていた。[159] 科学的根拠のない代替医療(前述の助成金対象のような)を検証することは、限られた研究資源の浪費と指摘されている。[160] [161] 代替医療が「西洋科学と科学的メソッドが医療の主要基盤として広く受け入れられ、『エビデンスに基づく』実践が主流のパラダイムである国々」で増加してい る現象は、オーストラリア医学雑誌において「謎」と評された。[162] 2022年に発表された15年間の系統的レビューでは、医療専門家におけるCAM(補完代替医療)の世界的な受容度と使用率が調査され、CAMの全体的な 受容度は52%、使用率は45%と判明した。[163] アメリカ合衆国 アメリカ合衆国では、1974年の児童虐待防止・治療法(CAPTA)により、州が連邦資金を受け取るためには、宗教に基づく治療行為に関する児童虐待・ ネグレクト法の宗教的免除を認めることが義務付けられた。[164] 31州が児童虐待に関する宗教的免除を認めている。[165] アメリカにおける代替医療の利用は増加しており、 [11][166]。1990年から1997年の間に代替療法の支出は50%、利用率は25%増加した[166]。2002年の全国調査によれば、「18 歳以上の米国成人の36%が何らかの補完代替医療を利用している」という。[167] アメリカ人は年間数十億ドルをこれらの療法に費やしている。[166] ほとんどのアメリカ人は、筋骨格系の疾患や慢性・反復性疼痛に関連する他の症状の治療や予防にCAMを利用していた。[149] アメリカでは、女性が男性よりもCAMを利用する傾向が強く、特に健康目的での祈りを含む心身療法の利用に最も大きな差が見られた。[149] 2008年には、米国の病院の37%以上が代替療法を提供しており、2005年の27%、2004年の25%から増加した。[168] CAMを提供する病院の70%以上は都市部にあった。[出典必要] アメリカ人を対象とした調査では、88%が「医学が認めない病気の治療法にも有効なものがある」と考えていた。[11] エネルギー医療において磁石の使用が最も一般的であり、その利用者の中で58%が「少なくともある程度科学的」と評価していたが、実際には全く科学的根拠 がない。[11] 2002年時点で、米国の医学部の少なくとも60%が代替療法を教える授業時間を設けていた。[11] 「セラピューティック・タッチ」は75カ国100以上の大学で教えられていたが、9歳の児童が学校の科学プロジェクトでその非科学性を暴いたことで廃れ た。[11][91] 特定療法の利用頻度 2002年に米国で最も一般的に使用されていた代替医療は、祈り(45%)、ハーブ療法(19%)、呼吸瞑想(12%)、瞑想(8%)、カイロプラク ティック(8%)、ヨガ(5~6%)、ボディワーク(5%)、食事療法(4%)、漸進的リラクゼーション(3%)、 メガビタミン療法(3%)、視覚化(2%)であった。[149][169] 英国では、最もよく利用される代替療法は、アレクサンダー・テクニック、アロマセラピー、バッハおよびその他のフラワーレメディ、マッサージを含むボディ ワーク療法、カウンセリングストレス療法、催眠療法、瞑想、リフレクソロジー、指圧、アーユルヴェーダ医学、栄養医学、ヨガであった。[170] アーユルヴェーダ医学の治療法は、主に植物ベースで、動物性材料も一部使用されている。[171] 安全上の懸念事項としては、有毒化合物を含むハーブの使用や、アーユルヴェーダ施設における品質管理の欠如などが挙げられる。[85] [87] 英国国民保健サービス(NHS)によると、英国でNHSが支援する最も一般的に使用されている補完代替医療(CAM)は、鍼治療、アロマセラピー、カイロプラクティック、ホメオパシー、マッサージ、整骨療法、臨床催眠療法である。[172] 緩和ケアにおける補完療法 補完療法は緩和ケアや、患者の慢性疼痛管理を試みる医療従事者によって頻繁に用いられる。統合医療は、他の医療分野よりも緩和ケアの学際的アプローチにお いてより受け入れられやすいと考えられている。「緩和ケアは、終末期ケアの初期経験から、質の高い終末期ケアの設計と提供において、患者の価値観と生活習 慣を中核に据える必要性を当然のこととしてきた。患者が補完療法を希望し、かつそのような治療が追加的な支援を提供し、患者の生命を危険にさらさない限 り、それらは容認可能とみなされた。」[173] 補完医療の非薬物療法は、「痛みを軽減し、それに伴う気分障害を緩和し、生活の質を高める」ことを目的とした心身療法を活用することができる。[174] |
| Regulation Further information: Regulation of alternative medicine and Regulation and prevalence of homeopathy [icon] This section needs expansion. You can help by making an edit request. (May 2018)  Health campaign flyers, as in this example from the Food and Drug Administration, warn the public about unsafe products. The alternative medicine lobby has successfully pushed for alternative therapies to be subject to far less regulation than conventional medicine.[1] Some professions of complementary/traditional/alternative medicine, such as chiropractic, have achieved full regulation in North America and other parts of the world[175] and are regulated in a manner similar to that governing science-based medicine. In contrast, other approaches may be partially recognized and others have no regulation at all.[175] In some cases, promotion of alternative therapies is allowed when there is demonstrably no effect, only a tradition of use. Despite laws making it illegal to market or promote alternative therapies for use in cancer treatment, many practitioners promote them.[176] Regulation and licensing of alternative medicine ranges widely from country to country, and state to state.[175] In Austria and Germany complementary and alternative medicine is mainly in the hands of doctors with MDs,[43] and half or more of the American alternative practitioners are licensed MDs.[177] In Germany herbs are tightly regulated: half are prescribed by doctors and covered by health insurance.[178] Government bodies in the US and elsewhere have published information or guidance about alternative medicine. The U.S. Food and Drug Administration (FDA), has issued online warnings for consumers about medication health fraud.[179] This includes a section on Alternative Medicine Fraud, such as a warning that Ayurvedic products generally have not been approved by the FDA before marketing.[180] |
規制 詳細情報:代替医療の規制およびホメオパシーの規制と普及状況 [icon] この節は拡充が必要です。編集依頼を行うことで貢献できます。(2018年5月) 食品医薬品局(FDA)のこの例のように、健康キャンペーンのチラシは一般市民に安全でない製品について警告している。 代替医療ロビーは、代替療法が従来の医療よりもはるかに少ない規制しか受けないよう成功裏に働きかけてきた。[1] カイロプラクティックなど、補完・伝統・代替医療のいくつかの専門職は、北米や世界の他の地域で完全な規制を達成しており[175]、科学に基づく医療を 統治するものと同様の方法で規制されている。一方、他の手法は部分的に認められる場合もあれば、全く規制されていないものもある[175]。効果がないこ とが証明されているにもかかわらず、使用の伝統があるという理由だけで代替療法の宣伝が許可されるケースもある。がん治療への代替療法の使用を宣伝・販売 することを違法とする法律があるにもかかわらず、多くの施術者がそれらを推奨している[176]。 代替医療の規制と免許制度は国や州によって大きく異なる[175]。オーストリアとドイツでは補完代替医療は主に医学博士(MD)を持つ医師が担っており [43]、米国の代替医療従事者の半数以上は免許を持つ医師である[177]。ドイツではハーブ療法は厳しく規制されており、その半数は医師が処方し健康 保険の対象となる[178]。 米国をはじめとする各国政府機関は、代替医療に関する情報や指針を公表している。米国食品医薬品局(FDA)は、医薬品関連の健康詐欺について消費者向け オンライン警告を発出している[179]。これには「代替医療詐欺」の項目が含まれ、例えばアーユルヴェーダ製品は一般的に販売前にFDAの承認を得てい ないとの警告が掲載されている[180]。 |
| Risks and problems The National Science Foundation has studied the problematic side of the public's attitudes and understandings of science fiction, pseudoscience, and belief in alternative medicine. They use a quote from Robert L. Park to describe some issues with alternative medicine: Alternative medicine is another concern. As used here, alternative medicine refers to all treatments that have not been proven effective using scientific methods. A scientist's view of the situation appeared in a recent book (Park 2000b)": Between homeopathy and herbal therapy lies a bewildering array of untested and unregulated treatments, all labeled alternative by their proponents. Alternative seems to define a culture rather than a field of medicine—a culture that is not scientifically demanding. It is a culture in which ancient traditions are given more weight than biological science, and anecdotes are preferred over clinical trials. Alternative therapies steadfastly resist change, often for centuries or even millennia, unaffected by scientific advances in the understanding of physiology or disease. Incredible explanations invoking modern physics are sometimes offered for how alternative therapies might work, but there seems to be little interest in testing these speculations scientifically.[11] |
リスクと問題点 米国国立科学財団は、一般市民のSFや疑似科学に対する態度や理解、代替医療への信仰といった問題点を研究している。代替医療に関する問題点を説明する際、ロバート・L・パークの言葉を引用している: 代替医療もまた懸念材料だ。ここでいう代替医療とは、科学的方法で有効性が証明されていない全ての治療法を指す。科学者の見解は近著(Park 2000b)にこう記されている: ホメオパシーとハーブ療法の間には、検証も規制もされていない治療法が驚くほど多様にある。これら全てが支持者によって「代替」と称される。代替医療は医 療分野というより文化を定義するようだ——科学的な厳密さを求めない文化である。この文化では、生物学的な科学よりも古代の伝統が重視され、臨床試験より も逸話が優先される。代替療法は変化を頑なに拒み、生理学や疾病に関する科学的進歩の影響を受けずに、しばしば数世紀、あるいは数千年にわたって存続す る。代替療法の作用機序について現代物理学を引用した信じがたい説明が提示されることもあるが、こうした推測を科学的に検証する意欲はほとんど見られな い。[11] |
| Negative outcomes See also: List of herbs with known adverse effects According to the Institute of Medicine, use of alternative medical techniques may result in several types of harm: "Direct harm, which results in adverse patient outcome."[181] "Economic harm, which results in monetary loss but presents no health hazard;" "Indirect harm, which results in a delay of appropriate treatment, or in unreasonable expectations that discourage patients and their families from accepting and dealing effectively with their medical conditions;" Interactions with conventional pharmaceuticals Forms of alternative medicine that are biologically active can be dangerous even when used in conjunction with conventional medicine. Examples include immuno-augmentation therapy, shark cartilage, bioresonance therapy, oxygen and ozone therapies, and insulin potentiation therapy. Some herbal remedies can cause dangerous interactions with chemotherapy drugs, radiation therapy, or anesthetics during surgery, among other problems.[44][132][33] An example of these dangers was reported by Associate Professor Alastair MacLennan of Adelaide University, Australia regarding a patient who almost bled to death on the operating table after neglecting to mention that she had been taking "natural" potions to "build up her strength" before the operation, including a powerful anticoagulant that nearly caused her death.[182] To ABC Online, MacLennan also gives another possible mechanism: And lastly there's the cynicism and disappointment and depression that some patients get from going on from one alternative medicine to the next, and they find after three months the placebo effect wears off, and they're disappointed and they move on to the next one, and they're disappointed and disillusioned, and that can create depression and make the eventual treatment of the patient with anything effective difficult, because you may not get compliance, because they've seen the failure so often in the past.[183] |
有害な結果 関連項目:有害作用が確認されているハーブの一覧 米国医学研究所によれば、代替医療技術の使用は以下のような複数の種類の害をもたらす可能性がある: 「直接的な害:患者の有害な結果をもたらすもの」[181] 「経済的損害:金銭的損失をもたらすが健康被害を伴わないもの」 「間接的損害:適切な治療の遅延、あるいは患者や家族が自身の病状を受け入れ効果的に対処することを妨げる不合理な期待を生むもの」 従来の医薬品との相互作用 生物学的に活性な代替医療は、従来の医療と併用しても危険な場合がある。例としては、免疫増強療法、サメ軟骨、バイオレゾナンス療法、酸素・オゾン療法、 インスリン増強療法などが挙げられる。一部のハーブ療法は、化学療法薬、放射線療法、手術中の麻酔薬などとの危険な相互作用を引き起こす可能性がある。 [44][132] [33] こうした危険性の事例として、オーストラリア・アデレード大学のアラステア・マクレナン准教授が報告した。ある患者は手術前に「体力増強」を目的とした 「自然派」薬液を服用していたことを伝えなかったため、強力な抗凝固剤の影響で手術台上で出血死寸前となった。[182] マクレナンはABCオンラインに対し、別の可能性として次のようなメカニズムも示している: 最後に、代替医療を次々と試す患者が陥る冷笑、失望、抑うつがある。3ヶ月もすればプラセボ効果が薄れ、 失望して次へ移り、また失望と幻滅を味わう。これが鬱状態を生み、最終的に効果的な治療を施すことを困難にする。なぜなら、過去に何度も失敗を経験してい るため、患者の治療への協力が得られない可能性があるからだ。[183] |
| Side-effects Conventional treatments are subjected to testing for undesired side-effects, whereas alternative therapies, in general, are not subjected to such testing at all. Any treatment – whether conventional or alternative – that has a biological or psychological effect on a patient may also have potential to possess dangerous biological or psychological side-effects. Attempts to refute this fact with regard to alternative therapies sometimes use the appeal to nature fallacy, i.e., "That which is natural cannot be harmful." Specific groups of patients such as patients with impaired hepatic or renal function are more susceptible to side effects of alternative remedies.[184][185] An exception to the normal thinking regarding side-effects is homeopathy. Since 1938, the FDA has regulated homeopathic products in "several significantly different ways from other drugs."[186] Homeopathic preparations, termed "remedies", are extremely dilute, often far beyond the point where a single molecule of the original active (and possibly toxic) ingredient is likely to remain. They are, thus, considered safe on that count, but "their products are exempt from good manufacturing practice requirements related to expiration dating and from finished product testing for identity and strength", and their alcohol concentration may be much higher than allowed in conventional drugs.[186] |
副作用 従来の治療法は望ましくない副作用について試験を受けるが、代替療法は一般的にそのような試験を全く受けていない。患者に生物学的または心理的影響を与え る治療法は、それが従来のものであれ代替のものであれ、危険な生物学的または心理的副作用を伴う可能性がある。代替療法に関してこの事実を否定しようとす る試みでは、時に「自然なものに害はない」という自然の訴求という誤謬が用いられる。肝機能や腎機能が低下している患者などの特定の患者群は、代替療法の 副作用の影響を受けやすい。[184][185] 副作用に関する通常の考え方に対する例外がホメオパシーである。1938年以来、FDAはホメオパシー製品を「他の医薬品とは大きく異なる複数の方法で」 規制している[186]。「レメディ」と呼ばれるホメオパシー製剤は極めて希釈されており、元の有効成分(そしておそらく毒性のある成分)の分子が単一で 残存する可能性のある濃度をはるかに超えていることが多い。したがって、この点では安全と見なされるが、「有効期限に関する適正製造規範(GMP)の要件 や、完成品の同一性・強度試験から免除されている」。また、アルコール濃度が従来の医薬品で許容される値を大幅に上回る場合もある。[186] |
| Treatment delay Alternative medicine may discourage people from getting the best possible treatment.[187] Those having experienced or perceived success with one alternative therapy for a minor ailment may be convinced of its efficacy and persuaded to extrapolate that success to some other alternative therapy for a more serious, possibly life-threatening illness.[188] For this reason, critics argue that therapies that rely on the placebo effect to define success are very dangerous. According to mental health journalist Scott Lilienfeld in 2002, "unvalidated or scientifically unsupported mental health practices can lead individuals to forgo effective treatments" and refers to this as opportunity cost. Individuals who spend large amounts of time and money on ineffective treatments may be left with precious little of either, and may forfeit the opportunity to obtain treatments that could be more helpful. In short, even innocuous treatments can indirectly produce negative outcomes.[189] Between 2001 and 2003, four children died in Australia because their parents chose ineffective naturopathic, homeopathic, or other alternative medicines and diets rather than conventional therapies.[190] |
治療の遅れ 代替医療は、人々が最善の治療を受けることを妨げる可能性がある。[187] 軽度の病気に対してある代替療法で成功を経験した、あるいは成功したと感じた人々は、その有効性を確信し、より深刻で命に関わる可能性のある病気に対する 他の代替療法にもその成功を当てはめようとするかもしれない。[188] このため、批判者は、プラセボ効果に依存して成功を定義する療法は非常に危険だと主張する。2002年に精神保健ジャーナリストのスコット・リリエンフェ ルドは「検証されていない、あるいは科学的に裏付けのない精神保健実践は、個人が効果的な治療を放棄する原因となり得る」と述べ、これを機会費用と呼ん だ。効果のない治療に多大な時間と金銭を費やす個人は、その貴重な資源をほとんど残さず、より有益な治療を得る機会を放棄する可能性がある。要するに、無 害な治療法でさえ間接的に悪影響を及ぼし得るのだ[189]。2001年から2003年にかけて、オーストラリアでは4人の子供が死亡した。原因は、親が 従来の治療法ではなく、効果のない自然療法、ホメオパシー、その他の代替医療や食事療法を選択したことにある[190]。 |
| Unconventional cancer "cures" There have always been "many therapies offered outside of conventional cancer treatment centers and based on theories not found in biomedicine. These alternative cancer cures have often been described as 'unproven,' suggesting that appropriate clinical trials have not been conducted and that the therapeutic value of the treatment is unknown." However, "many alternative cancer treatments have been investigated in good-quality clinical trials, and they have been shown to be ineffective.... The label 'unproven' is inappropriate for such therapies; it is time to assert that many alternative cancer therapies have been 'disproven'."[134] Edzard Ernst has stated: any alternative cancer cure is bogus by definition. There will never be an alternative cancer cure. Why? Because if something looked halfway promising, then mainstream oncology would scrutinize it, and if there is anything to it, it would become mainstream almost automatically and very quickly. All curative "alternative cancer cures" are based on false claims, are bogus, and, I would say, even criminal.[191] |
非従来型のがん「治療法」 従来型のがん治療センター外で提供される「多くの療法」は、生物医学に見られない理論に基づいている。こうした代替がん治療はしばしば「未検証」と表現さ れ、適切な臨床試験が行われておらず治療効果が不明であることを示唆している。しかし、「多くの代替がん治療法は質の高い臨床試験で検証され、効果が認め られなかった。…『未検証』というレッテルはこうした療法には不適切だ。多くの代替がん治療法は『効果が否定された』と断言すべき時が来ている」 [134] エドザード・エルンストは次のように述べている: 代替がん治療は定義上、すべて偽物だ。代替がん治療が存在するはずがない。なぜか?もし何かが半分でも有望に見えれば、主流の腫瘍学がそれを精査するから だ。もし何らかの根拠があれば、それはほぼ自動的に、そして非常に迅速に主流になる。すべての「代替がん治療」は虚偽の主張に基づいており、偽物であり、 私は言うが、犯罪的だと言える。[191] |
| Rejection of science There is no alternative medicine. There is only scientifically proven, evidence-based medicine supported by solid data or unproven medicine, for which scientific evidence is lacking. — P.B. Fontanarosa, JAMA (1998)[55] Complementary and alternative medicine (CAM) is not as well researched as conventional medicine, which undergoes intense research before release to the public.[192] Practitioners of science-based medicine also discard practices and treatments when they are shown ineffective, while alternative practitioners do not.[1] Funding for research is also sparse making it difficult to do further research for effectiveness of CAM.[193] Most funding for CAM is funded by government agencies.[192] Proposed research for CAM are rejected by most private funding agencies because the results of research are not reliable.[192] The research for CAM has to meet certain standards from research ethics committees, which most CAM researchers find almost impossible to meet.[192] Even with the little research done on it, CAM has not been proven to be effective.[194] Studies that have been done will be cited by CAM practitioners in an attempt to claim a basis in science. These studies tend to have a variety of problems, such as small samples, various biases, poor research design, lack of controls, negative results, etc. Even those with positive results can be better explained as resulting in false positives due to bias and noisy data.[195] Alternative medicine may lead to a false understanding of the body and of the process of science.[187][196] Steven Novella, a neurologist at Yale School of Medicine, wrote that government-funded studies of integrating alternative medicine techniques into the mainstream are "used to lend an appearance of legitimacy to treatments that are not legitimate."[197] Marcia Angell considered that critics felt that healthcare practices should be classified based solely on scientific evidence, and if a treatment had been rigorously tested and found safe and effective, science-based medicine will adopt it regardless of whether it was considered "alternative" to begin with.[2] It is possible for a method to change categories (proven vs. unproven), based on increased knowledge of its effectiveness or lack thereof. Prominent supporters of this position are George D. Lundberg, former editor of the Journal of the American Medical Association (JAMA) and the journal's interim editor-in-chief Phil Fontanarosa.[55] Writing in 1999 in CA: A Cancer Journal for Clinicians Barrie R. Cassileth mentioned a 1997 letter to the United States Senate's Subcommittee on Public Health and Safety, which had deplored the lack of critical thinking and scientific rigor in OAM-supported research, had been signed by four Nobel Laureates and other prominent scientists. (This was supported by the National Institutes of Health (NIH).)[198]  Neil deGrasse Tyson: Q: What do you call Alternative Medicine that survives double-blind laboratory tests? A: Regular Medicine.[199] In March 2009, a staff writer for The Washington Post reported that the impending national discussion about broadening access to health care, improving medical practice and saving money was giving a group of scientists an opening to propose shutting down the National Center for Complementary and Alternative Medicine. They quoted one of these scientists, Steven Salzberg, a genome researcher and computational biologist at the University of Maryland, as saying "One of our concerns is that NIH is funding pseudoscience." They noted that the vast majority of studies were based on fundamental misunderstandings of physiology and disease, and had shown little or no effect.[197] Writers such as Carl Sagan, a noted astrophysicist, advocate of scientific skepticism and the author of The Demon-Haunted World: Science as a Candle in the Dark (1996), have lambasted the lack of empirical evidence to support the existence of the putative energy fields on which these therapies are predicated.[90] Sampson has also pointed out that CAM tolerated contradiction without thorough reason and experiment.[200] Barrett has pointed out that there is a policy at the NIH of never saying something does not work, only that a different version or dose might give different results.[138] Barrett also expressed concern that, just because some "alternatives" have merit, there is the impression that the rest deserve equal consideration and respect even though most are worthless, since they are all classified under the one heading of alternative medicine.[201] Some critics of alternative medicine are focused upon health fraud, misinformation, and quackery as public health problems, notably Wallace Sampson and Paul Kurtz founders of Scientific Review of Alternative Medicine and Stephen Barrett, co-founder of The National Council Against Health Fraud and webmaster of Quackwatch.[202] Grounds for opposing alternative medicine include that: Alternative therapies typically lack any scientific validation, and their effectiveness either is unproven or has been disproved.[9][121][122] It is usually based on religion, tradition, superstition, belief in supernatural energies, pseudoscience, errors in reasoning, propaganda, or fraud.[148][11][9][203] Methods may incorporate or base themselves on traditional medicine, folk knowledge, spiritual beliefs, ignorance or misunderstanding of scientific principles, errors in reasoning, or newly conceived approaches claiming to heal.[148][9][204] Research on alternative medicine is frequently of low quality and methodologically flawed.[22][205] Treatments are not part of the conventional, science-based healthcare system.[206][22][207][208] Where alternative therapies have replaced conventional science-based medicine, even with the safest alternative medicines, failure to use or delay in using conventional science-based medicine has caused deaths.[189][190] Many alternative medical treatments are not patentable,[209] which may lead to less research funding from the private sector. In addition, in most countries, alternative therapies (in contrast to pharmaceuticals) can be marketed without any proof of efficacy – also a disincentive for manufacturers to fund scientific research.[210] English evolutionary biologist Richard Dawkins, in his 2003 book A Devil's Chaplain, defined alternative medicine as a "set of practices that cannot be tested, refuse to be tested, or consistently fail tests."[211] Dawkins argued that if a technique is demonstrated effective in properly performed trials then it ceases to be alternative and simply becomes medicine.[212] CAM is also often less regulated than conventional medicine.[192] There are ethical concerns about whether people who perform CAM have the proper knowledge to treat patients.[192] CAM is often done by non-physicians who do not operate with the same medical licensing laws which govern conventional medicine,[192] and it is often described as an issue of non-maleficence.[213] According to two writers, Wallace Sampson and K. Butler, marketing is part of the training required in alternative medicine, and propaganda methods in alternative medicine have been traced back to those used by Hitler and Goebels in their promotion of pseudoscience in medicine.[76][214] In November 2011 Edzard Ernst stated that the "level of misinformation about alternative medicine has now reached the point where it has become dangerous and unethical. So far, alternative medicine has remained an ethics-free zone. It is time to change this."[215] Harriet Hall criticized the low standard of evidence accepted by the alternative medicine community: Science-based medicine has one rigorous standard of evidence, the kind [used for pharmaceuticals] .... CAM has a double standard. They gladly accept a lower standard of evidence for treatments they believe in. However, I suspect they would reject a pharmaceutical if it were approved for marketing on the kind of evidence they accept for CAM.[216] |
科学の拒絶 代替医療など存在しない。科学的に証明され、 確固たるデータに裏付けられたエビデンスに基づく医療か、 科学的証拠が欠如した未検証の医療かの二者択一である。 — P.B. フォンタナローザ、JAMA (1998)[55] 補完代替医療(CAM)は、一般公開前に徹底的な研究を経る従来の医療ほど十分に研究されていない。[192] 科学に基づく医療の施術者は、効果が証明されない場合、その施術や治療法を廃棄するが、代替医療の施術者はそうしない。[1] 研究資金も乏しいため、CAMの有効性に関するさらなる研究は困難である。[193] CAMの研究資金の大半は政府機関から提供されている。[192] CAM研究の提案は、研究結果の信頼性が低いという理由で、ほとんどの民間資金提供機関から拒否される。[192] CAM研究は研究倫理委員会の定める基準を満たさねばならないが、大半のCAM研究者にとってこれはほぼ不可能だ。[192] わずかな研究すら行われていない現状では、CAMの有効性は証明されていない。[194] 実施された研究は、CAM施術者によって科学的根拠を主張するために引用される。これらの研究には、サンプル数が少ない、様々なバイアスがある、研究設計 が不十分、対照群の欠如、否定的な結果など、様々な問題がある傾向がある。肯定的な結果を示した研究でさえ、バイアスやノイズの多いデータによる偽陽性と して説明できる場合が多い。[195] 代替医療は、人体や科学のプロセスに対する誤った理解を招く恐れがある。[187][196] イエール大学医学部の神経科医スティーブン・ノベラは、代替医療技術を主流医療に統合する政府資金による研究について、「正当ではない治療法に正当性の外 観を与えるために利用されている」と記している。[197] マーシア・アンジェルは、批判派が医療行為は科学的証拠のみに基づいて分類されるべきだと考えており、治療法が厳密に検証され安全かつ有効と認められれ ば、当初「代替」と見なされていたか否かに関わらず、科学に基づく医療はそれを採用すると考えた。[2] ある手法は、その有効性または無効性に関する知識の増加に基づき、カテゴリー(実証済み vs 未実証)を変更する可能性がある。この立場の著名な支持者には、米国医師会雑誌(JAMA)の元編集長ジョージ・D・ランドバーグと、同誌の暫定編集長 フィル・フォンタナローザがいる。[55] 1999年に『CA: A Cancer Journal for Clinicians』に寄稿したバリー・R・キャシレスは、1997年に米国上院公衆衛生安全小委員会宛てに提出された書簡について言及した。この書簡 は、代替医療支援研究における批判的思考と科学的厳密性の欠如を嘆く内容で、4人のノーベル賞受賞者を含む著名な科学者たちが署名していた。(この書簡は 国立衛生研究所(NIH)によって支持された。) [198] ニール・ドグラース・タイソン: Q: 二重盲検実験に耐えた代替医療を何と呼ぶか? A: 通常の医療だ。[199] 2009年3月、ワシントン・ポスト紙のスタッフライターは、医療アクセスの拡大・医療行為の改善・経費削減をめぐる全国的な議論が迫る中、科学者グルー プが国立補完代替医療センター(NCCAM)の閉鎖を提案する機会を得たと報じた。メリーランド大学のゲノム研究者で計算生物学者であるスティーブン・サ ルツバーグは「我々の懸念の一つは、NIHが疑似科学に資金を提供していることだ」と述べたと引用された。同紙は、研究の大半が生理学や疾病に対する根本 的な誤解に基づいており、ほとんど効果を示していないと指摘した。[197] 著名な天体物理学者であり、科学的懐疑論の提唱者であり、『悪魔に憑かれた世界:暗闇のろうそくとしての科学』(1996年)の著者であるカール・セーガ ンなどの作家は、これらの療法の根拠となっている推定エネルギー場の存在を裏付ける実証的証拠の欠如を厳しく非難している。[90] サンプソンはまた、CAM は徹底的な理由や実験なしに矛盾を容認していると指摘している。[200] バレットは、NIH には「効果がない」とは決して言わず、別のバージョンや投与量で異なる結果が出るかもしれないと言うだけという方針があると指摘している。[138] バレットはまた、一部の「代替療法」にメリットがあるという理由だけで、そのほとんどは価値がないにもかかわらず、それらはすべて代替医療という一つの見 出しに分類されているため、残りの療法も同等の考慮と尊敬に値するという印象があることに懸念を表明している。[201] 代替医療に対する批判者の中には、公衆衛生上の問題として、健康詐欺、誤った情報、偽医療に焦点を当てている者もいる。特に、代替医療の科学的レビューの 創設者であるウォレス・サンプソンとポール・カーツ、そして全米健康詐欺対策協議会(NCAHF)の共同創設者であり、Quackwatch のウェブマスターであるスティーブン・バレットが挙げられる。[202] 代替医療に反対する理由としては、以下のようなものが挙げられる。 代替療法は通常、科学的な検証がまったく行われておらず、その有効性は証明されていないか、あるいは反証されている。[9][121][122] 代替医療は通常、宗教、伝統、迷信、超自然的なエネルギーへの信仰、疑似科学、推論の誤り、プロパガンダ、または詐欺に基づいている。[148][11][9][203] その方法は、伝統医学、民間知識、精神的信念、科学的原理の無知または誤解、推論の誤り、あるいは治癒を主張する新しく考案されたアプローチを取り入れたり、それらに基づいたりする場合がある。[148][9][204] 代替医療に関する研究は、質が低く方法論的に欠陥がある場合が多い。[22][205] これらの治療法は、科学に基づく従来の医療システムの一部ではない。[206][22][207][208] 代替療法が科学に基づく従来の医療に取って代わった場合、最も安全な代替医療であっても、従来の科学に基づく医療を使用しなかったこと、あるいは使用が遅れたことが死を引き起こした事例がある。[189] [190] 多くの代替医療治療法は特許を取得できない[209]ため、民間セクターからの研究資金が減少する可能性がある。さらに、ほとんどの国では、代替療法(医 薬品とは対照的に)は有効性の証明なしに販売できる。これもまた、製造業者が科学的研究に資金を提供する意欲を削ぐ要因である。[210] 英国の進化生物学者リチャード・ドーキンスは、2003年の著書『悪魔のチャプレン』において、代替医療を「検証できない、検証を拒む、あるいは検証に一 貫して失敗する一連の実践」と定義した[211]。ドーキンスは、ある技術が適切に実施された試験で有効性が実証されれば、それはもはや代替医療ではな く、単なる医療になると主張した。[212] CAMはまた、従来の医療よりも規制が緩いことが多い。[192] CAMを行う者が患者を治療する適切な知識を持っているかどうかについては、倫理的な懸念がある。[192] CAMは、従来の医療を規制する医療免許法と同じ法律で運営されていない非医師によって行われることが多く、[192] これはしばしば非加害性の問題として説明される。[213] ウォレス・サンプソンとK・バトラーの二名の著述家によれば、マーケティングは代替医療に必要な訓練の一部であり、代替医療における宣伝手法は、ヒトラーとゲッベルスが医学における疑似科学を推進するために用いた手法に遡ることができるという。[76] [214] 2011年11月、エドザード・エルンストは「代替医療に関する誤情報のレベルは、今や危険かつ非倫理的な段階に達している。これまで代替医療は倫理の適用を受けない領域であった。これを変える時が来た」と述べた。[215] ハリエット・ホールは代替医療界が容認する証拠基準の低さを批判した: 科学に基づく医療には厳格な証拠基準が一つある。それは[医薬品に用いられる]種類のものだ。一方、CAM(補完代替医療)には二重基準がある。彼らは自 らが信じる治療法には喜んで低い証拠基準を受け入れる。しかし、もし医薬品がCAMで受け入れられる種類の証拠で承認されたなら、彼らはそれを拒否するだ ろうと私は疑っている。[216] |
| Conflicts of interest Some commentators have said that special consideration must be given to the issue of conflicts of interest in alternative medicine. Edzard Ernst has said that most researchers into alternative medicine are at risk of "unidirectional bias" because of a generally uncritical belief in their chosen subject.[217] Ernst cites as evidence the phenomenon whereby 100% of a sample of acupuncture trials originating in China had positive conclusions.[217] David Gorski contrasts evidence-based medicine, in which researchers try to disprove hyphotheses, with what he says is the frequent practice in pseudoscience-based research, of striving to confirm pre-existing notions.[218] Harriet Hall writes that there is a contrast between the circumstances of alternative medicine practitioners and disinterested scientists: in the case of acupuncture, for example, an acupuncturist would have "a great deal to lose" if acupuncture were rejected by research; but the disinterested skeptic would not lose anything if its effects were confirmed; rather their change of mind would enhance their skeptical credentials.[219] |
利益相反 一部の評論家は、代替医療における利益相反の問題には特別な配慮が必要だと述べている。エドザード・エルンストは、代替医療の研究者の大半が、自らの研究 対象に対する批判的でない信念ゆえに「一方向的な偏り」の危険にさらされていると指摘している。[217] アーンストは証拠として、中国発の鍼治療試験のサンプル100%が肯定的結論を示した現象を挙げている。[217] デイヴィッド・ゴースキは、研究者が仮説を反証しようとするエビデンスに基づく医療と、疑似科学に基づく研究で頻繁に見られる「既存の概念を立証しようと する姿勢」とを対比させている。[218] ハリエット・ホールは、代替医療実践者と無利害の科学者との状況の違いを指摘している。例えば鍼治療の場合、鍼灸師は研究で鍼治療が否定されれば「大きな 損失を被る」が、無利害の懐疑論者はその効果が確認されても何も失わない。むしろ考えを改めることで懐疑論者としての信頼性を高められるのだ。[219] |
| Use of health and research resources Research into alternative therapies has been criticized for "diverting research time, money, and other resources from more fruitful lines of investigation in order to pursue a theory that has no basis in biology."[64][40] Research methods expert and author of Snake Oil Science, R. Barker Bausell, has stated that "it's become politically correct to investigate nonsense."[138] A commonly cited statistic is that the US National Institute of Health had spent $2.5 billion on investigating alternative therapies prior to 2009, with none being found to be effective.[138] |
健康と研究資源の活用 代替療法の研究は「生物学的な根拠のない理論を追求するために、より実りある研究分野から研究時間、資金、その他の資源を転用している」と批判されてき た。[64][40] 研究方法論の専門家であり『Snake Oil Science』の著者であるR. Barker Bausellは、「ナンセンスを調査することが政治的に正しいとされるようになった」と述べている。[138] よく引用される統計として、米国国立衛生研究所(NIH)は2009年までに代替療法の調査に25億ドルを費やしたが、有効性が確認されたものは一つもな かったという。[138] |
| Alternative therapies for developmental and learning disabilities Conservation medicine Ethnomedicine Psychic surgery Siddha medicine Thomsonianism, in United States early 19th century Chelation of heavy metals in autism |
発達障害と学習障害に対する代替療法 保全医学 民族医学 霊的手術 シッダ医学 19世紀初頭のアメリカにおけるトムソン主義 自閉症における重金属キレート療法 |
| Notes | Notes リンク先を参照してください |
| References Barrett, Stephen; Hall, Harriet; Baratz, Robert S.; London, William M.; Kroger, Manfred (2013). Consumer health: a guide to intelligent decisions (9th ed.). New York: McGraw-Hill. pp. 34–35, 134, 137. ISBN 978-0-07-802848-9. OCLC 758098687. Angell, M.; et al. (1998). "Alternative medicine--The risks of untested and unregulated remedies" (PDF). New England Journal of Medicine. 339 (12): 839–841. CiteSeerX 10.1.1.694.9581. doi:10.1056/NEJM199809173391210. PMID 9738094. Archived (PDF) from the original on 2022-10-09. Shapiro, Rose (2010). Suckers: How Alternative Medicine Makes Fools of Us All. Random House. p. 8. ISBN 978-1-4090-5916-5. Further rebranding has given rise to the notion of 'integrated medicine'. Bombardieri, D; Easthope, G (October 2000). "Convergence between Orthodox and Alternative Medicine: A Theoretical Elaboration and Empirical Test". Health. 4 (4): 479–494. doi:10.1177/136345930000400404. S2CID 71900519. Shuval, Judith T.; Averbuch, Emma (2012). "Complementary and Alternative Healthcare in Israel". Israel Journal of Health Policy Research. 1 (7): 7. doi:10.1186/2045-4015-1-7. PMC 3424827. PMID 22913721. Freedman, David H. (July–August 2011). "The Triumph of New-Age Medicine". The Atlantic. Archived from the original on 10 May 2015. Retrieved 6 June 2015. Gorski, David (August 15, 2011). "Integrative medicine": A brand, not a specialty. sciencebasedmedicine.org. (Retrieved March 25, 2022). "Directive 2004/24/EC of the European Parliament and of the Council". Official Journal of the European Union. 2004-04-30. Sampson, Wallace (June 1995). "Antiscience Trends in the Rise of the Alternative Medicine Movement". Annals of the New York Academy of Sciences. 775 (1): 188–197. doi:10.1111/j.1749-6632.1996.tb23138.x. ISSN 0077-8923. PMID 8678416. S2CID 2813395. Kolata, Gina (June 17, 1996), "On Fringes of Health Care, Untested Therapies Thrive", The New York Times, retrieved December 22, 2015 National Science Foundation (April 2002). "Chapter 7: Science and Technology: Public Attitudes and Public Understanding: Science Fiction and Pseudoscience". National Science Foundation. Archived from the original on February 18, 2007. Retrieved March 15, 2023. IOM Report 2005, p. 19. Hines, Terence (2003). Pseudoscience and the Paranormal (2nd ed.). Amerst, New York: Prometheue Books. ISBN 978-1-57392-979-0.; Sampson, Walter (March 2001). "The Need for Educational Reform in Teaching about Alternative Therapies". Academic Medicine. 76 (3): 248–250. doi:10.1097/00001888-200103000-00011. PMID 11242574.; Coulter, Ian D; Willis, Evan M (June 2004). "The Rise and Rise of Complementary and Alternative Medicine: a Sociological Perspective". Medical Journal of Australia. 180 (11): 587–589. doi:10.5694/j.1326-5377.2004.tb06099.x. PMID 15174992. S2CID 15983789.; Sagan 1996 Kent Heather (1997). "Ignore Growing Patient Interest in Alternative Medicine at Your Peril – MDs Warned". Canadian Medical Association Journal. 157 (10): 1427–1428. PMC 1228476. PMID 9371077. Goldrosen MH, Straus SE (2004). "Complementary and alternative medicine: assessing the evidence for immunological benefits". Nature Reviews Immunology. 4 (11): 912–921. doi:10.1038/nri1486. PMID 15516970. S2CID 11708302. Harrison's Principles of Internal Medicine 2015, p. 1, chpt. 14-E. "Complementary Medicine – Alternative Medical Systems". WebMD. 2014-01-14. Archived from the original on 2015-06-01. Retrieved 2015-06-04. "The Use of Complementary and Alternative Medicine in the United States". National Center for Complementary and Integrative Health. 2015-04-07. Archived from the original on 2015-06-01. Retrieved 2015-06-04. Beyerstein BL (2001). "Alternative medicine and common errors of reasoning". Academic Medicine. 76 (3): 230–237. doi:10.1097/00001888-200103000-00009. PMID 11242572. S2CID 41527148. Saks, M. (1992). "Introduction". In Saks, M. (ed.). Alternative Medicine in Britain. Oxford: Clarendon Press. pp. 1–21. ISBN 978-0-19-827278-6. IOM Report 2005, p. 19. "Complementary, Alternative, or Integrative Health: What's In a Name?". National Center for Complementary and Integrative Health (NCCIH), National Institutes of Health (NIH), US Dept. of Health and Human Services (US HHS). May 2002. Archived from the original on 2005-12-08. Retrieved 2022-12-01. Sir Walton: Science and Technology Committee 2000, Chapter 1: Introduction. Kopelman 2004. Wieland et al. 2011. Astin, J.A.; et al. (1998). "A review of the incorporation of complementary and alternative medicine by mainstream physicians". JAMA Internal Medicine. 158 (21): 2303–2310. doi:10.1001/archinte.158.21.2303. PMID 9827781. Pelletier, K.R.; et al. (1997). "Current trends in the integration and reimbursement of complementary and alternative medicine by managed care, insurance carriers, and hospital providers". American Journal of Health Promotion. 12 (2): 112–122. doi:10.4278/0890-1171-12.2.112. PMID 10174663. S2CID 46772634. IOM Report 2005, pp. 17, 196–252. White House Commission on Complementary and Alternative Medicine Policy Staff; Dept. of Health and Human Services Staff United States (March 2002). "Overview of CAM in the United States: Recent History, Current Status, And Prospects for the Future". White House Commission on Complementary and Alternative Medicine Policy Final Report (Report). US Government Printing Office. ISBN 978-0-16-051476-0. Archived from the original on 2013-02-15. Chapter 2 archived 2011-08-25. Ernst, E. (1995). "Complementary medicine: Common misconceptions". Journal of the Royal Society of Medicine. 88 (5): 244–247. PMC 1295191. PMID 7636814. Complementary medicine, defined as health care which lies for the most part outside the mainstream of conventional medicine. Joyce, C.R.B. (1994). "Placebo and complementary medicine". The Lancet. 344 (8932): 1279–1281. doi:10.1016/S0140-6736(94)90757-9. PMID 7967992. S2CID 36724993. May, J. (2011). "What is integrative health?". BMJ. 343: d4372. doi:10.1136/bmj.d4372. PMID 21750063. S2CID 206893456. "Complementary and Alternative Medicine in Cancer Treatment (PDQ®): Questions and Answers About Complementary and Alternative Medicine in Cancer Treatment". NCI website. Physician Data Query (PDQ). National Cancer Institute (NCI), NIH. Archived from the original on 2012-12-15. Retrieved 2012-12-11. Borkan, J. (2012). "Complementary alternative health care in Israel and the western world". Israel Journal of Health Policy Research. 1 (1) 8. doi:10.1186/2045-4015-1-8. PMC 3424836. PMID 22913745. "What is Complementary and Alternative Medicine (CAM)?". National Center for Complementary and Alternative Medicine. Archived from the original on 2005-12-08. Retrieved 2006-07-11. Zeller, T.; Muenstedt, K.; Stoll, C.; Schweder, J.; Senf, B.; Ruckhaeberle, E.; Becker, S.; Serve, H.; Huebner, J. (2013-03-01). "Potential interactions of complementary and alternative medicine with cancer therapy in outpatients with gynecological cancer in a comprehensive cancer center". Journal of Cancer Research and Clinical Oncology. 139 (3): 357–365. doi:10.1007/s00432-012-1336-6. ISSN 1432-1335. PMC 11824351. PMID 23099993. S2CID 29598970. Ben-Arye, Eran; Polliack, Aaron; Schiff, Elad; Tadmor, Tamar; Samuels, Noah (2013-12-01). "Advising patients on the use of non-herbal nutritional supplements during cancer therapy: a need for doctor-patient communication". Journal of Pain and Symptom Management. 46 (6): 887–896. doi:10.1016/j.jpainsymman.2013.02.010. ISSN 1873-6513. PMID 23707384. Li, B; Forbes, T.; Byrne, J. (2018). "Integrative medicine or infiltrative pseudoscience?". The Surgeon. 16 (5): 271–277. doi:10.1016/j.surge.2017.12.002. PMID 29305045. S2CID 19580427. "Complementary and alternative medicine". National Health Service. March 1, 2022. Retrieved 2023-05-06. "The difference between complementary and alternative therapies (CAMs)". Cancer Research UK. 4 April 2022. Retrieved 2023-05-06. "Complementary and Alternative Medicine for Cancer Patients". Centers for Disease Control and Prevention. 2022-06-09. Retrieved 2023-05-06. Belloni, Silvia; Bonucci, Massimo; Arrigoni, Cristina; Dellafiore, Federica; Caruso, Rosario (2023-01-01). "A Systematic Review of Systematic Reviews and a Pooled Meta-Analysis on Complementary and Integrative Medicine for Improving Cancer-Related Fatigue". Clinical Therapeutics. 45 (1): e54 – e73. doi:10.1016/j.clinthera.2022.12.001. ISSN 0149-2918. PMID 36566113. S2CID 255049739. Greenlee, Heather; Zick, Suzanna M.; Rosenthal, David; Cohen, Lorenzo; Cassileth, Barrie; Tripathy, Debu (March 2015). "Integrative oncology — strong science is needed for better patient care". Nature Reviews Cancer. 15 (3): 165. doi:10.1038/nrc3822-c1. ISSN 1474-1768. PMID 25693833. S2CID 8053861. Gorski, D. (2010-08-03). "Credulity about acupuncture infiltrates The New England Journal of Medicine". Science-Based Medicine. Archived from the original on 2013-09-28. Caldwell, Elizabeth Frances (2017-07-03). "Quackademia? Mass-Media Delegitimation of Homeopathy Education". Science as Culture. 26 (3): 380–407. doi:10.1080/09505431.2017.1316253. ISSN 0950-5431. S2CID 151442812. Robert Todd Carroll. Integrative medicine. Skeptic's Dictionary Elsevier Science (2002). "Author interview (Edzard Ernst, editor of The Desktop Guide to Complementary and Alternative Medicine)". Harcourt International. Archived from the original on 2002-03-02. Cassileth, B.R.; et al. (2004). "Complementary and alternative therapies for cancer". The Oncologist. 9 (1): 80–89. doi:10.1634/theoncologist.9-1-80. PMID 14755017. S2CID 6453919. Tyreman, Stephen (2011-05-01). "Values in complementary and alternative medicine". Medicine, Health Care and Philosophy. 14 (2): 209–217. doi:10.1007/s11019-010-9297-5. ISSN 1572-8633. PMID 21104324. S2CID 32143622. WHO global report on traditional and complementary medicine (PDF). World Health Organization (Report). Geneva. 2019. ISBN 978-92-4-151543-6. Archived (PDF) from the original on 2022-07-29. Retrieved 2022-12-06. Gorski, David (29 September 2014). "Quackademia update: The Cleveland Clinic, George Washington University, and the continued infiltration of quackery into medical academia". Science-Based Medicine. Retrieved 8 April 2025. "Integrative Medicine Exam Description". American Board of Physician Specialties. July 16, 2021. Retrieved March 11, 2022. Wake, Getu Engida; Fitie, Girma Wogie (29 April 2022). "Magnitude and Determinant Factors of Herbal Medicine Utilization Among Mothers Attending Their Antenatal Care at Public Health Institutions in Debre Berhan Town, Ethiopia". Frontiers in Public Health. 10 883053. Bibcode:2022FrPH...1083053W. doi:10.3389/fpubh.2022.883053. ISSN 2296-2565. PMC 9098925. PMID 35570953. Traditional medicine is defined as the ways of protecting and restoring health that existed before the arrival of modern medicine. It is underestimated part of healthcare that finds in almost every country in the world. Traditional medicine has been being used in the maintenance of health and the prevention, diagnosis, improvement, or treatment of physical and mental illness. Che, C.-T.; George, V.; Ijinu, T.P.; Pushpangadan, P.; Andrae-Marobela, K. (2017). "Traditional Medicine". Pharmacognosy. Elsevier. pp. 15–30. doi:10.1016/B978-0-12-802104-0.00002-0. ISBN 978-0-12-802104-0. Traditional medicine, as defined by the World Health Organization, is the sum total of the knowledge, skills, and practices based on the theories, beliefs, and experiences indigenous to different cultures, whether explicable or not, used in the maintenance of health as well as in the prevention, diagnosis, improvement, or treatment of physical and mental illness. Some traditional medicine systems are supported by huge volumes of literature and records of the theoretical concepts and practical skills; others pass down from generation to generation through verbal teaching. Draft preliminary report on traditional medicine and its ethical implications. Paris: UNESCO International Bioethics Committee. 2010. p. 5. Retrieved 29 March 2023. Whereas traditional medicine is based on analogical reasoning and a holistic approach to disease and health, conventional medicine rests on scientific knowledge and is evidence-based. Li, Fu-Shuang; Weng, Jing-Ke (31 July 2017). "Demystifying traditional herbal medicine with modern approach". Nature Plants. 3 (8): 17109. Bibcode:2017NatPl...317109L. doi:10.1038/nplants.2017.109. ISSN 2055-0278. PMID 28758992. S2CID 2127457. Although the initial development of these holistic traditional herbal prescriptions predated modern science, the process was based on thousands of years of phenotype-based and personalized human clinical trials. Meanwhile, meticulous descriptions of disease symptoms and systematic medical theories have also been recorded by generations of herbal doctors, relating therapeutic properties of diverse medicinal plants to their utility in treating specific symptoms. Yet most of the foundational concepts in the traditional medical systems—for example, the concepts of yin versus yang and cold versus hot in traditional Chinese medicine—are disconnected from the modern descriptions of normal and disease states in the language of physiology and molecular biology. The lack of modern scientific and clinical evidence for safety, efficacy and action mechanisms further prevented those holistic herbal medicine prescriptions from being accepted beyond their culture of origin. Jansen, C.; Baker, J.D.; Kodaira, E.; Ang, L.; Bacani, A.J.; Aldan, J.T.; Shimoda, L.M.N.; Salameh, M.; Small-Howard, A.L.; Stokes, A.J.; Turner, H.; Adra, C.N. (March 2021). "Medicine in motion: Opportunities, challenges and data analytics-based solutions for traditional medicine integration into western medical practice". Journal of Ethnopharmacology. 267 113477. doi:10.1016/j.jep.2020.113477. ISSN 0378-8741. PMC 7577282. PMID 33098971. When adopted outside its traditional or root culture, traditional medicine is often classified as a form of alternative medicine (AM), for example by Western professional medical organizations, insurers and healthcare systems. This problematically leads to lack of regulation (e.g., in the U.S. where these approaches are at best relegated to the nutraceutical market largely outside the FDA sphere of regulation) and a lack of fidelity to original formulations, dose schedules, delivery methods and indications. Tabish, Syed Amin (2008). "Complementary and Alternative Healthcare: Is it Evidence-based?". International Journal of Health Sciences. 2 (1): V–IX. ISSN 1658-3639. PMC 3068720. PMID 21475465. Complementary and alternative healthcare and medical practices (CAM) is a group of diverse medical and health care systems, practices, and products that are not presently considered to be part of conventional medicine. The list of practices that are considered as CAM changes continually as CAM practices and therapies that are proven safe and effective become accepted as the "mainstream" healthcare practices...Alternative medicine is commonly categorized together with complementary medicine under the umbrella term "complementary and alternative medicine". Complementary medicine refers to therapies that complement traditional western (or allopathic) medicine and is used together with conventional medicine, and alternative medicine is used in place of conventional medicine. Alternative medicine refers to therapeutic approaches taken in place of traditional medicine and used to treat or ameliorate disease. Fontanarosa, P.B.; et al. (1998). "Alternative medicine meets science". JAMA. 280 (18): 1618–1619. doi:10.1001/jama.280.18.1618. PMID 9820267. S2CID 5485601. Beresford, M. J. (15 April 2010). "Medical reductionism: lessons from the great philosophers". QJM. 103 (9). Oxford University Press (OUP): 721–724. doi:10.1093/qjmed/hcq057. ISSN 1460-2725. PMID 20395240. Unfortunately, the term 'holistic medicine' has been somewhat hijacked by alternative therapists and is often thought mistakenly to be at odds with conventional medicine. Zucker, Arthur (January 1979). "Reductionism and holistic medicine". Journal of Social and Biological Systems. 2 (1). Elsevier BV: 39–42. doi:10.1016/0140-1750(79)90019-8. ISSN 0140-1750. Offit, P. (2013). Do You Believe in Magic?: The Sense and Nonsense of Alternative Medicine. HarperCollins. ISBN 978-0-06-222296-1. Also published in the UK as Offit, Dr Paul (2013). Killing Us Softly: The Sense and Nonsense of Alternative Medicine. HarperCollins Publishers. ISBN 978-0-00-749173-5. Diamond, J. quoted in Dawkins 2003. (p. 36 in 2004 US ed. ISBN 0618335404). IOM Report 2005, pp. 14–20. Sointu 2012, p. 13. Nissen, N.; et al. (2013). "Researching alternative and complementary therapies: Mapping the field". Medical Anthropology. 32 (1): 1–7. doi:10.1080/01459740.2012.718016. PMID 23206171. S2CID 31843233. Carroll, R.T. (2011-05-14). "complementary medicine". The Skeptics Dictionary (Online ed.). Archived from the original on 2013-09-27. 2013-09-27. Novella, S. (2010-08-04). "Acupuncture pseudoscience in The New England Journal of Medicine". Science-Based Medicine. Archived from the original on 2013-09-28. Jeffery, Nick (2015). "There is no such thing as alternative medicine". Editorial. Journal of Small Animal Practice. 56 (12): 687–688. doi:10.1111/jsap.12427. ISSN 1748-5827. PMID 26735773. O'Connor 1995, p. 2. Sarris, J.; et al. (2010). Clinical Naturopathy: An Evidence-based Guide to Practice. Elsevier Health Sciences. ISBN 978-0-7295-7926-1. Jagtenberg T, Evans S, Grant A, Howden I, Lewis M, Singer J (2006). "Evidence-based medicine and naturopathy". J Altern Complement Med. 12 (3): 323–328. doi:10.1089/acm.2006.12.323. PMID 16646733. Archived from the original on 2018-02-22. Retrieved 2017-05-13. Ernst E (2001). "Rise in popularity of complementary and alternative medicine: reasons and consequences for vaccination". Vaccine. 20 (Suppl 1): S89 – S93. doi:10.1016/S0264-410X(01)00290-0. PMID 11587822. "Naturopathic Medicine". American Cancer Society. 1 Nov 2008. Archived from the original on 3 April 2015. Retrieved 20 Nov 2010. Hahnemann 1833, pp. iii, 48–49. Ernst, E. (2002). "A systematic review of systematic reviews of homeopathy". British Journal of Clinical Pharmacology. 54 (6): 577–582. doi:10.1046/j.1365-2125.2002.01699.x. PMC 1874503. PMID 12492603. House of Commons: Science and Technology Committee (22 February 2010). Evidence Check 2: Homeopathy (PDF) (Report). HC 45, Fourth Report of Session 2009–2010. London: The Stationery Office. Shang, Aijing; Huwiler-Müntener, Karin; Nartey, Linda; Jüni, Peter; Dörig, Stephan; Sterne, Jonathan AC; Pewsner, Daniel; Egger, Matthias (2005), "Are the clinical effects of homoeopathy placebo effects? Comparative study of placebo-controlled trials of homoeopathy and allopathy", The Lancet, 366 (9487): 726–732, doi:10.1016/S0140-6736(05)67177-2, PMID 16125589, S2CID 17939264 "Homeopathy: An Introduction". Backgrounders. NCCIH. 2013 [2009]. Archived from the original on 2013-10-15. Sampson, W. (1995). "Antiscience Trends in the Rise of the "Alternative Medicine" Movement". Annals of the New York Academy of Sciences. 775 (1): 188–197. doi:10.1111/j.1749-6632.1996.tb23138.x. PMID 8678416. S2CID 2813395. Beyerstein, BL; Wallace Sampson (1996). "Traditional Medicine and Pseudoscience in China: A Report of the Second CSICOP Delegation (Part 1)". Skeptical Inquirer. 20 (4). Archived from the original on 2009-10-04. Lu, Gwei-Djen; Needham, Joseph (1980). Celestial Lancets: a History and Rationale of Acupuncture and Moxa. Cambridge and New York: Cambridge University Press. ISBN 978-0-521-21513-8. Maciocia, Giovanni (1995). Tongue Diagnosis in Chinese Medicine. Seattle: Eastland Press. ISBN 978-0-939616-19-0. Camillia Matuk (2006). "Seeing the Body: The Divergence of Ancient Chinese and Western Medical Illustration" (PDF). Journal of Biocommunication. 32 (1). Archived (PDF) from the original on 2022-10-09. Deshpande, Vijaya (January 1987). "Medieval Transmission of Alchemical and Chemical Ideas between India and China" (PDF). Indian Journal of History of Science. 22 (1): 15–28. PMID 11622483. Archived from the original (PDF) on 2015-05-05. Wujastyk 2003, p. xviii. Mishra 2004, p. 8. Dasgupta, Amitava; Hammett-Stabler, Catherine A (2011). Herbal Supplements: Efficacy, Toxicity, Interactions with Western Drugs, and Effects on Clinical Laboratory Tests. Hoboken NJ: John Wiley and Sons. pp. 202–205. ISBN 978-0-470-43350-8. Valiathan, M.S. (2006). "Ayurveda: Putting the house in order" (PDF). Guest Editorial. Current Science. 90 (1): 5–6. Archived (PDF) from the original on 2022-10-09. Centers for Disease Control Prevention (CDC) (9 July 2004). "Lead Poisoning Associated with Ayurvedic Medications – Five States, 2000–2003". Morbidity and Mortality Weekly Report. 53 (26): 582–584. PMC 2768057. PMID 15241300. Saper, R.B.; et al. (2008). "Lead, mercury, and arsenic in US- and Indian-manufactured Ayurvedic medicines sold via the Internet". JAMA. 300 (8): 915–923. doi:10.1001/jama.300.8.915. PMC 2755247. PMID 18728265. Hall, Harriet (2017-12-14). "Ayurveda: Ancient Superstition, Not Ancient Wisdom". Skeptical Inquirer. Retrieved 1 February 2018. Breeher L, Mikulski MA, Czeczok T, Leinenkugel K, Fuortes LJ (6 Apr 2015). "A cluster of lead poisoning among consumers of Ayurvedic medicine". International Journal of Occupational and Environmental Health. 21 (4): 303–307. doi:10.1179/2049396715Y.0000000009. PMC 4727589. PMID 25843124. Sagan 1996. Rosa L, Rosa E, Sarner L, Barrett S (April 1998). "A close look at therapeutic touch". JAMA. 279 (13): 1005–1010. doi:10.1001/jama.279.13.1005. PMID 9533499. Abdulla, Sara (May 13, 1999). "Phytotherapy – good science or big business?". Nature. doi:10.1038/news990513-8. Science-based medicine, with its emphasis on controlled study, proof, evidence, statistical significance and safety is being rejected in favour of 'alternative medicine' – an atavistic portmanteau of anecdote, hearsay, rumour and hokum. ... Probably the most commercially successful and widely used branch of alternative or complementary medicine is 'phytotherapy'. These are the tablets, powders and elixirs, otherwise known as herbal medicine, that are sold in most countries, through health shops and pharmacies as 'nutritional supplements'. ... Only a tiny minority of these remedies have been shown to have mild-to moderately beneficial health effects ... So why are affluent, otherwise rational, highly educated people (for this is the average user profile) so hungry for phytotherapy? ... people still believe that 'natural' equals good and safe despite plenty of evidence to the contrary. ... as far as the human body is concerned, 'natural' is meaningless ... Equally, what's so safe about consuming substances that need meet no standards of contents? De Smet, Peter A.G.M. (December 1997). "The Role of Plant-Derived Drugs and Herbal Medicines in Healthcare". Drugs. 54 (6): 801–840. doi:10.2165/00003495-199754060-00003. PMID 9421691. S2CID 46970414. "According to a New Government Survey, 38 Percent of Adults and 12 Percent of Children Use Complementary and Alternative Medicine" (Press release). NIH News. Bethseda, Maryland: National Center for Complementary and Integrative Medicine. 10 December 2008. Archived from the original on April 7, 2015. Retrieved 4 June 2015. Pearce, Alison; Simpson, Neil (March 1998). "A paediatrician's guide to complementary medicine". Current Paediatrics. 8 (1): 62–67. doi:10.1016/S0957-5839(98)80061-4. "Faith Healing – Making Treatment Decisions". American Cancer Society. June 15, 2009. Archived from the original on February 12, 2010. Retrieved May 28, 2018. Aviles, Jennifer M.; Whelan, Sr Ellen; Hernke, Debra A.; Williams, Brent A.; Kenny, Kathleen E.; O'Fallon, W. Michael; Kopecky, Stephen L. (December 2001). "Intercessory Prayer and Cardiovascular Disease Progression in a Coronary Care Unit Population: A Randomized Controlled Trial". Mayo Clinic Proceedings. 76 (12): 1192–1198. doi:10.4065/76.12.1192. PMID 11761499. S2CID 7300728. "Energy Medicine: An Overview". Backgrounders. NCCIH. 2005 [2004]. Archived from the original on 2016-05-22. Quack Medicine: A History of Combating Health Fraud in Twentieth-Century America, Eric W. Boyle, [1] Whorton, James (2003). "Countercultural Healing: A brief History of Alternative Medicine in America". PBS Frontline. Retrieved 2022-03-25. Coulter, Ian D.; Willis, Evan M. (2004-06-07). "The rise and rise of complementary and alternative medicine: a sociological perspective". Medical Journal of Australia. 180 (11): 587–589. doi:10.5694/j.1326-5377.2004.tb06099.x. ISSN 0025-729X. PMID 15174992. S2CID 15983789. Whorton, James C. (2002). Nature Cures: The History of Alternative Medicine in America. Oxford University Press. ISBN 978-0-19-534978-8. "The Alternative Fix: Introduction". www.pbs.org. PBS Frontline. November 3, 2003. Wallis, Claudia (November 4, 1991). "Cover Stories: Why New Age Medicine Is Catching On". Time. Vol. 138, no. 18. ISSN 0040-781X. Retrieved 2022-03-25. Ankerberg, John; Weldon, John (1996). New Age Medicine, Encyclopedia of New Age Beliefs. Harvest House Publishers. pp. 470–508. ISBN 978-1-56507-160-5. Smith, T (1983). "Alternative medicine". British Medical Journal (Clinical Research Ed.). 287 (6388): 307–308. doi:10.1136/bmj.287.6388.307. PMC 1548588. PMID 6307462. One of the few growth industries in contemporary Britain is alternative medicine. An apparently endless stream of books, articles, and radio and television programmes urge on the public the virtues of treatments ranging from meditation to drilling a hole in the skull to let in more oxygen. Kruger, Helen (1974). Other Healers, Other Cures: A Guide to Alternative Medicine. Bobbs-Merrill. ISBN 978-0-672-51708-2. Law, Donald (1975). A Guide to Alternative Medicine. Turnstone Press. ISBN 978-0-85500-107-0. Winnick, T.A. (2005). "From quackery to "complementary" medicine: The American medical profession confronts alternative therapies". Social Problems. 52 (1): 38–61. doi:10.1525/sp.2005.52.1.38. JSTOR 10.1525/sp.2005.52.1.38. Winnick, T.A. (2009). "From Quackery to "Complementary" Medicine: The American Medical Profession Confronts Alternative Therapies". In Conrad, P. (ed.). The Sociology of Health and Illness (8th ed.). New York: Worth. pp. 261–277. ISBN 978-1-4292-0558-0. Young, J.H. (1998). "The Development of the Office of Alternative Medicine in the National Institutes of Health, 1991–1996". Bulletin of the History of Medicine. 72 (2): 279–298. doi:10.1353/bhm.1998.0110. PMID 9628052. S2CID 26685737. Flexner, A. (1910). Medical Education in the United States and Canada A Report to the Carnegie Foundation (Report). Boston: D. B. Updike, Merrymount Press. Available from CFAT: The Flexner Report Archived 2013-11-05 at the Wayback Machine Ludmerer, K.M. (2010). "Commentary: Understanding the Flexner Report" (PDF). Academic Medicine. 85 (2): 193–196. doi:10.1097/ACM.0b013e3181c8f1e7. PMID 20107341. Archived (PDF) from the original on 2022-10-09. Bianco, C. (April 2000). "How Becoming a Doctor Works: Medical School Curriculum". HowStuffWorks website. Archived from the original on 2013-10-05. "Stanford's medical curriculum". Stanford University website. Stanford University School of Medicine. Archived from the original on 2013-05-09. Retrieved 2013-01-26. "Medical Student Education Program: Curriculum Overview". Yale University website. Yale School of Medicine. Archived from the original on 2013-10-04. Snyderman, R.; et al. (2002). "Integrative medicine: Bringing medicine back to its roots". JAMA Internal Medicine. 162 (4): 395–397. doi:10.1001/archinte.162.4.395. PMID 11863470. S2CID 46177131. Berman, B.M. (2001). "Complementary medicine and medical education". BMJ. 322 (7279): 121–132. doi:10.1136/bmj.322.7279.121. PMC 1119400. PMID 11159555. "Cochrane CAM Field". University of Maryland website. Center for Integrative Medicine, School of Medicine, University of Maryland. Archived from the original on 2013-09-28. "Center for Integrative Medicine". University of Maryland website. University of Maryland School of Medicine. Archived from the original on 2010-03-23. "Doctor of medicine profession (MD)". MedlinePlus. US National Library of Medicine, NIH. 2011-02-03. Archived from the original on 2013-01-27. Retrieved 2012-12-20. Kent, H. (1997). "Ignore growing patient interest in alternative medicine at your peril - MDs warned". Canadian Medical Association Journal. 157 (10): 1427–1428. PMC 1228476. PMID 9371077. Goldrosen, M.H.; et al. (2004). "Complementary and alternative medicine: assessing the evidence for immunological benefits". Perspective. Nature Reviews Immunology. 4 (11): 912–921. doi:10.1038/nri1486. PMID 15516970. S2CID 11708302. IOM Report 2005. Sarris, J. (2012). "Current challenges in appraising complementary medicine evidence" (PDF). Medical Journal of Australia. 196 (5): 310–311. doi:10.5694/mja11.10751. PMID 22432660. S2CID 31044567. Archived (PDF) from the original on 2022-10-09. Alcock, J. (1999). "Alternative medicine and the psychology of belief". Scientific Review of Alternative Medicine. 3 (2). Ernst, E. "The HealthWatch Award 2005: Prof. Edzard Ernst: Complementary medicine: The good the bad and the ugly". UK: HealthWatch. Archived from the original on 2013-10-16. Ernst, E. (2011). "How Much of CAM Is Based on Research Evidence?". Evidence-Based Complementary and Alternative Medicine. 2011 676490. doi:10.1093/ecam/nep044. PMC 3136881. PMID 19465405. "Alternative Medicine: Think yourself better". The Economist. 2011-05-19. pp. 83–84. Archived from the original on 2011-05-22. Ernst, E. (2008). "Placebo and other Non-specific Effects". In Ernst, E. (ed.). Healing, Hype, or Harm? A Critical Analysis of Complementary or Alternative Medicine. Imprint Academic, Societas. ISBN 978-1-84540-118-4. Katz, D.L.; et al. (2003). "The evidence base for complementary and alternative medicine: Methods of evidence mapping with application to CAM". Alternative Therapies in Health and Medicine. 9 (4): 22–30. PMID 12868249. IOM Report 2005, pp. 135–136. Zeller, T.; Muenstedt, K.; Stoll, C.; Schweder, J.; Senf, B.; Ruckhaeberle, E.; Becker, S.; Serve, H.; Huebner, J. (2013-03-01). "Potential interactions of complementary and alternative medicine with cancer therapy in outpatients with gynecological cancer in a comprehensive cancer center". Journal of Cancer Research and Clinical Oncology. 139 (3): 357–365. doi:10.1007/s00432-012-1336-6. ISSN 1432-1335. PMC 11824351. PMID 23099993. S2CID 29598970. Bodeker, G.; et al. (2002). "A public health agenda for traditional, complementary, and alternative medicine". American Journal of Public Health. 92 (10): 1582–1591. doi:10.2105/AJPH.92.10.1582. PMC 3221447. PMID 12356597. Vickers, A. (2004). "Alternative cancer cures: 'Unproven' or 'disproven'?". CA – A Cancer Journal for Clinicians. 54 (2): 110–118. CiteSeerX 10.1.1.521.2180. doi:10.3322/canjclin.54.2.110. PMID 15061600. S2CID 35124492. Hróbjartsson A, Gøtzsche PC (January 2010). Hróbjartsson A (ed.). "Placebo interventions for all clinical conditions" (PDF). The Cochrane Database of Systematic Reviews. 106 (1): CD003974. doi:10.1002/14651858.CD003974.pub3. PMC 7156905. PMID 20091554. Archived from the original (PDF) on 2019-04-02. Retrieved 2019-03-25. Hróbjartsson A, Gøtzsche PC (May 2001). "Is the placebo powerless? An analysis of clinical trials comparing placebo with no treatment". The New England Journal of Medicine. 344 (21): 1594–1602. doi:10.1056/NEJM200105243442106. PMID 11372012. Kienle GS, Kiene H (December 1997). "The powerful placebo effect: fact or fiction?". Journal of Clinical Epidemiology. 50 (12): 1311–1318. doi:10.1016/s0895-4356(97)00203-5. PMID 9449934. "$2.5 billion spent, no alternative cures found". Alternative Medicine. NBCNews.com. Associated Press. 2009-06-10. Sobel, D.S. (2000). "Chapter 28: The Cost-effectiveness of Mind-body Medicine Interventions". In Mayer, E.A.; Saper, C.B. (eds.). The Biological Basis for Mind Body Interactions. Progress in Brain Research. Vol. 122. pp. 393–412. doi:10.1016/S0079-6123(08)62153-6. ISBN 978-0-444-50049-6. PMID 10737073. Beyerstein, B.L. (1999). "Psychology and 'alternative medicine' social and judgmental biases that make inert treatments seem to work". Scientific Review of Alternative Medicine. 3 (2). Archived from the original on 2011-10-12. Retrieved 2008-07-07. Rimmer, Abi (25 January 2018). "Empathy and ethics: five minutes with Edzard Ernst". BMJ. 360: k309. doi:10.1136/bmj.k309. PMID 29371199. S2CID 3511158. Laurance, Jeremy (2008-04-22). "Complementary therapies: The big con?". The Independent. London. Archived from the original on 2010-04-17. Retrieved 2010-04-23. Jerome Groopman (October 19, 2013). "The Quackish Cult of Alternative Medicine. Dr. Paul Offit's battle against charlatanism". The New Republic. Retrieved 2015-02-03. Weisleder, P (January 2010). "Unethical prescriptions: alternative therapies for children with cerebral palsy". Clinical Pediatrics. 49 (1): 7–11. doi:10.1177/0009922809340438. PMID 19628756. S2CID 19719686. Ernst, Edzard (2015). A scientist in wonderland: a memoir of searching for truth and finding trouble. Exeter, UK: Imprint Academic. pp. 404, 439, 443. ISBN 978-1-84540-777-3. Singh, Simon; Ernst, Edzard (2008). Trick or treatment: the undeniable facts about alternative medicine (1st American ed.). New York: W.W. Norton. pp. 201, 222, 259. ISBN 978-0-393-33778-5. Weber, D.O. (1998). "Complementary and alternative medicine considering the alternatives". Physician Executive. 24 (6): 6–14. PMID 10351720. Beyerstein, B.L. (2001). "Alternative medicine and common errors of reasoning". Academic Medicine. 76 (3): 230–237. doi:10.1097/00001888-200103000-00009. PMID 11242572. S2CID 41527148. Barnes, P.M.; Powell-Griner, E.; McFann, K.; Nahin, R.L. (2004). "Complementary and alternative medicine use among adults: United States, 2002" (PDF). Advance Data from Vital and Health Statistics (343): 1–19. PMID 15188733. Martin, Hélène; Debons, Jérôme (2015). "CAM and conventional medicine in Switzerland: divided in theory, united in practice". In Gale, Nicola K.; McHale, Jean V. (eds.). Routledge Handbook of Complementary and Alternative Medicine: Perspectives from Social Science and Law. London and New York: Routledge. pp. 271–291. ISBN 978-1-136-68555-2. "Traditional medicine". WHO. 2003. Archived from the original on 2008-07-27. Retrieved 2008-03-06. Castro, Arachu; Savage, Virginia; Kaufman, Hannah (2015). "Assessing equitable care for indigenous and afrodescendant women in Latin America". Revista Panamericana de Salud Pública. 38 (2): 96–109. ISSN 1020-4989. PMID 26581050. Horrobin, D.F. (1986). "Glittering prizes for research support". Nature. 324 (6094): 221. Bibcode:1986Natur.324..221H. doi:10.1038/324221a0. S2CID 28273314. Salzberg, Steven (March 26, 2018). "$142 Million For Quack Medicine Buried Inside The New 2018 Budget". Forbes. Retrieved 2019-02-14. "NCCIH Funding: Appropriations History". NCCIH. 2008-01-09. Archived from the original on 2009-06-25. Retrieved 2008-04-02. Gorski, David (April 4, 2016). "NCCIH Strategic Plan 2016–2021, or: Let's try to do some real science for a change". Science-Based Medicine. Retrieved 2019-02-14. Atwood, K.C. IV (September–October 2003). "The Ongoing Problem with the National Center for Complementary and Alternative Medicine". Skeptical Inquirer. 27 (5). Archived from the original on 2009-11-16. Retrieved 2009-11-18. Green, Saul (2001). "Stated goals and grants of the Office of Alternative Medicine/National Center for Complementary and Alternative Medicine". Scientific Review of Alternative Medicine. 5 (4): 205–207. Annual Report on CAM 2011 (PDF) (Report). Archived (PDF) from the original on 2022-10-09. Wadman, Meredith (7 December 2009). "Centre turns away from healing herbs". Nature. 462 (7274). Nature Publishing Group: 711. doi:10.1038/462711a. PMID 20010660. Gorski, David; Novella, Steven (August 20, 2014). "Clinical trials of integrative medicine: testing whether magic works?". Trends in Molecular Medicine. 20 (9): 473–476. doi:10.1016/j.molmed.2014.06.007. PMID 25150944. Coulter, I.D.; et al. (2004). "The rise and rise of complementary and alternative medicine: A sociological perspective". Medical Journal of Australia. 180 (11): 587–589. doi:10.5694/j.1326-5377.2004.tb06099.x. PMID 15174992. S2CID 15983789. Phutrakool P, Pongpirul K (January 2022). "Acceptance and use of complementary and alternative medicine among medical specialists: a 15-year systematic review and data synthesis". Systematic Reviews. 11 (1) 10. doi:10.1186/s13643-021-01882-4. PMC 8759198. PMID 35027078. Merrick, Janna (June 2003). "Spiritual Healing, Sick Kids and the Law: Inequities in the American Healthcare System". American Journal of Law & Medicine. 29 (2): 269–299. doi:10.1017/S0098858800002847. PMID 12961808. S2CID 27122896. "Definitions of Child Abuse and Neglect" (PDF). Child Welfare Information Gateway. April 2007. Archived from the original (PDF) on 11 October 2007. Retrieved 2009-02-27. Eisenberg, D.M.; et al. (1998). "Trends in alternative medicine use in the United States, 1990–1997: Results of a follow-up national survey". JAMA. 280 (18): 1569–1575. doi:10.1001/jama.280.18.1569. PMID 9820257. Patricia M. Barnes; Eve Powell-Grine; Kim McFann; Richard L. Nahin (May 27, 2004). "Complementary and Alternative Medicine Use Among Adults: United States, 2002" (PDF). Advance Data from Vital and Health Statistics. 343. CDC: 1–20. Retrieved June 1, 2021. Warner, J. (2006-07-20). "Alternative Medicine Goes Mainstream". WebMD. CBS News. Archived from the original on 2013-09-28. Retrieved 2013-03-11. Barnes, P.M.; Bloom, B.; Nahin, R.L. (2008). "Complementary and alternative medicine use among adults and children: United States, 2007". National Health Statistics Reports (12): 1–23. PMID 19361005. Archived from the original on 2022-10-09. Sir Walton: Science and Technology Committee 2000. Wujastyk 2003. "Complementary and alternative medicine (CAM)". NHS Careers website. National Health Service in England (NHS), UK Dept. of Health. Archived from the original on 2013-04-03. Retrieved 2013-03-11. Kellehear, A. (2003). "Complementary medicine: Is it more acceptable in palliative care practice?". Medical Journal of Australia. 179 (6 Supplement): S46 – S48. doi:10.5694/j.1326-5377.2003.tb05580.x. PMID 12964939. S2CID 35560507. Menefee, L.A.; Monti, D.A. (2005). "Nonpharmacologic and complementary approaches to cancer pain management". The Journal of the American Osteopathic Association. 105 (5 Supplement): S15 – S20. PMID 16368903. Archived from the original on 2008-12-01. WHO 2005. "Complementary and alternative therapies". www.cancerresearchuk.org. Cancer Research UK. July 4, 2019. Cassileth, B.R. (1996). "Alternative and complementary cancer treatments". The Oncologist. 1 (3): 173–179. CiteSeerX 10.1.1.493.434. doi:10.1634/theoncologist.1-3-173. PMID 10387984. Marty, A.T. (1999). "The Complete German Commission E Monographs: Therapeutic Guide to Herbal Medicines". Books, Journals, New Media. JAMA. 281 (19): 1852–1853. doi:10.1001/jama.281.19.1852-JBK0519-2-1. Research, Center for Drug Evaluation and (5 January 2022). "Medication Health Fraud". FDA. Archived from the original on July 1, 2010. Retrieved 21 May 2022. Research, Center for Biologics Evaluation and (6 May 2020). "Complementary and Alternative Medicine Products and their Regulation by the Food and Drug Administration". U.S. Food and Drug Administration. Archived from the original on September 5, 2019. Retrieved 21 May 2022. "Appendix E: Model Guidelines for the Use of Complementary and Alternative Therapies in Medical Practice". Complementary and Alternative Medicine in the United States. The National Academies Press. 2005. pp. 298–308. doi:10.17226/11182. ISBN 0-309-09270-1. PMID 22379647. Retrieved June 14, 2021. Hills, B. (2011-09-23) [1999]. "Fake healers: Why Australia's $1 billion-a-year alternative medicine industry is ineffective and out of control". BenHills.com. Archived from the original on 2012-03-15. Retrieved 2008-03-06. Swan, N. (2000-10-02). "Alternative Medicine – Part Three". The Health Report. Australian Broadcasting Corporation. Radio National. Archived from the original on 2008-03-06. Retrieved 2008-03-06. Roozbeh, J; Hashempur, M. H.; Heydari, M (Nov 2013). "Use of herbal remedies among patients undergoing hemodialysis". Iranian Journal of Kidney Diseases. 7 (6): 492–495. PMID 24241097. Del Prete, A; Scalera, A; Iadevaia, M. D.; Miranda, A; Zulli, C; Gaeta, L; Tuccillo, C; Federico, A; Loguercio, C (2012). "Herbal products: benefits, limits, and applications in chronic liver disease". Evid Based Complement Alternat Med. 2012: 1–19. doi:10.1155/2012/837939. PMC 3443820. PMID 22991573. Stehlin, I. (December 1996). "Homeopathy: Real medicine or empty promises?". FDA Consumer Magazine. Archived from the original on 2007-10-12. Ernst, Edzard; Smith, Kevin (2018). More harm than good?: the moral maze of complementary and alternative medicine. Cham, Switzerland: Springer. p. 18. ISBN 978-3-319-69941-7. OCLC 1019807158. Navarro, V.J.; et al. (2006). "Drug-related hepatotoxicity". New England Journal of Medicine. 354 (7): 731–739. doi:10.1056/NEJMra052270. PMID 16481640. S2CID 41793815. Lilienfeld, S.O. (2002). "Our raison d'ĕtre". Scientific Review of Mental Health Practice. 1 (1). Archived from the original on 2007-07-11. Retrieved 2008-01-28. Hughes, D. (2010-12-23). "Alternative remedies 'dangerous' for kids says report". BBC News. Archived from the original on 2010-12-24. Miller, Gabriel (2 September 2014), "Asking the Experts: Complementary and Alternative Medicine and Cancer", Medscape, retrieved 7 September 2014 Ernst, E.; et al. (2004). "Ethical problems arising in evidence based complementary and alternative medicine". Journal of Medical Ethics. 30 (2): 156–159. doi:10.1136/jme.2003.007021. PMC 1733834. PMID 15082809. Ernst, E. (1999). "Funding research into complementary medicine: The situation in Britain". Complementary Therapies in Medicine. 7 (4): 250–253. doi:10.1016/S0965-2299(99)80011-9. PMID 10709311. Ernst, .E; Pittler, M.H.; Stevinson, C.; White, A., eds. (2001). The Desktop Guide to Complementary and Alternative Medicine. Edinburgh: Mosby. ISBN 978-0-7234-3207-4. OCLC 492760852. Hall, Harriet (2019). "Science Envy in Alternative Medicine". Skeptical Inquirer. 43 (4): 21–23. Archived from the original on 2019-09-17. Retrieved 17 September 2019. Fisken, Roger A. (2014-05-19). "Teach evidence based, not alternative, medicine". BMJ. 348: g3218. doi:10.1136/bmj.g3218. ISSN 1756-1833. PMID 24839973. S2CID 206902331. Brown, D. (2009-03-17). "Scientists speak out against federal funds for research on alternative medicine". The Washington Post. Retrieved 2010-04-23. Cassileth, B.R. (1999). "Evaluating complementary and alternative therapies for cancer patients". CA – A Cancer Journal for Clinicians. 49 (6): 362–375. doi:10.3322/canjclin.49.6.362. PMID 11198952. S2CID 7889638. Derkatch, C. (2016). Bounding Biomedicine: Evidence and Rhetoric in the New Science of Alternative Medicine. University of Chicago Press. p. 215. ISBN 978-0-226-34584-0. Retrieved March 18, 2023. Sampson W, Atwood K (2005). "Propagation of the absurd: demarcation of the absurd revisited". Med. J. Aust. 183 (11–12): 580–581. doi:10.5694/j.1326-5377.2005.tb00040.x. PMID 16336135. S2CID 43272637. Barrett, S. (2004-02-10). "Be Wary of "Alternative" Health Methods". Quackwatch. Archived from the original on 2008-05-09. Retrieved 2008-03-03. "NCAHF Mission Statement". National Council Against Health Fraud (NCAHF) website. 2009-11-30. Retrieved 2013-03-11. Steele, F.R. (1996). "Book review: The Demon-Haunted World: Science as a Candle in the Dark by Carl Sagan". Nature Medicine. 2 (9): 1042. doi:10.1038/nm0996-1042. S2CID 41229701. Hines, T. (2003). Pseudoscience and the Paranormal (2nd ed.). Amherst, NY: Prometheus Books. ISBN 978-1-57392-979-0. Sampson, W. (2001). Grollman, A.P. (ed.). "The need for educational reform in teaching about alternative therapies". Academic Medicine. 76 (3): 248–250. doi:10.1097/00001888-200103000-00011. PMID 11242574. Coulter et al. 2004. Kent 1997. Sagan 1996. Acharya, D.; et al. (2008). Indigenous Herbal Medicines: Tribal Formulations and Traditional Herbal Practices. Jaipur, India: Aavishkar Publishers. p. 440. ISBN 978-81-7910-252-7. IOM Report 2005, p. 146. Xiaorui Zhang. "Traditional Medicines: Definitions". WHO Website. Archived from the original on 2013-09-27. Retrieved 2012-11-11. Extracted from WHO 2000. IOM Report 2005, pp. 17–19. Zollman, C.; et al. (1999). "What is complementary medicine?". ABC of complementary medicine. BMJ. 319 (7211): 693–696. doi:10.1136/bmj.319.7211.693. PMC 1116545. PMID 10480829. Fonfa, Anne E. (September 1, 2017). "Patient Perspectives: Barriers to Complementary and Alternative Medicine Therapies Create Problems for Patients and Survivors". Integrative Cancer Therapies. 6 (September 2007): 297–300. doi:10.1177/1534735407306598. PMID 17761643. Ernst, E. (2005). "The efficacy of herbal medicine -- An overview". Fundamental & Clinical Pharmacology. 19 (4): 405–409. doi:10.1111/j.1472-8206.2005.00335.x. PMID 16011726. S2CID 2327655. Dawkins, R. (2003). Menon, L. (ed.). A Devil's Chaplain: Selected Essays. London: Weidenfeld & Nicolson. ISBN 978-0-7538-1750-6. (p. 180 in 2004 US ed. ISBN 0618335404). Holloway, R. (2003-02-14). "A callous view". Books. The Guardian. London. Archived from the original on 2010-04-11. Retrieved 2010-04-23. Ernst, E. (1996). "The ethics of complementary medicine". Journal of Medical Ethics. 22 (4): 197–198. doi:10.1136/jme.22.4.197. PMC 1376996. PMID 8863142. Butler, K.; et al. (1992). A Consumer's Guide to "Alternative Medicine": A Close Look at Homeopathy, Acupuncture, Faith-healing and Other Unconventional Treatments. Consumer Health Library. Buffalo, New York: Prometheus. ISBN 978-0-87975-733-5. Ernst, E. (2011-11-08). "Alternative medicine remains an ethics-free zone". The Guardian. London. Archived from the original on 2013-01-28. Hall, Harriet (September 2015), "Evidence: "It Worked for My Aunt Tillie" is Not Enough", Skeptic, Volume 20, Number 3, retrieved November 22, 2015 Ernst, Edzard (2011). "Conflicts of Interest in Alternative Medicine". Skeptical Inquirer. 35 (4). Gorski, David (16 November 2009). "Conflicts of interest in science-based medicine". Science-Based Medicine. Hall, Harriet A. (27 April 2011). "Conflicts of interest". Science-Based Medicine. |
参考文献 バレット、スティーブン、ホール、ハリエット、バラッツ、ロバート S.、ロンドン、ウィリアム M.、クローガー、マンフレッド (2013). 消費者の健康:賢明な決断のためのガイド (第 9 版). ニューヨーク: McGraw-Hill. pp. 34–35, 134, 137. ISBN 978-0-07-802848-9. OCLC 758098687. アンジェル, M.; 他 (1998). 「代替医療―未検証かつ規制されていない治療法のリスク」 (PDF). ニューイングランド・ジャーナル・オブ・メディシン. 339 (12): 839–841. CiteSeerX 10.1.1.694.9581. doi:10.1056/NEJM199809173391210. PMID 9738094. 2022年10月9日時点のオリジナルからアーカイブ (PDF). シャピロ, ローズ (2010). 『騙される人々:代替医療が我々を愚かにする仕組み』. ランダムハウス. p. 8. ISBN 978-1-4090-5916-5. さらなるブランド変更により、「統合医療」という概念が生まれた。 ボンバルディエリ、D; イーストホープ、G (2000年10月). 「正統医療と代替医療の収斂:理論的考察と実証的検証」. Health. 4 (4): 479–494. doi:10.1177/136345930000400404. S2CID 71900519. Shuval, Judith T.; Averbuch, Emma (2012). 「イスラエルにおける補完代替医療」『イスラエル保健政策研究ジャーナル』1巻7号、7頁。doi:10.1186/2045-4015-1-7。PMC 3424827。PMID 22913721。 フリードマン、デイヴィッド・H.(2011年7月-8月)。「ニューエイジ医療の勝利」『アトランティック』 アトランティック誌。2015年5月10日にオリジナルからアーカイブ。2015年6月6日に取得。 ゴルスキー、デイヴィッド(2011年8月15日)。「統合医療」:専門分野ではなくブランドだ。sciencebasedmedicine.org。(2022年3月25日取得)。 「欧州議会及び理事会指令2004/24/EC」. 欧州連合官報. 2004年4月30日. サンプソン, ウォレス (1995年6月). 「代替医療運動の台頭における反科学的傾向」 . ニューヨーク科学アカデミー紀要. 775 (1): 188–197. doi:10.1111/j.1749-6632.1996.tb23138.x. ISSN 0077-8923. PMID 8678416. S2CID 2813395. コラタ、ジーナ(1996年6月17日)、「医療の周辺で、未検証療法が繁栄する」、『ニューヨーク・タイムズ』、2015年12月22日閲覧 全米科学財団(2002年4月)。「第7章:科学技術:公衆の態度と理解:SFと疑似科学」. 全米科学財団. 2007年2月18日時点のオリジナルからアーカイブ. 2023年3月15日閲覧. IOM報告書 2005, p. 19. ハインズ、テレンス(2003)。『疑似科学と超常現象』(第2版)。ニューヨーク州アマースト:プロメテウス・ブックス。ISBN 978-1-57392-979-0。; サンプソン、ウォルター(2001年3月)。「代替療法教育における教育改革の必要性」。『アカデミック・メディシン』。76巻3号: 248–250頁。doi:10.1097/00001888-200103000-00011。PMID 11242574。; Coulter, Ian D; Willis, Evan M (2004年6月). 「補完代替医療の台頭と拡大:社会学的視点」. Medical Journal of Australia. 180 (11): 587–589. doi:10.5694/j.1326-5377.2004.tb06099.x. PMID 15174992. S2CID 15983789.;Sagan 1996 Kent Heather (1997). 「代替医療への患者の関心の高まりを無視すれば危険だ―医師は警告する」. カナダ医師会雑誌. 157 (10): 1427–1428. PMC 1228476. PMID 9371077. Goldrosen MH, Straus SE (2004). 「補完代替医療:免疫学的効果に関する証拠の評価」. ネイチャー・レビューズ・イミュノロジー. 4 (11): 912–921. doi:10.1038/nri1486. PMID 15516970. S2CID 11708302. ハリソン内科学 2015, p. 1, chpt. 14-E. 「補完医療 – 代替医療システム」. WebMD. 2014年1月14日. 2015年6月1日にオリジナルからアーカイブ. 2015年6月4日に閲覧. 「米国における補完代替医療の利用状況」. 国立補完統合医療センター. 2015年4月7日. 2015年6月1日にオリジナルからアーカイブ. 2015年6月4日に閲覧. Beyerstein BL (2001). 「代替医療と一般的な推論の誤り」. Academic Medicine. 76 (3): 230–237. doi:10.1097/00001888-200103000-00009. PMID 11242572. S2CID 41527148. サックス, M. (1992). 「序論」. サックス, M. (編). 『英国における代替医療』. オックスフォード: クラレンドン・プレス. pp. 1–21. ISBN 978-0-19-827278-6. IOM報告書 2005, p. 19. 「補完・代替・統合医療:名称の意義とは?」米国保健福祉省(US HHS)国立衛生研究所(NIH)傘下国立補完統合医療センター(NCCIH)。2002年5月。2005年12月8日時点のオリジナルからアーカイブ。2022年12月1日取得。 サー・ウォルトン:科学技術委員会 2000、第1章:序論。 コペルマン 2004。 ヴィーランドら 2011。 アスティン、J.A.;他(1998)。「主流の医師による補完代替医療の取り入れに関するレビュー」。JAMA Internal Medicine。158 (21): 2303–2310。doi:10.1001/archinte.158.21.2303. PMID 9827781. Pelletier, K.R. 他 (1997). 「管理医療、保険会社、病院提供者による補完代替医療の統合と償還の現状動向」. American Journal of Health Promotion. 12 (2): 112–122. doi:10.4278/0890-1171-12.2.112. PMID 10174663. S2CID 46772634. IOM報告書2005年、17頁、196–252頁。 ホワイトハウス補完代替医療政策委員会スタッフ;米国保健社会福祉省スタッフ(2002年3月)。「米国における補完代替医療(CAM)の概要:近年の歴 史、現状、および将来展望」。ホワイトハウス補完代替医療政策委員会最終報告書(報告書) 米国政府印刷局。ISBN 978-0-16-051476-0。2013年2月15日にオリジナルからアーカイブ。第2章は2011年8月25日にアーカイブ。 Ernst, E. (1995). 「補完医療:一般的な誤解」. 王立医学会誌. 88 (5): 244–247. PMC 1295191. PMID 7636814. 補完医療とは、主に従来の主流医療の外側にある医療と定義される。 ジョイス、C.R.B. (1994). 「プラセボと補完医療」. ランセット. 344 (8932): 1279–1281. doi:10.1016/S0140-6736(94)90757-9. PMID 7967992. S2CID 36724993. メイ、J.(2011)。「統合医療とは何か?」。BMJ。343: d4372。doi:10.1136/bmj.d4372。PMID 21750063。S2CID 206893456。 「がん治療における補完代替医療(PDQ®):がん治療における補完代替医療に関する質問と回答」. NCIウェブサイト. 医師用データクエリ(PDQ). 米国国立がん研究所(NCI), 米国国立衛生研究所(NIH). 2012年12月15日にオリジナルからアーカイブ. 2012年12月11日に閲覧. ボルカン, J. (2012). 「イスラエルと西洋世界における補完代替医療」. Israel Journal of Health Policy Research. 1 (1) 8. doi:10.1186/2045-4015-1-8. PMC 3424836. PMID 22913745. 「補完代替医療(CAM)とは何か?」. 国立補完代替医療センター. 2005年12月8日時点のオリジナルからアーカイブ. 2006年7月11日に閲覧. Zeller, T.; Muenstedt, K.; Stoll, C.; Schweder, J.; Senf, B.; Ruckhaeberle, E.; Becker, S.; Serve, H.; Huebner, J. (2013-03-01). 「総合がんセンターにおける婦人科がん外来患者における補完代替医療とがん治療の潜在的な相互作用」. Journal of Cancer Research and Clinical Oncology. 139 (3): 357–365. doi:10.1007/s00432-012-1336-6. ISSN 1432-1335. PMC 11824351. PMID 23099993. S2CID 29598970. Ben-Arye, Eran; Polliack, Aaron; Schiff, Elad; Tadmor, Tamar; Samuels, Noah (2013-12-01). 「がん治療中の非ハーブ系栄養補助食品使用に関する患者への助言:医師と患者のコミュニケーションの必要性」 . Journal of Pain and Symptom Management. 46 (6): 887–896. doi:10.1016/j.jpainsymman.2013.02.010. ISSN 1873-6513. PMID 23707384. Li, B; Forbes, T.; Byrne, J. (2018). " 統合医療か、それとも浸透する疑似科学か?」。外科医。16 (5): 271–277. doi:10.1016/j.surge.2017.12.002. PMID 29305045. S2CID 19580427. 「補完代替医療」。英国国民保健サービス. 2022年3月1日. 2023年5月6日閲覧. 「補完療法と代替療法(CAM)の違い」. 英国がん研究機構. 2022年4月4日. 2023年5月6日閲覧. 「がん患者向け補完代替医療」. 米国疾病予防管理センター. 2022年6月9日. 2023年5月6日閲覧。 Belloni, Silvia; Bonucci, Massimo; Arrigoni, Cristina; Dellafiore, Federica; Caruso, Rosario (2023-01-01). 「がん関連疲労改善のための補完統合医療に関するシステマティックレビューの系統的レビューと統合メタ分析」. 臨床治療学。45 (1): e54 – e73。doi:10.1016/j.clinthera.2022.12.001。ISSN 0149-2918。PMID 36566113。S2CID 255049739。 Greenlee, Heather; Zick, Suzanna M.; Rosenthal, David; Cohen, Lorenzo; Cassileth, Barrie; トリパシー、デブ(2015年3月)。「統合腫瘍学 ― より良い患者ケアには確固たる科学が必要だ」。ネイチャー・レビューズ・キャンサー。15 (3): 165。doi:10.1038/nrc3822-c1。ISSN 1474-1768。PMID 25693833。S2CID 8053861. ゴルスキー, D. (2010-08-03). 「鍼治療への軽信がニューイングランド・ジャーナル・オブ・メディシンに浸透する」. サイエンス・ベースド・メディシン. 2013-09-28にオリジナルからアーカイブ. コールドウェル, エリザベス・フランセス (2017-07-03) 。「偽科学教育?ホメオパシー教育に対するマスメディアによる正当性否定」。『科学としての文化』。26巻3号:380–407頁。doi: 10.1080/09505431.2017.1316253。ISSN 0950-5431。S2CID 151442812。 ロバート・トッド・キャロル. 統合医療. 懐疑主義者の辞典 エルゼビア・サイエンス (2002). 「著者インタビュー(エザード・エルンスト、『補完代替医療デスクトップガイド』編集者)」。ハーコート・インターナショナル。2002年3月2日にオリジナルからアーカイブ。 キャシレス, B.R.; 他 (2004). 「 がんに対する補完代替療法」『The Oncologist』9巻1号:80–89頁。doi:10.1634/theoncologist.9-1-80。PMID 14755017。S2CID 6453919。 タイアマン、スティーブン(2011-05-01)。「補完代替医療における価値観」『 医学、医療、哲学。14 (2): 209–217. doi:10.1007/s11019-010-9297-5. ISSN 1572-8633. PMID 21104324. S2CID 32143622. WHO伝統的・補完医療に関するグローバル報告書 (PDF). 世界保健機関(報告書)。ジュネーブ。2019年。ISBN 978-92-4-151543-6。2022年7月29日時点のオリジナルからアーカイブ(PDF)。2022年12月6日に取得。 Gorski, David (2014年9月29日). 「偽科学の学問的浸透:クリーブランド・クリニック、ジョージ・ワシントン大学、そして医学界への偽科学の継続的浸透」. Science-Based Medicine. 2025年4月8日に取得。 「統合医療試験の説明」. 米国専門医認定機構. 2021年7月16日. 2022年3月11日取得. ウェイク, ゲトゥ・エンギダ; フィティエ, ギルマ・ウォギー (2022年4月29日). 「エチオピア、デブレ・ベルハン町の公的医療機関で妊婦健診を受ける母親における漢方薬利用の規模と決定要因」 . フロントィアーズ・イン・パブリック・ヘルス. 10 883053. Bibcode:2022FrPH...1083053W. doi:10.3389/fpubh.2022.883053. ISSN 2296-2565. PMC 9098925. PMID 35570953。伝統医療とは、現代医学が普及する以前に存在した健康の保護と回復の方法と定義される。これは世界のほぼ全ての国で見られる、医療にお いて過小評価されている分野である。伝統医療は、健康の維持、及び身体的・精神的疾患の予防、診断、改善、治療に用いられてきた。 Che, C.-T.; George, V.; Ijinu, T.P.; Pushpangadan, P.; Andrae-Marobela, K. (2017). 「伝統医学」. 薬用植物学. Elsevier. pp. 15–30. doi:10.1016/B978-0-12-802104-0.00002-0. ISBN 978-0-12-802104-0. 伝統医学とは、 世界保健機関(WHO)の定義によれば、伝統医学とは、健康の維持、ならびに身体的・精神的疾患の予防、診断、改善、治療のために用いられる、様々な文化 に固有の理論、信念、経験に基づく知識、技術、実践の総体である。説明可能か否かを問わない。一部の伝統医学体系は、膨大な文献や理論的概念・実践技術の 記録によって支えられている。他方、口頭伝承によって世代から世代へと受け継がれるものもある。 伝統医療とその倫理的含意に関する予備報告書草案。パリ:ユネスコ国際生命倫理委員会。2010年。p. 5。2023年3月29日取得。伝統医療は類推的推論と疾病・健康への全体論的アプローチに基づくのに対し、現代医学は科学的知識に依拠し、証拠に基づいている。 李福双、翁景可 (2017年7月31日). 「現代的アプローチによる伝統的漢方薬の解明」 . Nature Plants. 3 (8): 17109. Bibcode:2017NatPl...317109L. doi:10.1038/nplants.2017.109. ISSN 2055-0278. PMID 28758992. S2CID 2127457. これらの総合的な伝統的漢方処方の初期開発は現代科学より前であったが、その過程は数千年にわたる表現型に基づく個別化された臨床試験に基づいていた。一 方、 病気の症状に関する緻密な記述や体系的な医学理論も、何世代にもわたる漢方医によって記録されてきた。それらは多様な薬用植物の治療特性と、特定の症状を 治療する有用性を関連付けている。しかし、伝統医療体系の基礎概念のほとんど——例えば、中医学における陰と陽、寒と熱の概念——は、生理学や分子生物学 の言語で表現される正常状態や病態の現代的な記述とは切り離されている。安全性、有効性、作用メカニズムに関する現代的な科学的・臨床的証拠の欠如が、こ うしたホリスティックな漢方薬の処方が、その文化圏の外で受け入れられることをさらに妨げている。 Jansen, C.; Baker, J.D.; Kodaira, E.; Ang, L.; Bacani, A.J.; Aldan, J.T.; Shimoda, L.M.N.; Salameh, M.; Small-Howard, A.L.; Stokes, A.J.; Turner, H.; Adra, C.N. (2021年3月). 「動きのある医学:西洋医療への伝統医学の統合のための機会、課題、およびデータ分析に基づく解決策」. Journal of Ethnopharmacology. 267 113477. doi:10.1016/j.jep.2020.113477. ISSN 0378-8741。PMC 7577282。PMID 33098971。伝統的な文化やルーツ文化の外で採用される場合、伝統医学は、西洋の専門医療機関、保険会社、医療制度などによって、代替医療(AM) の一形態として分類されることが多い。これは問題を引き起こす。規制の欠如(例えば米国では、こうした手法はせいぜい栄養補助食品市場に追いやられ、 FDAの規制範囲外となる)や、本来の処方や投与スケジュール、投与方法、適応症への忠実性の欠如につながるのだ。 Tabish, Syed Amin (2008). 「Complementary and Alternative Healthcare: Is it Evidence-based?」. International Journal of Health Sciences. 2 (1): V–IX. ISSN 1658-3639. PMC 3068720. PMID 21475465. 補完代替医療(CAM)とは、現在、従来の医学の一部とは見なされていない多様な医療・健康システム、実践、製品群を指す。安全性と有効性が証明された CAMの実践や療法が「主流」の医療実践として受け入れられるにつれ、CAMと見なされる実践のリストは絶えず変化している...代替医療は、一般的に 「補完代替医療」という包括的用語の下で補完医療と共に分類される。補完医療とは、伝統的な西洋医学(または対症療法)を補完し、従来の医療と併用される 療法を指す。一方、代替医療は従来の医療に代わって用いられる。代替医療とは、伝統的な医療に代わる治療アプローチであり、疾病の治療や緩和に用いられ る。 Fontanarosa, P.B.; et al. (1998). 「Alternative medicine meets science」. JAMA. 280 (18): 1618–1619. doi:10.1001/jama.280.18.1618. PMID 9820267. S2CID 5485601. ベレスフォード, M. J. (2010年4月15日). 「医学的還元主義:偉大な哲学者たちからの教訓」. QJM. 103 (9). オックスフォード大学出版局 (OUP): 721–724. doi:10.1093/qjmed/hcq057. ISSN 1460-2725. PMID 20395240. 残念ながら、「ホリスティック医療」という用語は代替療法家によってある意味で乗っ取られており、しばしば誤って従来の医療と対立するものと考えられてい る。 Zucker, Arthur (1979年1月). 「還元主義とホリスティック医療」 . ジャーナル・オブ・ソーシャル・アンド・バイオロジカル・システムズ. 2 (1). エルゼビア BV: 39–42. doi:10.1016/0140-1750(79)90019-8. ISSN 0140-1750. オフイット、P. (2013) 。魔法を信じますか?:代替医療の理屈と非理屈。ハーパーコリンズ。ISBN 978-0-06-222296-1。英国では、オフイット、ポール博士 (2013)『Killing Us Softly: The Sense and Nonsense of Alternative Medicine』HarperCollins Publishers. ISBN 978-0-00-749173-5. Diamond, J. quoted in Dawkins 2003. (p. 36 in 2004 US ed. ISBN 0618335404). IOM 報告書 2005、14-20 ページ。 Sointu 2012、13 ページ。 Nissen, N.; et al. (2013). 「代替療法および補完療法の研究:この分野のマッピング」. Medical Anthropology. 32 (1): 1–7. doi:10. 1080/01459740.2012.718016. PMID 23206171. S2CID 31843233. キャロル、R.T.(2011-05-14)。「補完医療」。『懐疑主義辞典』(オンライン版)。2013-09-27にオリジナルからアーカイブされた。2013-09-27. ノベラ, S. (2010-08-04). 「ニューイングランド・ジャーナル・オブ・メディシンにおける鍼治療の疑似科学」. 科学に基づく医学. 2013-09-28にオリジナルからアーカイブされた。 ジェフリー, ニック (2015). 「代替医療など存在しない」. 論説. 小動物診療ジャーナル. 56 (12): 687–688. doi:10.1111/jsap.12427. ISSN 1748-5827. PMID 26735773. O'Connor 1995, p. 2. Sarris, J.; et al. (2010). 臨床自然療法:実践のためのエビデンスに基づくガイド。エルゼビア・ヘルスサイエンス。ISBN 978-0-7295-7926-1。 Jagtenberg T、エヴァンス S、グラント A、ハウデン I、ルイス M、シンガー J (2006)。「エビデンスに基づく医療と自然療法」。J Altern Complement Med. 12 (3): 323–328. doi:10.1089/acm.2006.12.323. PMID 16646733. 2018年2月22日にオリジナルからアーカイブ。2017年5月13日に取得。 Ernst E (2001). 「補完代替医療の人気の高まり:その理由と予防接種への影響」. Vaccine. 20 (Suppl 1): S89 – S93. doi:10.1016/S0264-410X(01)00290-0. PMID 11587822. 「自然療法医学」. アメリカ癌協会. 2008年11月1日. 2015年4月3日にオリジナルからアーカイブ. 2010年11月20日に閲覧. ハーネマン 1833, pp. iii, 48–49. Ernst, E. (2002). 「ホメオパシーに関する系統的レビューの系統的レビュー」. British Journal of Clinical Pharmacology. 54 (6): 577–582. doi:10.1046/j.1365-2125.2002.01699.x. PMC 1874503. PMID 12492603. 下院:科学技術委員会 (2010年2月22日). 証拠検証2:ホメオパシー (PDF) (報告書). HC 45, 2009–2010年会期第4回報告書. ロンドン: 文房具局. シャン、アイジン; ヒューウィラー=ミュンテナー、カリン; ナルテイ、リンダ; ユニ、ピーター; ドーリグ、ステファン; スターン、ジョナサン AC; プースナー、ダニエル; エガー、マティアス (2005), "ホメオパシーの臨床効果はプラセボ効果か?ホメオパシーとアロパシーのプラセボ対照試験の比較研究」、『ランセット』366巻9487号、 726–732頁、doi:10.1016/S0140-6736(05)67177-2、PMID 16125589、S2CID 17939264 「ホメオパシー:入門」。背景情報。NCCIH。2013年[2009年]。2013年10月15日にオリジナルからアーカイブ。 Sampson, W. (1995). 「『代替医療』運動の台頭における反科学的傾向」。ニューヨーク科学アカデミー紀要。775 (1): 188–197. doi:10.1111/j.1749-6632.1996.tb23138.x. PMID 8678416. S2CID 2813395. ベイヤーシュタイン, B.L.; ウォレス・サンプソン (1996). 「中国における伝統医学と疑似科学:第2回CSICOP代表団報告書(第1部)」。『懐疑的探求者』20巻4号。2009年10月4日時点のオリジナルからアーカイブ。 呂桂珍、ニードハム・ジョセフ(1980)。『天の鉗子:鍼灸の歴史と理論』 ケンブリッジ及びニューヨーク:ケンブリッジ大学出版局。ISBN 978-0-521-21513-8。 マシオシア、ジョバンニ(1995)。『中医学における舌診』。シアトル:イーストランド出版。ISBN 978-0-939616-19-0。 カミリア・マトゥク(2006) 。「身体を見る:古代中国と西洋の医学図解の相違」 (PDF)。バイオコミュニケーション誌。32 (1)。2022年10月9日にオリジナルからアーカイブ (PDF)。 デシュパンデ、ヴィジャヤ (1987年1月)。「インドと中国間における中世の錬金術および化学思想の伝播」 (PDF)。インド科学史ジャーナル。22巻1号:15–28頁。PMID 11622483。2015年5月5日にオリジナル(PDF)からアーカイブ。 ウジャスティク 2003, p. xviii. ミシュラ 2004, p. 8. ダスグプタ、アミタヴァ; ハメット=ステーブラー、キャサリン・A(2011)。『ハーブサプリメント:有効性、毒性、西洋薬との相互作用、臨床検査への影響』。ホボーケン (ニュージャージー州):ジョン・ワイリー・アンド・サンズ。pp. 202–205。ISBN 978-0-470-43350-8。 ヴァリアサン、M.S.(2006)。「 アーユルヴェーダ:秩序を立て直す」 (PDF). ゲスト論説. カレント・サイエンス. 90 (1): 5–6. 2022年10月9日時点のオリジナルからアーカイブ (PDF). 疾病予防管理センター (CDC) (2004年7月9日). 「アーユルヴェーダ薬に関連する鉛中毒 – 5州、2000–2003年」. 疾病死亡週報. 53 (26) : 582–584. PMC 2768057. PMID 15241300. Saper, R.B.; et al. (2008). 「インターネット経由で販売される米国及びインド製造のアーユルヴェーダ医薬品中の鉛、水銀、ヒ素」. JAMA. 300 (8): 915–923. doi:10.1001/jama.300.8.915. PMC 2755247. PMID 18728265. Hall, Harriet (2017-12-14). 「アーユルヴェーダ:古代の迷信であって、古代の知恵ではない」. Skeptical Inquirer. 2018年2月1日取得。 Breeher L, Mikulski MA, Czeczok T, Leinenkugel K, Fuortes LJ (2015年4月6日). 「アーユルヴェーダ薬の消費者における鉛中毒の集団発生」. International Journal of Occupational and Environmental Health. 21 (4): 303–307. doi:10.1179/2049396715Y.0000000009. PMC 4727589. PMID 25843124. Sagan 1996. Rosa L、Rosa E、Sarner L、バレット S (1998年4月)。「 治療的タッチを詳しく見てみよう」。JAMA。279 (13): 1005–1010. doi:10.1001/jama.279.13.1005. PMID 9533499. アブドゥラ、サラ (1999年5月13日)。「植物療法 – 優れた科学か、それとも大ビジネスか?ネイチャー. doi:10.1038/news990513-8. 科学に基づく医療は、統制された研究、証明、証拠、統計的有意性、安全性を重視するが、これらは「代替医療」に取って代わられつつある。代替医療とは、逸 話、噂、風評、でたらめを寄せ集めた退行的な混合物だ。..代替医療あるいは補完医療の中で、おそらく最も商業的に成功し広く利用されている分野が「植物 療法」だ。これらは錠剤、粉末、エリキシル剤、つまりハーブ療法として知られ、ほとんどの国で健康食品店や薬局を通じて「栄養補助食品」として販売されて いる。.. これらの治療法のうち、軽度から中程度の健康効果があると証明されているものはごく一部に過ぎない。ではなぜ、裕福で、それ以外では合理的で、高学歴の人 々(これが平均的な利用者のプロフィールだ)が、これほどまでに植物療法を渇望するのか?人々は依然として、「自然」は良くて安全だと信じている。それと は反対の証拠が山ほどあるにもかかわらずだ。人体に関して言えば、「自然」という言葉は意味をなさない。同様に、成分基準すら満たさない物質を摂取するこ とに、いったい何が安全だというのか? De Smet, Peter A.G.M. (1997年12月). 「医療における植物由来薬物とハーブ医薬品の役割」. Drugs. 54 (6) : 801–840. doi:10.2165/00003495-199754060-00003. PMID 9421691. S2CID 46970414. 「新たな政府調査によると、成人の38%、子供の12%が補完代替医療を利用している」 」 (プレスリリース). NIHニュース. メリーランド州ベセスダ: 国立補完統合医療センター. 2008年12月10日. 2015年4月7日にオリジナルからアーカイブ. 2015年6月4日に閲覧. ピアース, アリソン; シンプソン, ニール (1998年3月). 「小児科医のための補完医療ガイド」. 現代小児科学. 8 (1): 62–67. doi:10.1016/S0957-5839(98)80061-4. 「信仰治療 – 治療決定について」. アメリカ癌協会. 2009年6月15日. 2010年2月12日にオリジナルからアーカイブ. 2018年5月28日閲覧。 Aviles, Jennifer M.; Whelan, Sr Ellen; Hernke, Debra A.; Williams, Brent A.; Kenny, Kathleen E.; O'Fallon, W. Michael; Kopecky, Stephen L. (2001年12月). 「冠動脈ケア病棟患者における執り成しの祈りと心血管疾患の進行:無作為化比較試験」. Mayo Clinic Proceedings. 76 (12): 1192–1198. doi:10.4065/76.12.1192. PMID 11761499. S2CID 7300728. 「エネルギー医学:概要」. 背景資料. NCCIH. 2005 [2004]. 2016年5月22日にオリジナルからアーカイブ. 『偽医療:20世紀アメリカにおける健康詐欺との闘いの歴史』, エリック・W・ボイル, [1] Whorton, James (2003). 「カウンターカルチャーの癒し:アメリカにおける代替医療の簡史」. PBS Frontline. 2022-03-25 取得. Coulter, Ian D.; Willis, Evan M. (2004-06-07). 「補完代替医療の台頭と拡大:社会学的視点」. オーストラリア医学雑誌。180 (11): 587–589. doi:10.5694/j.1326-5377.2004.tb06099.x. ISSN 0025-729X. PMID 15174992. S2CID 15983789. Whorton, James C. (2002). 自然療法:アメリカにおける代替医療の歴史. オックスフォード大学出版局. ISBN 978-0-19-534978-8. 「代替療法:序論」. www.pbs.org. PBS フロントライン. 2003年11月3日. ウォリス、クローディア (1991年11月4日). 「特集記事:ニューエイジ医療が広まる理由」. タイム. 第138巻、第18号. ISSN 0040-781X. 2022年3月25日取得。 アンカーバーグ、ジョン;ウェルドン、ジョン(1996)。『ニューエイジ医学』、『ニューエイジ信仰事典』。ハーベスト・ハウス出版社。470–508頁。ISBN 978-1-56507-160-5。 スミス、T(1983)。「代替医療」。British Medical Journal (Clinical Research Ed.) 287 (6388): 307–308. doi:10.1136/bmj.287.6388.307. PMC 1548588. PMID 6307462. 現代英国で数少ない成長産業の一つが代替医療である。瞑想から頭蓋骨に穴を開けて酸素を取り込む治療法まで、その効能を説く書籍、記事、ラジオ・テレビ番 組が絶え間なく流れ続けている。 クルーガー、ヘレン (1974). 『他の治療者、他の治療法:代替医療ガイド』. ボブス・メリル. ISBN 978-0-672-51708-2. ロー、ドナルド(1975)。『代替医療ガイド』。ターンストーン・プレス。ISBN 978-0-85500-107-0。 ウィニック、T.A.(2005)。「偽医療から『補完』医療へ:代替療法に直面するアメリカ医学界」『社会問題』52巻1号:38-61頁。doi:10.1525/sp.2005.52.1.38。JSTOR 10.1525/sp.2005.52.1.38。 ウィニック, T.A. (2009). 「偽医療から「補完」医療へ:代替療法に直面するアメリカ医学界」. コンラッド, P. (編). 『健康と病気の社会学』 (第8版)。ニューヨーク:ワース。pp. 261–277。ISBN 978-1-4292-0558-0。 ヤング、J.H.(1998)。「国立衛生研究所における代替医療局の発展、1991–1996」。医学史紀要. 72 (2): 279–298. doi:10.1353/bhm.1998.0110. PMID 9628052. S2CID 26685737. フレクナー, A. (1910). 『米国とカナダの医学教育 カーネギー財団への報告書』(報告書). ボストン: D. B. アップダイク, メリーマウント・プレス. CFAT: フレクナー報告書より入手可能 2013-11-05 ウェイバックマシンにアーカイブ ルドメラー, K.M. (2010). 「解説: フレクナー報告書を理解する」(PDF). アカデミック・メディシン. 85 (2): 193–196. doi:10.1097/ACM.0b013e3181c8f1e7. PMID 20107341. 2022-10-09にオリジナルからアーカイブ (PDF). ビアンコ、C.(2000年4月)。「医師になる仕組み:医学部のカリキュラム」。HowStuffWorksウェブサイト。2013年10月5日にオリジナルからアーカイブ。 「スタンフォード大学の医学カリキュラム」. スタンフォード大学ウェブサイト. スタンフォード大学医学部. 2013年5月9日にオリジナルからアーカイブ. 2013年1月26日に取得. 「医学生教育プログラム:カリキュラム概要」. イエール大学ウェブサイト. イエール大学医学部. 2013年10月4日にオリジナルからアーカイブ. Snyderman, R.; 他 (2002). 「統合医療:医療をその根源へ戻す」. JAMA Internal Medicine. 162 (4): 395–397. doi:10.1001/archinte.162.4.395. PMID 11863470. S2CID 46177131. バーマン、B.M.(2001)。「補完医療と医学教育」。BMJ。322 (7279): 121–132。doi:10.1136/bmj.322.7279.121。PMC 1119400。PMID 11159555。 「コクラン補完代替医療分野」. メリーランド大学ウェブサイト. メリーランド大学医学部統合医療センター. 2013年9月28日時点のオリジナルからアーカイブ. 「統合医療センター」. メリーランド大学ウェブサイト. メリーランド大学医学部. 2010年3月23日時点のオリジナルからアーカイブ. 「医学博士(MD)の職業」. MedlinePlus. 米国国立医学図書館、NIH. 2011年2月3日. 2013年1月27日にオリジナルからアーカイブ. 2012年12月20日に取得. Kent, H. (1997). 「代替医療への患者の関心の高まりを無視すれば危険だ - 医師への警告」 . カナダ医師会雑誌. 157 (10): 1427–1428. PMC 1228476. PMID 9371077. Goldrosen, M.H.; et al. (2004). 「補完代替医療:免疫学的効果に関する証拠の評価」. 展望. ネイチャー・レビューズ・イミュノロジー. 4 (11): 912–921. doi:10.1038/nri1486. PMID 15516970. S2CID 11708302. IOM報告書2005年。 サリス、J.(2012)。「補完医療の証拠評価における現在の課題」(PDF)。オーストラリア医学雑誌。196 (5) : 310–311. doi:10.5694/mja11.10751. PMID 22432660. S2CID 31044567. 2022-10-09にオリジナルからアーカイブされた (PDF). Alcock, J. (1999). 「代替医療と信念の心理学」. 代替医療の科学的レビュー。3 (2)。 Ernst, E. 「2005年ヘルスウォッチ賞:エドザード・エルンスト教授:補完医療:良い面、悪い面、そして醜い面」。英国:ヘルスウォッチ。2013年10月16日にオリジナルからアーカイブ。 Ernst, E. (2011). 「CAMのどれほどが研究的証拠に基づいているのか?」。エビデンスに基づく補完代替医療. 2011 676490. doi:10.1093/ecam/nep044. PMC 3136881. PMID 19465405. 「代替医療: 自らを癒す」。エコノミスト。2011年5月19日。pp. 83–84。2011年5月22日にオリジナルからアーカイブ。 Ernst, E. (2008). 「プラセボ及びその他の非特異的効果」。Ernst, E. (編)『癒し、誇大宣伝、それとも害?補完代替医療の批判的分析』。インプリント・アカデミック、ソシエタス刊。ISBN 978-1-84540-118-4。 カッツ、D.L.ほか(2003)。「補完代替医療のエビデンス基盤:CAMへの応用を伴うエビデンスマッピングの方法」。『健康と医療における代替療法』。9巻4号:22–30頁。PMID 12868249。 IOM報告書2005年、135–136ページ。 ツェラー、T.;ミュンシュテット、K.;シュトル、C.;シュヴェーダー、J.;ゼンフ、B.;ルッカヘーベルレ、E.;ベッカー、S.;ザーヴェ、 H.;ヒュブナー、J.(2013年3月1日)。「総合がんセンターにおける婦人科がん外来患者に対する補完代替医療とがん治療の潜在的相互作用」。 『Journal of Cancer Research and Clinical Oncology』139巻3号、357–365頁。complementary and alternative medicine with cancer therapy in outpatients with gynecological cancer in a comprehensive cancer center". Journal of Cancer Research and Clinical Oncology. 139 (3): 357–365. doi:10.1007/s00432-012-1336-6. ISSN 1432-1335. PMC 11824351. PMID 23099993. S2CID 29598970. Bodeker, G.; et al. (2002). 「伝統的、補完的、代替医療のための公衆衛生アジェンダ」。American Journal of Public Health. 92 (10): 1582–1591. doi:10.2105/AJPH.92.10.1582. PMC 3221447. PMID 12356597. ヴィッカース、A. (2004). 「代替がん治療:「証明されていない」か「反証されている」か?」。CA – 臨床医のためのがんジャーナル。54 (2): 110–118. CiteSeerX 10.1.1.521.2180. doi:10.3322/canjclin.54.2.110. PMID 15061600. S2CID 35124492. Hróbjartsson A, Gøtzsche PC (2010年1月). Hróbjartsson A (編). 「あらゆる臨床症状に対するプラセボ介入」 (PDF). コクラン・データベース・オブ・システマティック・レビュー. 106 (1): CD003974. doi:10.1002/14651858.CD003974.pub3. PMC 7156905. PMID 20091554. 2019年4月2日にオリジナル (PDF) からアーカイブされた。2019年3月25日に取得。 Hróbjartsson A, Gøtzsche PC (2001年5月). 「プラセボは無力か?プラセボと無治療を比較した臨床試験の分析」. The New England Journal of Medicine. 344 (21): 1594–1602. doi:10.1056/NEJM200105243442106. PMID 11372012. キーンレ GS、キーン H (1997年12月). 「強力なプラセボ効果:事実か虚構か?」. 臨床疫学ジャーナル. 50 (12): 1311–1318. doi:10.1016/s0895-4356(97)00203-5. PMID 9449934. 「25億ドルを費やしたが、代替療法は見つからなかった」。代替医療。NBCニュース.com。AP通信。2009年6月10日。 Sobel, D.S. (2000). 「第28章:心身医学的介入の費用対効果」。Mayer, E.A.; Saper, C.B. (eds.). 心身相互作用の生物学的基盤. 脳研究の進歩. 第122巻. pp. 393–412. doi:10.1016/S0079-6123(08)62153-6. ISBN 978-0-444-50049-6. PMID 10737073. ベイヤーシュタイン, B.L. (1999). 「心理学と『代替医療』―無効な治療が効果があるように見える社会的・判断的バイアス」. 代替医療の科学的レビュー. 3 (2). 2011年10月12日にオリジナルからアーカイブ. 2008年7月7日に閲覧. リマー、アビ(2018年1月25日)。「共感と倫理:エドザード・エルンストとの5分間」。BMJ。360: k309。doi:10.1136/bmj.k309。PMID 29371199。S2CID 3511158。 ローレンス、ジェレミー(2008年4月22日)。「補完療法:大いなる詐欺か?」。インディペンデント紙。ロンドン。2010年4月17日にオリジナルからアーカイブ。2010年4月23日に取得。 ジェローム・グループマン (2013年10月19日). 「代替医療の怪しげなカルト。ポール・オフィット博士のペテン師との戦い」. ザ・ニュー・リパブリック. 2015年2月3日に取得. ワイズレダー, P (2010年1月). 「非倫理的な処方箋:脳性麻痺児に対する代替療法」. 臨床小児科学。49(1): 7–11. doi:10.1177/0009922809340438. PMID 19628756. S2CID 19719686. エルンスト、エドザード (2015). 『不思議の国の科学者:真実を探しトラブルに遭遇した回想録』. イギリス・エクセター: Imprint Academic. pp. 404, 439, 443. ISBN 978-1-84540-777-3. Singh, Simon; Ernst, Edzard (2008). トリックか治療か:代替医療に関する否定できない事実(第 1 版、米国版)。ニューヨーク:W.W. Norton。201、222、259 ページ。ISBN 978-0-393-33778-5。 ヴェーバー、D.O. (1998). 「代替医療と代替医療の選択肢」. Physician Executive. 24 (6): 6–14. PMID 10351720. ベイアスタイン、B.L. (2001). 「代替医療と一般的な推論の誤り」. Academic Medicine. 76 (3): 230–237. doi:10.1097/00001888-200103000-00009. PMID 11242572. S2CID 41527148. Barnes, P.M.; Powell-Griner, E.; McFann, K.; Nahin, R.L. (2004). 「成人における補完代替医療の利用:2002年、米国」 (PDF). 生命統計および健康統計の事前データ (343): 1–19. PMID 15188733. マーティン、エレーヌ; デボンズ、ジェローム (2015). 「スイスにおけるCAMと従来型医療:理論では分断され、実践では統合されている」. ゲイル、ニコラ K.、マクヘイル、ジャン V. (編). 『補完代替医療のラウトレッジ・ハンドブック:社会科学と法律からの視点』. ロンドンおよびニューヨーク:ラウトレッジ. pp. 271–291. ISBN 978-1-136-68555-2. 「伝統医療」. WHO. 2003. 2008-07-27にオリジナルからアーカイブ. 2008-03-06に取得. カストロ, アラチュ; サベージ, バージニア; カウフマン, ハンナ (2015). 「ラテンアメリカにおける先住民およびアフリカ系女性への公平な医療の評価」. 『Revista Panamericana de Salud Pública』38巻2号:96–109頁。ISSN 1020-4989。PMID 26581050。 ホロビン、D.F.(1986)。「研究支援のための輝かしい賞」。『Nature』324巻6094号:221頁。Bibcode:1986Natur.324. .221H. doi:10.1038/324221a0. S2CID 28273314. Salzberg, Steven (2018年3月26日). 「2018年度新予算に埋もれた1億4200万ドルの偽科学医療」. Forbes. 2019年2月14日閲覧。 「NCCIHの資金調達:予算配分の歴史」. NCCIH. 2008年1月9日. 2009年6月25日にオリジナルからアーカイブ. 2008年4月2日に取得. Gorski, David (2016年4月4日). 「NCCIH戦略計画2016-2021、あるいは:たまには本物の科学をやってみよう」. Science-Based Medicine. 2019年2月14日閲覧. Atwood, K.C. IV (2003年9月-10月). 「国立補完代替医療センターにおける継続的な問題」『Skeptical Inquirer』27巻5号。2009年11月16日時点のオリジナルからアーカイブ。2009年11月18日閲覧。 グリーン、ソール(2001年)。「 代替医療局/国立補完代替医療センターの表明された目標と助成金」. 代替医療の科学的レビュー. 5 (4): 205–207. 2011年補完代替医療年次報告書 (PDF) (報告書). 2022年10月9日にオリジナルからアーカイブ (PDF). ワドマン、メレディス (2009年12月7日). 「センターは治療用ハーブから距離を置く」. ネイチャー. 462 (7274). ネイチャー・パブリッシング・グループ: 711. doi:10.1038/462711a. PMID 20010660. ゴルスキー, デイヴィッド; ノベラ, スティーブン (2014年8月20日). 「統合医療の臨床試験:魔法が効くかどうかをテストするのか?」 分子医学の動向。20 (9): 473–476. doi:10.1016/j.molmed.2014.06.007. PMID 25150944. Coulter, I.D.; et al. (2004). 「補完代替医療の台頭と拡大:社会学的視点」 Medical Journal of Australia. 180 (11): 587–589. doi:10.5694/j.1326-5377.2004.tb06099.x. PMID 15174992. S2CID 15983789. Phutrakool P, Pongpirul K (2022年1月). 「専門医における補完代替医療の受容と利用:15年間の系統的レビューとデータ統合」. 系統的レビュー. 11 (1) 10. doi:10.1186/s13643-021-01882-4. PMC 8759198. PMID 35027078。 メリック、ジャナ(2003年6月)。「スピリチュアルヒーリング、病気の子供たち、そして法律:アメリカ医療制度における不平等」。American Journal of Law & Medicine。29 (2): 269–299。doi:10.1017/S0098858800002847。PMID 12961808。S2CID 27122896。 「児童虐待とネグレクトの定義」 (PDF)。児童福祉情報ゲートウェイ。2007年4月。2007年10月11日にオリジナル (PDF) からアーカイブ。2009年2月27日に取得。 アイゼンバーグ、D.M.;他 (1998). 「米国における代替医療利用の動向、1990–1997年:追跡全国調査の結果」. JAMA. 280 (18): 1569–1575. doi:10.1001/jama.280.18.1569. PMID 9820257. パトリシア・M・バーンズ、イブ・パウエル・グライン、キム・マクファン、リチャード・L・ナヒン(2004年5月27日)。「成人における補完代替医療 の利用:2002年、米国」(PDF)。生命統計および健康統計からの事前データ。343。CDC:1–20。2021年6月1日取得。 ワーナー、J. (2006-07-20). 「代替医療が主流になる」. WebMD. CBS ニュース. 2013-09-28 のオリジナルからアーカイブ. 2013-03-11 取得. バーンズ、P.M.; ブルーム、B.; ナヒン、R.L. (2008). 「成人および小児における補完代替医療の利用:米国、2007年」. National Health Statistics Reports (12): 1–23. PMID 19361005. 2022年10月9日にオリジナルからアーカイブ. サー・ウォルトン: 科学技術委員会 2000. ウジャスティク 2003. 「補完代替医療(CAM)」。NHSキャリアウェブサイト。イングランド国民保健サービス(NHS)、英国保健省。2013年4月3日にオリジナルからアーカイブ。2013年3月11日に取得。 ケレヘア、A.(2003)。「補完医療:緩和ケア実践においてより受け入れられやすいか?」。オーストラリア医学雑誌。179 (6 補遺): S46 – S48。doi:10.5694/j.1326-5377.2003.tb05580.x。PMID 12964939。S2CID 35560507。 Menefee, L.A.; Monti, D.A. (2005). 「がん疼痛管理における非薬物療法および補完的アプローチ」. アメリカ整骨医学会誌. 105 (5 補遺): S15 – S20. PMID 16368903. 2008年12月1日にオリジナルからアーカイブ. WHO 2005. 「補完代替療法」. www.cancerresearchuk.org. 英国がん研究機構. 2019年7月4日. Cassileth, B.R. (1996). 「代替・補完的癌治療」. The Oncologist. 1 (3): 173–179. CiteSeerX 10.1.1.493.434. doi:10.1634/theoncologist.1-3-173. PMID 10387984. マーティ、A.T.(1999)。「ドイツ委員会Eモノグラフ全集:ハーブ医薬品の治療ガイド」。書籍、雑誌、新メディア。JAMA。281 (19): 1852–1853. doi:10.1001/jama.281.19.1852-JBK0519-2-1. 医薬品評価研究センター (2022年1月5日). 「医薬品健康詐欺」. FDA. 2010年7月1日時点のオリジナルからアーカイブ. 2022年5月21日閲覧. 生物製剤評価研究センター(2020年5月6日)。「補完代替医療製品と食品医薬品局によるその規制」。米国食品医薬品局。2019年9月5日にオリジナルからアーカイブ。2022年5月21日に取得。 「付録E:医療現場における補完代替療法の使用に関するモデルガイドライン」。米国における補完代替医療。全米学術会議出版局。2005年。 298–308頁。doi:10.17226/11182。ISBN 0-309-09270-1。PMID 22379647. 2021年6月14日閲覧。 ヒルズ, B. (2011-09-23) [1999]. 「偽の治療者たち:オーストラリアの年間10億ドル規模の代替医療産業が効果なく制御不能な理由」. BenHills.com. 2012年3月15日にオリジナルからアーカイブされた。2008年3月6日に取得。 スワン、N. (2000年10月2日). 「代替医療 – 第三部」. ヘルス・レポート. オーストラリア放送協会. ラジオ・ナショナル. 2008年3月6日にオリジナルからアーカイブされた。2008年3月6日に取得。 ルーズベ、J; ハシェンプール、M. H.; ヘイダリ、M (2013年11月). 「血液透析患者におけるハーブ療法の使用」. イラン腎臓病ジャーナル. 7 (6): 492–495. PMID 24241097. デル・プレテ、A; スカレラ、A; イアデヴァイア、M. D.; ミランダ、A; ズッリ、C; ガエタ、L; トゥッチッロ、C; フェデリコ、A; ロゲルシオ、C (2012). 「ハーブ製品:慢性肝疾患における利点、限界、および応用」. Evid Based Complement Alternat Med. 2012: 1–19. doi:10.1155/2012/837939. PMC 3443820. PMID 22991573. ステリン, I. (1996年12月). 「ホメオパシー:真の医療か、空虚な約束か?」. FDAコンシューマー誌. 2007年10月12日にオリジナルからアーカイブ. Ernst, Edzard; Smith, Kevin (2018). 益よりも害が多い?:補完代替医療の道徳的迷路。スイス、シャム:Springer。18 ページ。ISBN 978-3-319-69941-7。OCLC 1019807158。 ナヴァロ、V.J.、他(2006)。「薬物関連肝毒性」。ニューイングランド・ジャーナル・オブ・メディシン。354 (7): 731–739. doi:10.1056/NEJMra052270. PMID 16481640. S2CID 41793815. Lilienfeld, S.O. (2002). 「私たちの存在意義」. メンタルヘルス実践の科学的レビュー. 1 (1). 2007-07-11 のオリジナルからアーカイブ。2008-01-28 に取得。 Hughes, D. (2010-12-23) . 「代替療法は子供にとって『危険』と報告書が指摘」. BBCニュース. 2010年12月24日にオリジナルからアーカイブ. Miller, Gabriel (2014年9月2日), 「専門家に聞く:補完代替医療と癌」, Medscape, 2014年9月7日取得 Ernst, E.; et al. (2004). 「エビデンスに基づく補完代替医療で生じる倫理的問題」. Journal of Medical Ethics. 30 (2): 156–159. doi:10.1136/jme.2003.007021. PMC 1733834. PMID 15082809. Ernst, E. (1999). 「補完医療研究への資金提供:英国の状況」. Complementary Therapies in Medicine. 7 (4): 250–253. doi:10.1016/S0965-2299(99)80011-9. PMID 10709311. Ernst, .E; Pittler, M.H.; Stevinson, C.; White, A., eds. (2001). 『補完代替医療のデスクトップガイド』. Edinburgh: Mosby. ISBN 978-0-7234-3207-4. OCLC 492760852. ホール、ハリエット (2019). 「代替医療における科学への羨望」. 『懐疑的探求者』. 43 (4): 21–23. 2019年9月17日にオリジナルからアーカイブ. 2019年9月17日に閲覧. フィスケン、ロジャー・A. (2014-05-19). 「代替医療ではなく、エビデンスに基づく医療を教えよ」. BMJ. 348: g3218. doi:10.1136/bmj.g3218. ISSN 1756-1833. PMID 24839973. S2CID 206902331. Brown, D. (2009-03-17). 「科学者たちが代替医療研究への連邦資金に反対を表明」. The Washington Post. 2010-04-23 取得. Cassileth, B.R. (1999). 「がん患者に対する補完代替療法の評価」. CA – A Cancer Journal for Clinicians. 49 (6): 362–375. doi:10.3322/canjclin.49.6.362. PMID 11198952. S2CID 7889638. Derkatch, C. (2016). 『境界を画する生物医学:代替医療の新たな科学における証拠とレトリック』シカゴ大学出版局. p. 215. ISBN 978-0-226-34584-0. 2023年3月18日閲覧. Sampson W, Atwood K (2005). 「 不条理の伝播:不条理の境界の再考」。Med. J. Aust. 183 (11–12): 580–581. doi:10.5694/j.1326-5377.2005.tb00040.x. PMID 16336135. S2CID 43272637。 バレット、S. (2004-02-10). 「「代替」医療法に警戒せよ」. クワックウォッチ. 2008-05-09 のオリジナルからアーカイブ。2008-03-03 取得。 「NCAHF の使命声明」。全米健康詐欺対策協議会 (NCAHF) ウェブサイト。2009-11-30。2013-03-11 取得。 Steele, F.R. (1996). 「書評:悪魔に憑かれた世界:暗闇のろうそくとしての科学、カール・セーガン著」。ネイチャー・メディシン。2 (9): 1042. doi:10.1038/nm0996-1042. S2CID 41229701. ハインズ, T. (2003). 『疑似科学と超常現象』(第2版). ニューヨーク州アマースト: プロメテウス・ブックス. ISBN 978-1-57392-979-0. Sampson, W. (2001). Grollman, A.P. (編). 「代替療法教育における教育改革の必要性」. Academic Medicine. 76 (3): 248–250. doi:10.1097/00001888-200103000-00011. PMID 11242574。 Coulter et al. 2004。 Kent 1997。 Sagan 1996。 Acharya, D.; et al. (2008). 『先住民の薬草療法:部族の処方と伝統的な薬草実践』. インド、ジャイプール: Aavishkar Publishers. p. 440. ISBN 978-81-7910-252-7。 IOM報告書2005年、p. 146。 Xiaorui Zhang。「伝統的医薬品:定義」。WHOウェブサイト。2013年9月27日にオリジナルからアーカイブ。2012年11月11日に取得。WHO 2000年より抽出。 IOM報告書2005年、17-19ページ。 Zollman, C. 他 (1999). 「補完医療とは何か?」. 補完医療のABC. BMJ. 319 (7211): 693–696. doi:10.1136/bmj.319.7211.693. PMC 1116545. PMID 10480829. フォンファ、アン・E.(2017年9月1日)。「患者の視点:補完代替医療療法への障壁が患者と生存者に問題をもたらす」。統合がん治療。6(2007 年9月): 297–300頁。doi:10.1177/1534735407306598。PMID 17761643。 Ernst, E. (2005). 「ハーブ療法の有効性 - 概観」. Fundamental & Clinical Pharmacology. 19 (4): 405–409頁。doi:10.1111/j.1472-8206.2005.00335.x. PMID 16011726. S2CID 2327655. ドーキンス, R. (2003). メノン, L. (編). 『悪魔のチャプレン:選集』. ロンドン: ワイデンフェルド・アンド・ニコルソン. ISBN 978-0-7538-1750-6. (2004年米国版 ISBN 0618335404 の180ページ). ホロウェイ, R. (2003-02-14). 「冷酷な見解」. 書籍. ガーディアン. ロンドン. 2010-04-11にオリジナルからアーカイブ. 2010-04-23に取得. Ernst, E. (1996). 「補完医療の倫理」. Journal of Medical Ethics. 22 (4): 197–198. doi:10.1136/jme.22.4.197. PMC 1376996. PMID 8863142. バトラー、K. 他(1992)。『「代替医療」消費者ガイド:ホメオパシー、鍼治療、信仰治療その他の非従来型治療を検証する』。コンシューマー・ヘルス・ライブラリー。ニューヨーク州バッファロー:プロメテウス。ISBN 978-0-87975-733-5。 アーンスト、E.(2011年11月8日)。「代替医療は依然として倫理の空白地帯だ」。ガーディアン。ロンドン。2013年1月28日にオリジナルからアーカイブ。 ホール、ハリエット(2015年9月)、「証拠:『私の叔母ティリーには効いた』では不十分」、『懐疑論者』、第20巻第3号、2015年11月22日取得 エルンスト、エドザード(2011年)。「代替医療における利益相反」。『懐疑的探求者』。35巻4号。 ゴルスキー、デイヴィッド(2009年11月16日)。「科学に基づく医療における利益相反」。『科学に基づく医療』。 ホール、ハリエット・A.(2011年4月27日)。「利益相反」。『科学に基づく医療』。 |
| Bibliography Bivins, R. (2007). Alternative Medicine? A History. Oxford University Press. ISBN 978-0-19-921887-5. Board of Science and Education, British Medical Association (1993). Complementary Medicine: New Approaches to Good Practice. Oxford University Press. ISBN 978-0-19-286166-5. Callahan, D., ed. (2004). The Role of Complementary and Alternative Medicine: Accommodating Pluralism. Washington, D.C.: Georgetown University Press. ISBN 978-1-58901-464-0. Cohen, Michael H. (1998). Complementary & Alternative Medicine: Legal Boundaries and Regulatory Perspectives. Baltimore: Johns Hopkins University Press. ISBN 978-0-8018-5689-1. Committee on the Use of Complementary and Alternative Medicine by the American Public for the Board on Health Promotion and Disease Prevention, Institute of Medicine (2005). Complementary and Alternative Medicine in the United States. Washington, D.C.: National Academy Press. ISBN 978-0-309-09270-8. Gevitz, N. (1997) [1993]. "Chapter 28: Unorthodox Medical Theories". In Bynum, W.F.; Porter, R.S. (eds.). Companion Encyclopedia of the History of Medicine. Vol. 1. New York & London: Routledge. ISBN 978-0-415-16419-1. Hahnemann, S. (1833). The Homœopathic Medical Doctrine, or "Organon of the Healing Art". Translated by Devrient, C.H. Annotated by Stratten, S. Dublin: W.F. Wakeman. Kasper, Dennis L; Fauci, Anthony S.; Hauser, Stephen L.; Longo, Dan L.; Jameson, J. Larry; Loscalzo, Joseph (2015). Harrison's Principles of Internal Medicine (19th ed.). New York: McGraw Hill Education. ISBN 978-0-07-180215-4. Kopelman, L. "The Role of Science in Assessing Conventional, Complementary, and Alternative Medicines". In Callahan (2004), pp. 36–53. Mishra, Lakshmi Chandra (2004). Scientific Basis for Ayurvedic Therapies. Boca Raton: CRC Press. ISBN 978-0-8493-1366-0. O'Connor, Bonnie Blair (1995). Healing Traditions: Alternative Medicine and the Health Professions. Philadelphia: University of Pennsylvania Press. ISBN 978-0-8122-1398-0. Ruggie, M. (2004). Marginal to Mainstream: Alternative Medicine in America. Cambridge University Press. ISBN 978-0-521-83429-2. Sagan, C. (1996). The Demon-Haunted World: Science As a Candle in the Dark. New York: Random House. ISBN 978-0-394-53512-8. Saks, M. (2003). Orthodox and Alternative Medicine: Politics, Professionalization and Health Care. Sage Publications. ISBN 978-1-4462-6536-9. Sointu, E. (2012). Theorizing Complementary and Alternative Medicines: Wellbeing, Self, Gender, Class. Basingstoke, England: Palgrave Macmillan. ISBN 978-0-230-30931-9. Taylor, Kim (2005). Chinese Medicine in Early Communist China, 1945–63: a Medicine of Revolution. Needham Research Institute Studies. London and New York: RoutledgeCurzon. ISBN 978-0-415-34512-5. Walton J. (2000) [Session 1999–2000, HL 123]. Sixth Report: Complementary and Alternative Medicine. London: The Stationery Office. ISBN 978-0-10-483100-7. Wieland, L.S.; et al. (2011). "Development and classification of an operational definition of complementary and alternative medicine for the Cochrane Collaboration". Alternative Therapies in Health and Medicine. 17 (2): 50–59. PMC 3196853. PMID 21717826. Wujastyk, D., ed. (2003). The Roots of Ayurveda: Selections from Sanskrit Medical Writings. Translated by D. Wujastyk. London and New York: Penguin Books. ISBN 978-0-14-044824-5. General Guidelines for Methodologies on Research and Evaluation of Traditional Medicine (PDF). Vol. WHO/EDM/TRM/2001.1. Geneva: World Health Organization (WHO). 2000. Archived (PDF) from the original on 2022-10-09. This document is not a formal publication of the WHO. The views expressed in documents by named authors are solely the responsibility of those authors. WHO Guidelines on Basic Training and Safety in Chiropractic (PDF). Geneva: WHO. 2005. ISBN 978-92-4-159371-7. Archived (PDF) from the original on 2022-10-09. |
参考文献 Bivins, R. (2007). 代替医療?その歴史. オックスフォード大学出版局. ISBN 978-0-19-921887-5. 英国医師会科学教育委員会 (1993). 補完医療:良き実践への新たなアプローチ. オックスフォード大学出版局. ISBN 978-0-19-286166-5。 キャラハン、D.、編(2004)。補完代替医療の役割:多元主義の受容。ワシントン D.C.:ジョージタウン大学出版局。ISBN 978-1-58901-464-0。 コーエン、マイケル H. (1998)。補完代替医療:法的境界と規制の視点。ボルチモア:ジョンズ・ホプキンズ大学出版局。ISBN 978-0-8018-5689-1。 米国公衆による補完代替医療の利用に関する委員会、健康増進・疾病予防委員会、医学研究所(2005)。米国における補完代替医療。ワシントン D.C.:ナショナル・アカデミー・プレス。ISBN 978-0-309-09270-8。 Gevitz, N. (1997) [1993]。「第 28 章:非正統的な医学理論」。Bynum, W.F.、Porter, R.S. (eds.) 『医学史コンパニオン百科事典』第 1 巻。第1巻。ニューヨーク&ロンドン:ラウトレッジ。ISBN 978-0-415-16419-1。 ハーネマン、S.(1833)。『ホメオパシー医学教義、あるいは「治療術のオルガノン」』。デヴリエント、C.H. 訳。ストラッテン、S. 注釈。ダブリン:W.F. ウェイクマン。 カスパー、デニス・L; ファウチ、アンソニー・S; ハウザー、スティーブン・L; ロング、ダン・L; ジェイムソン、J・ラリー; ロスカルゾ、ジョセフ (2015). 『ハリソン内科学原理 (第19版)』. ニューヨーク: マクグロウヒル・エデュケーション. ISBN 978-0-07-180215-4. コペルマン、L. 「従来型・補完・代替医療の評価における科学の役割」. カラハン編(2004年)、36-53頁. ミシュラ、ラクシュミ・チャンドラ(2004年). 『アーユルヴェーダ療法の科学的根拠』. ボカラトン:CRCプレス. ISBN 978-0-8493-1366-0。 オコナー、ボニー・ブレア(1995)。『ヒーリング・トラディションズ:代替医療と医療専門職』。フィラデルフィア:ペンシルベニア大学出版局。ISBN 978-0-8122-1398-0。 ラギー、M.(2004)。周辺から主流へ:アメリカにおける代替医療。ケンブリッジ大学出版局。ISBN 978-0-521-83429-2。 セーガン、C.(1996)。悪魔に憑かれた世界:闇の中のろうそくとしての科学。ニューヨーク:ランダムハウス。ISBN 978-0-394-53512-8。 サックス、M.(2003)。『正統医療と代替医療:政治、専門職化、医療』。セージ出版。ISBN 978-1-4462-6536-9。 ソイントゥ、E.(2012)。『補完代替医療の理論化:ウェルビーイング、自己、ジェンダー、階級』。イングランド、ベージングストーク:パルグレイブ・マクミラン。ISBN 978-0-230-30931-9。 テイラー、キム(2005)。『共産主義中国初期における漢方医学、1945–63:革命の医学』。ニーダム研究所研究叢書。ロンドンおよびニューヨーク:ラウトリッジ・カーゾン。ISBN 978-0-415-34512-5。 ウォルトン J. (2000) [1999–2000年議会期、HL 123]。第六報告書:補完代替医療。ロンドン:文房具局。ISBN 978-0-10-483100-7。 ヴィーランド, L.S. 他 (2011). 「コクラン・コラボレーションのための補完代替医療の運用定義の開発と分類」. 代替医療と健康. 17 (2): 50–59. PMC 3196853. PMID 21717826. ウジャスティク, D., 編 (2003). 『アーユルヴェーダの根源:サンスクリット医学文献選集』. D. ウジャスティク訳. ロンドン・ニューヨーク:ペンギンブックス. ISBN 978-0-14-044824-5. 伝統医療の研究と評価に関する方法論の一般指針 (PDF). Vol. WHO/EDM/TRM/2001.1. ジュネーブ: 世界保健機関 (WHO). 2000. 2022年10月9日にオリジナルからアーカイブ (PDF). この文書はWHOの正式な出版物ではない。文書内で名指しされた著者が表明した見解は、その著者自身の責任である。 カイロプラクティックにおける基礎訓練と安全に関するWHOガイドライン(PDF)。ジュネーブ:WHO。2005年。ISBN 978-92-4-159371-7。2022年10月9日にオリジナルからアーカイブ(PDF)。 |
| Further reading Bausell, R.B (2007). Snake oil science: the truth about complementary and alternative medicine. Oxford University Press. ISBN 978-0-19-531368-0. Benedetti, F.; et al. (2003). "Open versus hidden medical treatments: The patient's knowledge about a therapy affects the therapy outcome". Prevention & Treatment. 6 (1). doi:10.1037/1522-3736.6.1.61a. Dawkins, R. (2001). "Foreword". In Diamond, J. (ed.). Snake Oil and Other Preoccupations. London: Vintage. ISBN 978-0-09-942833-6. Reprinted in Dawkins 2003. Downing AM, Hunter DG (2003). "Validating clinical reasoning: A question of perspective, but whose perspective?". Manual Therapy. 8 (2): 117–119. doi:10.1016/S1356-689X(02)00077-2. PMID 12890440. Eisenberg DM (July 1997). "Advising patients who seek alternative medical therapies". Annals of Internal Medicine. 127 (1): 61–69. doi:10.7326/0003-4819-127-1-199707010-00010. PMID 9214254. S2CID 23351104. Gunn IP (December 1998). "A critique of Michael L. Millenson's book, Demanding Medical Excellence: Doctors and Accountability in the Information Age, and its Relevance to CRNAs and Nursing". AANA Journal. 66 (6): 575–582. ISSN 0094-6354. PMID 10488264. Hand, W.D. (1980). "Folk Magical Medicine and Symbolism in the West". Magical Medicine. Berkeley: University of California Press. pp. 305–319. ISBN 978-0-520-04129-5. OCLC 6420468. Illich, I. (1976). Limits to Medicine: Medical Nemesis: The Expropriation of Health. Penguin. ISBN 978-0-14-022009-4. OCLC 4134656. Mayo Clinic (2007). Mayo Clinic Book of Alternative Medicine: The New Approach to Using the Best of Natural Therapies and Conventional Medicine. Parsippany, New Jersey: Time Home Entertainment. ISBN 978-1-933405-92-6. Planer, F.E. (1988). Superstition (Rev. ed.). Buffalo, New York: Prometheus Books. ISBN 978-0-87975-494-5. OCLC 18616238. Rosenfeld, A. (c. 2000). "Where Do Americans Go for Healthcare?". Cleveland, Ohio: Case Western Reserve University. Archived from the original on 2006-05-09. Retrieved 2010-09-23. Snyder, Mariah; Lindquist, Ruth (May 2001). "Issues in Complementary Therapies: How We Got to Where We Are". Online Journal of Issues in Nursing. 6 (2): 1. PMID 11469921. Archived from the original on 2017-02-03. Retrieved 2017-01-18. Stevens, P. Jr. (November–December 2001). "Magical thinking in complementary and alternative medicine". Skeptical Inquirer. Tonelli MR (2001). "The limits of evidence-based medicine". Respiratory Care. 46 (12): 1435–1440, discussion 1440–1441. PMID 11728302. Trivieri, L. Jr. (2002). Anderson, J.W. (ed.). Alternative Medicine: The Definitive Guide. Berkeley: Ten Speed Press. ISBN 978-1-58761-141-4. Wisneski, L.A.; et al. (2005). The scientific basis of integrative medicine. CRC Press. ISBN 978-0-8493-2081-1. Zalewski, Z. (1999). "Importance of philosophy of science to the history of medical thinking". CMJ. 40 (1): 8–13. PMID 9933889. Archived from the original on 2004-02-06. World Health Organization Benchmarks for training in traditional / complementary and alternative medicine WHO Kobe Centre; Bodeker, G.; et al. (2005). WHO Global Atlas of Traditional, Complementary and Alternative Medicine. WHO. ISBN 978-92-4-156286-7. Summary. Journals Alternative Medicine Review: A Journal of Clinical Therapeutics. Sandpoint, Idaho : Thorne Research, c. 1996 NLM ID: 9705340 Archived 2018-06-12 at the Wayback Machine Alternative Therapies in Health and Medicine. Aliso Viejo, California : InnoVision Communications, c1995- NLM ID: 9502013 Archived 2018-06-12 at the Wayback Machine BMC Complementary and Alternative Medicine Archived 2015-09-24 at the Wayback Machine. London: BioMed Central, 2001 NLM ID: 101088661 Archived 2018-06-12 at the Wayback Machine Complementary Therapies in Medicine. Edinburgh; New York : Churchill Livingstone, c. 1993 NLM ID: 9308777 Archived 2018-06-12 at the Wayback Machine Evidence Based Complementary and Alternative Medicine: eCAM. New York: Hindawi, c. 2004 NLM ID: 101215021 Archived 2018-09-14 at the Wayback Machine Forschende Komplementärmedizin / Research in Complementary Medicine Journal for Alternative and Complementary Medicine New York : Mary Ann Liebert, c. 1995 Scientific Review of Alternative Medicine (SRAM) Archived 2010-08-22 at the Wayback Machine |
参考文献 Bausell, R.B (2007). 『偽科学の医療:補完代替医療の真実』. オックスフォード大学出版局. ISBN 978-0-19-531368-0. Benedetti, F. 他 (2003). 「公開治療と非公開治療:治療に関する患者の知識が治療結果に影響を与える」『予防と治療』6巻1号 doi:10.1037/1522-3736.6.1.61a. ドーキンス, R. (2001). 「序文」. ダイヤモンド, J. (編). 『スネークオイルとその他の関心事』. ロンドン: ヴィンテージ. ISBN 978-0-09-942833-6. ダウキンス 2003 に再版. ダウニング AM, ハンター DG (2003). 「臨床推論の妥当性検証:視点の問題だが、誰の視点か?」『マニュアルセラピー』8巻2号:117–119頁。doi:10.1016/S1356-689X(02)00077-2。PMID 12890440。 アイゼンバーグ、D.M.(1997年7月)。「代替医療を求める患者への助言」. Annals of Internal Medicine. 127 (1): 61–69. doi:10.7326/0003-4819-127-1-199707010-00010. PMID 9214254. S2CID 23351104. ガン IP (1998年12月). 「マイケル・L・ミレンソンの著書『医療の卓越性を求める:情報化時代における医師と説明責任』に対する批判、及びそのCRNAと看護への関連性」. AANAジャーナル. 66 (6): 575–582. ISSN 0094-6354. PMID 10488264. ハンド、W.D.(1980)。「西洋における民俗的魔法医療と象徴性」。『魔法医療』。バークレー:カリフォルニア大学出版局。pp. 305–319。ISBN 978-0-520-04129-5。OCLC 6420468。 イリッヒ, I. (1976). 『医療の限界:医療のネメシス―健康の収奪』. ペンギン. ISBN 978-0-14-022009-4. OCLC 4134656. メイヨークリニック (2007). 『メイヨークリニック代替医療ガイド:自然療法と従来医療のベストを活かす新アプローチ』. ニュージャージー州パーシッパニー:タイム・ホーム・エンターテイメント。ISBN 978-1-933405-92-6。 プレーナー、F.E.(1988)。『迷信(改訂版)』。ニューヨーク州バッファロー:プロメテウス・ブックス。ISBN 978-0-87975-494-5。OCLC 18616238。 ローゼンフェルド、A.(2000年頃)。「アメリカ人はどこで医療を受けるのか?」オハイオ州クリーブランド:ケース・ウェスタン・リザーブ大学。2006年5月9日にオリジナルからアーカイブ。2010年9月23日に取得。 スナイダー、マリア;リンドクイスト、ルース(2001年5月)。「補完療法の問題点:現状に至る経緯」. 看護問題オンラインジャーナル. 6 (2): 1. PMID 11469921. 2017-02-03にオリジナルからアーカイブ. 2017-01-18に取得. スティーブンス, P. Jr. (2001年11月–12月). 「補完代替医療における魔法的思考」。Skeptical Inquirer。 トネリ MR (2001)。「エビデンスに基づく医療の限界」。Respiratory Care。46 (12): 1435–1440、議論 1440–1441。PMID 11728302。 トリヴィエリ、L. Jr. (2002)。アンダーソン、J.W. (編)。代替医療:決定版ガイド。バークレー:Ten Speed Press。ISBN 978-1-58761-141-4。 ウィスネスキ、L.A. 他 (2005)。統合医療の科学的根拠。CRC Press。ISBN 978-0-8493-2081-1。 Zalewski, Z. (1999). 「医学思想の歴史における科学哲学の重要性」. CMJ. 40 (1): 8–13. PMID 9933889. 2004-02-06 のオリジナルからアーカイブ。 世界保健機関 伝統的/補完代替医療の研修基準 WHO神戸センター; Bodeker, G.; 他 (2005). WHO伝統的・補完・代替医療世界アトラス. WHO. ISBN 978-92-4-156286-7. 要約. 学術誌 代替医療レビュー:臨床治療学雑誌. アイダホ州サンドポイント:ソーン・リサーチ、1996年頃 NLM ID: 9705340 2018-06-12 ウェイバックマシンにアーカイブ 健康と医療における代替療法。カリフォルニア州アリソビエホ:イノビジョン・コミュニケーションズ、1995年頃 NLM ID: 9502013 2018-06-12 ウェイバックマシンにアーカイブ BMC補完代替医療 2015年9月24日ウェイバックマシンにアーカイブ。ロンドン:バイオメッド・セントラル、2001年 NLM ID: 101088661 2018年6月12日ウェイバックマシンにアーカイブ 補完療法医学。エディンバラ; ニューヨーク:チャーチル・リビングストン、1993年頃 NLM ID: 9308777 2018-06-12 ウェイバックマシンにアーカイブ エビデンスに基づく補完代替医療:eCAM。ニューヨーク:ヒンダウィ、2004年頃 NLM ID: 101215021 2018-09-14 ウェイバックマシンにアーカイブ 研究的補完医療 / Research in Complementary Medicine 代替・補完医療ジャーナル ニューヨーク:メアリー・アン・リーバート社、1995年頃 代替医療の科学的レビュー (SRAM) ウェイバックマシンに2010年8月22日アーカイブ |
| https://en.wikipedia.org/wiki/Alternative_medicine |
リンク(サイト内)
リンク(サイト外)
文献
その他の情報
Copyleft, CC, Mitzub'ixi Quq Chi'j, 1996-2099
++
Copyleft,
CC, Mitzub'ixi Quq Chi'j, 1996-2099