ハームリダクション 2.0としての「しきいを下げるプログラム」
Low-threshold
treatment programs,
Low-threshold harm reduction health care programs
「社会正義を公衆衛生や医療の中心に据えなければ、現在公衆衛生において流行している概念の
多く——飛鷹対効用から持続可能、反復可能まで——が悪用される可能性がある」(ポール・ファーマー 2012:51)
このページでは、しきいを下げるハームリダクション・プログラムについて考える。低しきい値療法プログ ラム(あるいはしきい値の低いハームリダクションプログラムは、薬物 使用者を対象としたハー ムリダクションに基づくヘルスケアの改訂版として考えだされたものである。「低しき い値」 プログラムは、患者への要求を最小限に抑え、薬物の摂取量をコントロールしようとせずにサービスを提供し、要求された場合のみカウンセリングを提供するプ ログラムである。低しきい値プログラムは、使用者が一定レベルのコントロールを受け入れることを要求し、支援の前提として患者にカウンセリ ングの受け入れとすべての薬物使用の中止を要求する「高閾値」プログラムと対比されることがある。(→カナダ・アルバータ州の「しきいの低いサービス(ちらし)」の事例)
科学研究
費補助金「支
援プログラムの「しきい」を下げる:薬物使用者の求助行動とサービスアクセスの研究」の支援をいただいている(→「ハームリダクション」「ハームリダクションのすすめ」「ハームリダクションの多様性」)。
★以下は、ウィキペディア英語の"Low-threshold treatment programs"の引用から。
| Low-threshold
treatment programs are harm reduction-based health care centers
targeted towards people who use substances.[1] "Low-threshold" programs
are programs that make minimal demands on the patient, offering
services without attempting to control their intake of drugs, and
providing counselling only if requested. Low-threshold programs may be
contrasted with "high-threshold" programs, which require the user to
accept a certain level of control and which demand that the patient
accept counselling and cease all drug use as a precondition of
support.[2] 1. Islam, M. M.; Day, C. A.; Conigrave, K. M. (2010). "Harm reduction healthcare: From an alternative to the mainstream platform?". International Journal of Drug Policy. 21 (2): 131–133. doi:10.1016/j.drugpo.2010.01.001. PMID 20092999. 2. Waal, Helge. "Risk reduction as a component of a comprehensive, multidisciplinary approach to drug abuse problems"(リンク切れ)→Principles of Drug Dependence Treatment, WHO 2008. |
低しきい値療法プログラム(あるいはしきい値の低いハームリダクションプログラム)は、薬物使用者を対象としたハー
ムリダクションに基づくヘルスケアに中心化されたものである。「低しきい値」
プログラムは、患者への要求を最小限に抑え、薬物の摂取量をコントロールしようとせずにサービスを提供し、要求された場合のみカウンセリングを提供するプ
ログラムである。低しきい値プログラムは、使用者が一定レベルのコントロールを受け入れることを要求し、支援の前提として患者にカウンセリ
ングの受け入れとすべての薬物使用の中止を要求する「高閾値」プログラムと対比されることがある。 1. Islam, M. M.; Day, C. A.; Conigrave, K. M. (2010). "Harm reduction healthcare: From an alternative to the mainstream platform?". International Journal of Drug Policy. 21 (2): 131–133. doi:10.1016/j.drugpo.2010.01.001. PMID 20092999. 2. Waal, Helge. "Risk reduction as a component of a comprehensive, multidisciplinary approach to drug abuse problems"(リンク切れ) |
| Low-threshold treatment programs
are distinct from simple needle exchange programs, and may include
comprehensive healthcare and counseling services.[1][3] The
International Journal of Drug Policy in its volume 24 published an
Editorial which endeavoured to define a service known to be
"low-threshold", based on some popular and known criteria. According to
that Editorial, low-threshold services for drug users can be defined as
those which offer services to drug users; do not impose abstinence from
drug use as a condition of service access; and endeavour to reduce
other documented barriers to service access.[4] Beyond comprehensive
needle exchange services, other examples of low-threshold,
community-based programs include those that support people who use
alcohol or drugs to consider positive or health protective changes
without a demand for "recovery," such as those piloted in New York City
in the 1990s as "recovery readiness" efforts to bolster HIV
prevention.[5][6] |
低
しきい値療法プログラムは、単なる針交換プログラムとは異なり、包括
的なヘルスケアやカウンセリングサービスを含むことがある[1][3]。 International Journal of Drug
Policyの第24巻では、一般的に知られているいくつかの基準に基づいて、「しきい値の低い」サービスを定義しようとする論説が掲載されている。その
論説によれば、薬物使用者のための敷居の低いサービスとは、薬物使用者にサービスを
提供し、サービス利用の条件として薬物使用の禁欲(=断薬)を課さず、
サービス利用に対する他の文書化された障害を減らすよう努めるものと定義することができる[4]。 [4]
包括的な針交換サービス以外にも、閾値の低い地域ベースのプログラムの例として、アルコールや薬物を使用する人々が「回復」を要求することなく、前向きな
変化や健康保護を考慮することを支援するプログラムがあり、1990年代にニューヨーク市でHIV予防を強化する「回復準備」活動として試験的に実施され
たものがある [5] [6]。 |
| Background Injection drug users (IDUs) are at risk of a wide range of health problems arising from non-sterile injecting practices, complications of the drug itself or of the lifestyle associated with drug use and dependence.[7] Furthermore, unrelated health problems, such as diabetes, may be neglected because of drug dependence. Sharing of health information with police, or requirements that patients abstain from all illegal drug use prior to receiving support are further impediments to health seeking, or require patients to lie about drug use in order to receive other lifesaving services.[8] For all these reasons, despite their increased health care needs, IDUs do not have the required access to care or may be reluctant to use conventional services.[9] Consequently, their health may deteriorate to a point at which emergency treatment is required,[10] with considerable costs to both the IDUs and the health system. Accordingly, harm reduction based health care centers, also known as targeted health care outlet or low-threshold health care outlet for IDUs have been established across a range of settings utilising a variety of models.[1] These targeted outlets provide integrated, low-threshold services within a harm-reduction framework targeting IDUs, and sometimes include social and/or other services. Where a particular service is not provided, referral and assistance with access is available. In 2007, for example, 33% of all US needle-syringe programs (NSPs) provided on-site medical care, and 7% provided buprenorphine treatment.[11] Similarly, in many European countries NSP outlets serve as low-threshold primary health care centers targeting primarily IDUs.[12] |
バッ
クグラウンド 注 射薬使用者(IDU)は、無菌注射の習慣、薬物自体の合併症、薬物使 用や依存に関連したライフスタイルから生じる様々な健康問題のリスクにさらされている[7]。 さらに、糖尿病などの無関係な健康問題が、薬物依存のために放置されることもありえ る。警察との健康情報の共有や、支援を受ける前にすべての違法薬物の使 用を控えるよう患者に要求することは、健康を求める上でさらなる障害となり、また他の救 命サービスを受けるために薬物使用について嘘をつく必要性にかられる [8]。 これらの理由により、IDUの健康管理のニーズが高まっているにもかかわらず、必要なケアを受けられなかったり、従来のサービスを使うことに消極的になっ たりする。その結果、緊急治療が必要になるほど健康状態が悪化し、IDUと医療システムの両方にかなりのコストがかかる可能性があがる[10]。した がって、IDUのための標的型ヘルスケア・アウトレットまたは低閾値ヘルスケア・ア ウトレットとしても知られるハームリダクションベースのヘルスケア・センターが、さ まざまなモデルを活用して、幅広い環境にわたって設置する[1]。これらの標的型アウトレットでは、IDUを対象とした害軽減の枠組みの中 で、統合的で低 閾値のサービスを提供しており、時には社会サービスや他のサービスを含むことがある。特定のサービスが提供されていない場合は、紹介やアクセスに関する支 援を受けることができる。例えば2007年には、米国の注射針プログラム(NSP)の33%が現場で医療を提供し、7%がブプレノルフィン治療を提供して いる[11]。同様に、多くのヨーロッパ諸国では、NSP店舗は主にIDUを対象とした敷居の低い一次医療センターとして機能している[12]。 |
| Health care models These targeted outlets vary widely and may be either "distributive", providing basic harm reduction services and simple healthcare with facilitated referrals to specialist services, or "one-stop-shops" where a range of services including specialist services are provided onsite. The services being offered by these outlets range from simple needle and syringe provision, to expanded services including basic and preventive primary healthcare, hepatitis B and A vaccinations, hepatitis C testing, counselling, tuberculosis screening and sometimes opioid maintenance therapy. Some centers offer hepatitis, HIV treatment and dental care.[13] The goal of these outlets is to provide: (1) opportunistic health care,[14] (2) increased temporal and spatial availability of health care, (3) trustworthy services of health care, (4) cost-effective mode of health care, (5) targeted and tailored services.[15] |
ヘ
ルスケアモデル 標的型アウトレットはさまざまで、基本的な有害物質削減サービスと 簡単なヘルスケアを提供し、専門家への紹介を促す「流通型」、または 専門家サービスを含むさまざまなサービスをその場で提供する「ワンストップショップ 型」のいずれかとなっている。これらの店舗で提供されるサービスは、単純な注射器やシリンジの提供から、基本的な予防医療、B型肝炎やA型 肝炎の予防接 種、C型肝炎検査、カウンセリング、結核スクリーニング、時にはオピオイド維持療法などの拡張サービスまで多岐にわたる。肝炎、HIV治療、歯科治療を行 うセンターもある[13]。これらのアウトレットの目標は、以下を提供することであ る。(1)日和見的なヘルスケア、(2)ヘルスケアの時間的・空間的利 用可能性の向上、(3)ヘルスケアの信頼できるサービス、(4)ヘルスケアの費用対効果の高い形態、(5)対象を絞って調整したサービス[15]、などで ある。 |
| In the United States as of 2011,
211 NSPs were known to be operating in 32 states, the District of
Columbia, Puerto Rico and the Indian Nations.[16] The bulk of funding
has come from state and local governments,[13] since for most of the
last several decades, federal funding for needle exchange programs has
been specifically banned.[17] |
2011年時点の米国では、32の州、コロンビア特別区、プエルトリ
コ、インディアン地区での211のNSP(needle-syringe
programs)が運営されていることが知られている[16]。過去数十年のほとんどで、針交換プログラムに対する連邦政府の資金は特に禁止されていた
ため、資金の大部分は州や地方自治体からのものだった[13][17]。 |
| Globally, as of 2008, at least
77 countries and territories offer NSPs with varying structures, aims,
and goals. Some countries use needle exchange services as part of
integrated programs to contain drug use, while others aim simply to
contain HIV infection as their top priority, considering a reduction in
the incidence of drug use as a much lower priority.[18] Acceptance of
NSPs vary widely from country to country. On the one hand, in Australia
and New Zealand, electronic dispensing machines are available at
selected locations such as the Auckland needle exchange and the
Christchurch needle exchange, allowing needle exchange service 24 hours
to registered users.[19] On the other hand, over half of the countries
in Asia, the Middle East, and North Africa retain the death penalty for
drug offenses, although some have not carried out executions in recent
years.[20] |
2008年現在、世界では少なくとも77の国と地域でNSP
(needle-syringe
programs)が実施されており、その仕組みや目的、目標はさまざまである。薬物乱用防止を目的とした総合的なプログラムの一環として
針交換サービス
を利用する国もあれば、単にHIV感染の防止を最優先とし、薬物乱用防止はそれよりもはるかに低い優先順位で考える国もある[18]。一方、オーストラリ
アやニュージーランドでは、オークランド針交換所やクライストチャーチ針交換所などの特定の場所で電子分包機が利用でき、登録した利用者に24時間針交換
サービスを提供している[19]。
他方、アジア、中東、北アフリカの半数以上の国では、近年は執行していない国もある
が、麻薬犯罪に対する死刑を維持している[20]。 |
| Evaluation Opposite Opinition Low-threshold programs offering needle exchange have faced much opposition on political and moral grounds.[21] Concerns are often expressed that NSPs may encourage drug use, or may actually increase the number of dirty needles in the community.[22] Another fear is that NSPs may draw drug activity into the communities in which they operate.[23] It has also been argued that in fighting disease, needle exchanges take attention away from bigger drug problems, and that, contrary to saving lives, they actually contribute to drug-related deaths.[24] Even in Australia, which is considered a leading country in harm reduction,[15] a survey showed that a third of the public believed that NSPs encouraged drug use, and 20% believed that NSPs dispensed drugs.[25] In the United States, the ambivalent public attitude towards NSPs is often reflected in police interference, with 43% of NSP program managers reporting frequent (at least monthly) client harassment, 31% reporting frequent confiscation of clients' syringes, 12% reporting frequent client arrest, and 26% reporting uninvited police appearances at program sites.[26] A single 1997 study which showed a correlation between frequent program use and elevated rates of HIV infection among IDUs in Vancouver, Canada,[27] has become widely cited by opponents of NSPs as demonstrating their counter-productiveness.[28][29] |
評価 《反対意見》 針交換を提供する低しきい値療法プログラムは、政治的・道徳的な理由か ら多くの反対に遭っている。NSPが薬物使用を助長したり、コミュニティ内の汚れた針の数を実際に増やしたりするのではないかという懸念が しばしば表明さ れる[22]。また、NSPが活動するコミュニティ内に薬物活動を呼び込むのではないかという懸念もある[23]。 23] また、病気との闘いにおいて、針交換はより大きな薬物問題から注意をそらし、命を救 うどころか、実際に薬物関連の死を助長しているという議論もある [24]。ハームリダクションの先進国とされるオーストラリアでさえ[15]、国民の3分の1がNSPが薬物使用を奨励すると信じ、20%がNSPが薬物 を調剤すると信じてい るという調査結果がある[25]。 [25] 米国では、NSPに対する国民のアンビバレントな態度はしばしば警察の干渉に反映され、NSPプログラムマネージャーの43%が頻繁に(少なくとも毎月) クライアントへの嫌がらせを、31%がクライアントの注射器を頻繁に没収して、12%がクライアントを頻繁に逮捕して、26%がプログラムサイトに招かれ ざる警察が現れると報告している。 [26] カナダのバンクーバーにおけるIDUの間でプログラムの頻繁な利用とHIV感染率の上昇との間に相関関係を示した1997年の研究[27]は、NSPの反 対派によって、その逆効果を示すものとして広く引用されるようになった[28][29]。 |
| Authors from the 1997 Vancouver
study have, in multiple publications, issued disclaimers against the
misuse of their work by opponents of NSPs. They point out that frequent
attendees of the program tended to be young and often indulged in
extreme high-risk behaviors. The 1997 results were hence of
statistically biased sampling.[28][29] They have emphasized that the
correct message to be derived from their 1997 study can be read in the
title of their work: "Needle exchange is not enough".[27] This is the
same message presented by many other articles since.[13][30][31][32] |
1997年のバンクーバーでの研究の著者は、複数の出版物で、NSPの
反対派による研究の誤用に対して免責の意を表明している。彼らは、プログラムに頻繁に参加する人は若い傾向があり、しばしば極端な高リスクの行動にふける
ことを指摘している。1997年の結果は、統計的に偏ったサンプリングによるものであった [28] [29]
。「針交換だけでは十分ではない」[27]。これは、それ以降、他の多くの論文によって提示されたメッセージと同じである |
| opinion in favor, or positive
evidence Comprehensive, systematic surveys of the costs and effectiveness of low-threshold primary healthcare programs are not available due to the heterogeneity of these programs and the study designs.[33][34] Narrower focus studies dealing solely with the needle exchange issue are abundant, however, and generally support the thesis that NSPs reduce the risk of prevalence of HIV, hepatitis and other blood-borne diseases. These studies suggest that such outlets improve the overall health status of IDUs and save on the health budget by reducing episodes in emergency departments and tertiary hospitals.[21][30][35][36] In Australia, monitoring of drug users participating in NSPs showed the incidence of HIV among NSP clients to be essentially identical to that of the general population.[32][37] Fears that NSPs may draw drug activity into the communities in which they operate are contradicted by a study that showed that by far the greatest number of clients of an NSP in Chicago came to the area to exchange needles (60%) rather than to buy drugs (3.8%).[38] |
賛成意見、あるいは効果性の証拠 しかし、針交換の問題だけに焦点を絞った研究は数多くあり、一般的に NSPがHIV、肝炎、その他の血液感染症の蔓延リスクを減らすという論文を支持している。これらの研究は、そのような店舗がIDUの全体 的な健康状態を 改善し、救急部や三次病院でのエピソードを減らすことによって医療予算を節約することを示唆している[21][30][35][36] オーストラリアでは、NSPに参加している麻薬使用者のモニタリングによってNSP利用者のHIV発生率が一般集団のそれと本質的に同一であることが示さ れた[32][37]。 [NSPが運営するコミュニティに薬物活動を呼び込むかもしれないという懸念は、シカゴのNSPの顧客のうち、薬物を買うため(3.8%)ではなく、針の 交換(60%)のためにその地域に来る人が圧倒的に多いという研究によって否定された[38] |
| Internationally, support for the
effectiveness of low-threshold programs including needle exchange have
come from studies conducted in Afghanistan,[39] China,[40] Spain,[41]
Taiwan,[42] Estonia,[43] Canada,[44] Iran,[45] and many other
countries. However, in many countries, there is strong opposition to
such programs.[20][46][47] |
国際的には、針交換を含む低しきい値療法プログラムの有効性に対する支
持は、アフガニスタン[39]、中国[40]、スペイン[41]、台湾[42]、エストニア[43]、カナダ[44]、イラン[45]、その他多くの国で
行われた研究から出てきている。しかし、多くの国では、このようなプログラムに対して強い反対がある[20][46][47]。 |
| Despite the lack of randomized
clinical trials demonstrating the impact of low-threshold
services,[33][34][48] the available evidence, barriers to service
access and the late presentation of seriously ill IDUs to hospital,
suggests the ongoing need for targeted and low-threshold services. In
addition, prevention of HIV and hepatitis C transmission is clearly
possible for those unable or unwilling to stop injecting drug use, and
a range of countries using low-threshold approach have achieved control
or virtual elimination of HIV transmission among people who inject
drugs.[49] For these reasons, organizations ranging from the U.S.
National Institutes of Health,[50] the Centers for Disease Control,[51]
the American Bar Association,[52] the American Medical Association,[53]
the American Psychological Association,[54] the World Health
Organization,[55] the European Monitoring Center for Drugs and Drug
Addiction[56] and many others have endorsed low-threshold programs
including needle exchange. References Islam, M. M.; Day, C. A.; Conigrave, K. M. (2010). "Harm reduction healthcare: From an alternative to the mainstream platform?". International Journal of Drug Policy. 21 (2): 131–133. doi:10.1016/j.drugpo.2010.01.001. PMID 20092999. Waal, Helge. "Risk reduction as a component of a comprehensive, multidisciplinary approach to drug abuse problems" (PDF). The Pompidou Group. Retrieved 25 March 2012. Rogers, S. J.; Ruefli, T. (2004). "Does harm reduction programming make a difference in the lives of highly marginalized, at-risk drug users?". Harm Reduction Journal. 1 (1): 7. doi:10.1186/1477-7517-1-7. PMC 420490. PMID 15171790. Islam, MM, Topp, L, Conigrave, KM, and Day, C (2013). "Defining a service for people who use drugs as 'low-threshold': What should be the criteria?". International Journal of Drug Policy. 24 (3): 220–222. doi:10.1016/j.drugpo.2013.03.005. PMID 23567101. Nealy, Eleanor C. (1997-11-07). "Early Intervention with Active Drug and Alcohol Users in Community-Based Settings". Journal of Chemical Dependency Treatment. 7 (1–2): 5–20. doi:10.1300/J034v07n01_02. ISSN 0885-4734. Elovich, R.E., & Cowing, M. (1995). Recovery-readiness: Strategies that bring treatment to addicts where they are. In Harm Reduction and Steps Toward Change: A Training Sourcebook. New York: The Gay Men’s Health Crisis. Latt, N.; Conigrave, K.; Marshall, J.; Saunders, J.; Marshall, J.; Nutt, D. (2009). Addiction Medicine. Oxford University Press. ISBN 9780199539338. Archived from the original on 2011-06-04. Wolfe, Daniel (2007-08-01). "Paradoxes in antiretroviral treatment for injecting drug users: Access, adherence and structural barriers in Asia and the former Soviet Union". International Journal of Drug Policy. HIV Treatment and Care for Injecting Drug Users. 18 (4): 246–254. doi:10.1016/j.drugpo.2007.01.012. ISSN 0955-3959. PMID 17689372. McCoy, C. B.; Metsch, L. R.; Chitwood, D. D.; Miles, C. (2001). "Drug use and barriers to use of health care services". Substance Use & Misuse. 36 (6–7): 789–806. doi:10.1081/ja-100104091. PMID 11697611. S2CID 23220436. McDonald, P (2002). "From streets to sidewalks: developments in primary care services for injecting drug users". Australian Journal of Primary Health. 8: 65–69. doi:10.1071/PY02010. Des Jarlais, D. C.; McKnight, C.; Goldblatt, C.; Purchase, D. (2009). "Doing harm reduction better: Syringe exchange in the United States". Addiction. 104 (9): 1441–1446. doi:10.1111/j.1360-0443.2008.02465.x. PMID 19215605. "Low-threshold services". The European Monitoring Centre for Drugs and Drug Addiction. Archived from the original on 19 February 2012. Retrieved 23 March 2012. Centers for Disease Control and Prevention (CDC) (2010). "Syringe exchange programs --- United States, 2008". Morbidity and Mortality Weekly Report. 59 (45): 1488–1491. PMID 21085091. Islam, MM, Reid, SE, White, A, Grummett, S, Conigrave, KM and Haber, PS (2012). "Opportunistic and continuing health care for injecting drug users from a nurse-run needle syringe program-based primary health-care clinic". Drug Alcohol Rev. 31 (1): 114–115. doi:10.1111/j.1465-3362.2011.00390.x. PMID 22145983. Islam, M. M. (2010). "Needle Syringe Program-Based Primary HealthCare Centers: Advantages and Disadvantages". Journal of Primary Care & Community Health. 1 (2): 100–103. doi:10.1177/2150131910369684. PMID 23804370. S2CID 8663924. "Syringe Exchange Programs in the United States 2011" (PDF). amfAR, The Foundation for AIDS Research. Retrieved 25 March 2012. Wilkey, Robin (4 January 2012). "Needle Exchange Programs Lose Federal Funding: Local AIDS Programs Brace For Cuts". Huffington Post - San Francisco. Retrieved 25 March 2012. "Syringe exchange programs around the world: The global context" (PDF). Gay Men's Health Crisis. Retrieved 25 March 2012. Anderton, Jim. "Needle and syringe exchange programme saves lives". beehive.govt.nz, the official website of the New Zealand Government. Retrieved 26 March 2012. "Global State of Harm Reduction 2010" (PDF). International Harm Reduction Association. Retrieved 26 March 2012. Small, D.; Glickman, A.; Rigter, G.; Walter, T. (2010). "The Washington Needle Depot: Fitting healthcare to injection drug users rather than injection drug users to healthcare: Moving from a syringe exchange to syringe distribution model". Harm Reduction Journal. 7: 1. doi:10.1186/1477-7517-7-1. PMC 2806876. PMID 20047690. "Needle Exchange FAQs". Ontario Harm Reduction Distribution Program. Archived from the original on 30 December 2011. Retrieved 26 March 2012. Keyl, P. M.; Gruskin, L.; Casano, K.; Montag, H.; Junge, B.; Vlahov, D. (1998). "Community support for needle exchange programs and pharmacy sale of syringes: A household survey in Baltimore, Maryland". Journal of Acquired Immune Deficiency Syndromes and Human Retrovirology. 18 Suppl 1: S82–S88. doi:10.1097/00042560-199802001-00015. PMID 9663629. Aaron, Lawrence (2005-08-26). "Why a Needle-Exchange Program is a Bad Idea". redOrbit.com. Retrieved 26 March 2012. "Community consulted for the first time on attitudes towards drugs" (PDF). Anex. Archived from the original (PDF) on 28 July 2014. Retrieved 26 March 2012. Beletsky, L.; Grau, L. E.; White, E.; Bowman, S.; Heimer, R. (2011). "The roles of law, client race and program visibility in shaping police interference with the operation of US syringe exchange programs". Addiction. 106 (2): 357–365. doi:10.1111/j.1360-0443.2010.03149.x. PMC 3088513. PMID 21054615. Strathdee, S. A.; Patrick, D. M.; Currie, S. L.; Cornelisse, P. G.; Rekart, M. L.; Montaner, J. S.; Schechter, M. T.; O'Shaughnessy, M. V. (1997). "Needle exchange is not enough: Lessons from the Vancouver injecting drug use study". AIDS. 11 (8): F59–F65. doi:10.1097/00002030-199708000-00001. PMID 9223727. S2CID 12297178. Schechter, M. T.; Strathdee, S. A.; Cornelisse, P. G.; Currie, S.; Patrick, D. M.; Rekart, M. L.; O'Shaughnessy, M. V. (1999). "Do needle exchange programmes increase the spread of HIV among injection drug users?: An investigation of the Vancouver outbreak". AIDS. 13 (6): F45–F51. doi:10.1097/00002030-199904160-00002. PMID 10397556. Wood, E.; Lloyd-Smith, E.; Li, K.; Strathdee, S. A.; Small, W.; Tyndall, M. W.; Montaner, J. S. G.; Kerr, T. (2007). "Frequent Needle Exchange Use and HIV Incidence in Vancouver, Canada". The American Journal of Medicine. 120 (2): 172–179. doi:10.1016/j.amjmed.2006.02.030. PMID 17275459. Des Jarlais, D. C.; Arasteh, K.; Friedman, S. R. (2011). "HIV Among Drug Users at Beth Israel Medical Center, New York City, the First 25 Years". Substance Use & Misuse. 46 (2–3): 131–139. doi:10.3109/10826084.2011.521456. PMID 21303233. S2CID 26988253. Falster, K.; Kaldor, J. M.; Maher, L.; collaboration of Australian Needle Syringe Programs (2008). "Hepatitis C Virus Acquisition among Injecting Drug Users: A Cohort Analysis of a National Repeated Cross-sectional Survey of Needle and Syringe Program Attendees in Australia, 1995–2004". Journal of Urban Health. 86 (1): 106–118. doi:10.1007/s11524-008-9330-7. PMC 2629525. PMID 18979201. Wodak, A.; Maher, L. (2010). "The effectiveness of harm reduction in preventing HIV among injecting drug users" (PDF). New South Wales Public Health Bulletin. 21 (4): 69–73. doi:10.1071/NB10007. PMID 20513304. Delgado, C. (2004). "Evaluation of Needle Exchange Programs". Public Health Nursing. 21 (2): 171–178. doi:10.1111/j.0737-1209.2004.021211.x. PMID 14987217. Islam, M. M.; Topp, L.; Day, C. A.; Dawson, A.; Conigrave, K. M. (2012). "The accessibility, acceptability, health impact and cost implications of primary healthcare outlets that target injecting drug users: A narrative synthesis of literature". International Journal of Drug Policy. 23 (2): 94–102. doi:10.1016/j.drugpo.2011.08.005. PMID 21996165. Shriver, M. (1998). "Needle exchange works". Newsline (People with AIDS Coalition of New York): 35. PMID 11367470. Knittel, A. K.; Wren, P. A.; Gore, L. (2010). "Lessons learned from a peri-urban needle exchange". Harm Reduction Journal. 7: 8. doi:10.1186/1477-7517-7-8. PMC 2868839. PMID 20429944. Topp, L.; Day, C. A.; Iversen, J.; Wand, H.; Maher, L.; Collaboration Of Australian, N. (2011). "Fifteen years of HIV surveillance among people who inject drugs: The Australian Needle and Syringe Program Survey 1995–2009". AIDS. 25 (6): 835–842. doi:10.1097/QAD.0b013e32834412cc. PMID 21192232. S2CID 21228670. Williams, C. T.; Ouellet, L. J. (2010). "Misdirected opposition: Evidence opposing "not in my back yard" arguments against syringe exchange programmes". International Journal of Drug Policy. 21 (5): 437–439. doi:10.1016/j.drugpo.2010.02.003. PMID 20233654. Todd, C. S.; Nasir, A.; Stanekzai, M.; Fiekert, K.; Rasuli, M.; Vlahov, D.; Strathdee, S. A. (2011). "Prevalence and correlates of HIV, syphilis, and hepatitis B and C infection and harm reduction program use among male injecting drug users in Kabul, Afghanistan: A cross-sectional assessment". Harm Reduction Journal. 8: 22. doi:10.1186/1477-7517-8-22. PMC 3180253. PMID 21867518. Zhang, L.; Yap, L.; Xun, Z.; Wu, Z.; Wilson, D. P. (2011). "Needle and syringe programs in Yunnan, China yield health and financial return". BMC Public Health. 11: 250. doi:10.1186/1471-2458-11-250. PMC 3102626. PMID 21507267. Ferrer-Castro, V.; Crespo-Leiro, M. R.; García-Marcos, L. S.; Pérez-Rivas, M.; Alonso-Conde, A.; García-Fernández, I.; Lorenzo-Guisado, A.; Sánchez-Fernández, J. L.; Seara-Selas, M.; Sanjosé-Vallejo, R. (2012). "Evaluation of needle exchange program at Pereiro de Aguiar prison (Ourense, Spain): Ten years of experience". Revista Espanola de Sanidad Penitenciaria. 14 (1): 3–11. doi:10.4321/s1575-06202012000100002. PMID 22437903. Lee, H. Y.; Yang, Y. H.; Yu, W. J.; Su, L. W.; Lin, T. Y.; Chiu, H. J.; Tang, H. P.; Lin, C. Y.; Pan, R. N.; Li, J. H. (2012). "Essentiality of HIV testing and education for effective HIV control in the national pilot harm reduction program: The Taiwan experience". The Kaohsiung Journal of Medical Sciences. 28 (2): 79–85. doi:10.1016/j.kjms.2011.10.006. PMID 22313534. Uusküla, A.; Des Jarlais, D. C.; Kals, M.; Rüütel, K.; Abel-Ollo, K.; Talu, A.; Sobolev, I. (2011). "Expanded syringe exchange programs and reduced HIV infection among new injection drug users in Tallinn, Estonia". BMC Public Health. 11: 517. doi:10.1186/1471-2458-11-517. PMC 3146432. PMID 21718469. Pinkerton, S. D. (2010). "Is Vancouver Canada's supervised injection facility cost-saving?". Addiction. 105 (8): 1429–1436. doi:10.1111/j.1360-0443.2010.02977.x. PMID 20653622. Zamani, S.; Vazirian, M.; Nassirimanesh, B.; Razzaghi, E. M.; Ono-Kihara, M.; Mortazavi Ravari, S.; Gouya, M. M.; Kihara, M. (2008). "Needle and Syringe Sharing Practices Among Injecting Drug Users in Tehran: A Comparison of Two Neighborhoods, One with and One Without a Needle and Syringe Program". AIDS and Behavior. 14 (4): 885–890. doi:10.1007/s10461-008-9404-2. PMID 18483849. S2CID 36532906. Chatterjee, A.; Sharma, M. (2010). "Moving from a project to programmatic response: Scaling up harm reduction in Asia". International Journal of Drug Policy. 21 (2): 134–136. doi:10.1016/j.drugpo.2009.12.004. PMID 20079618. Ngo, A. D.; Schmich, L.; Higgs, P.; Fischer, A. (2009). "Qualitative evaluation of a peer-based needle syringe programme in Vietnam". International Journal of Drug Policy. 20 (2): 179–182. doi:10.1016/j.drugpo.2007.12.009. PMID 18242971. Auerbach, J. D.; Smith, W. (2008). "Confronting the 'evidence' in evidence-based HIV prevention: Current scientific and political challenges". BETA Bulletin of Experimental Treatments for AIDS. 20 (4): 44–49. PMID 18814374. Wodak, Alex; McLeod, Leah (August 2008). "The role of harm reduction in controlling HIV among injecting drug users". AIDS. 22 (Suppl 2): S81–S92. doi:10.1097/01.aids.0000327439.20914.33. ISSN 0269-9370. PMC 3329723. PMID 18641473. "Interventions to prevent HIV risk behaviors". NIH Consensus Statement. 15 (2): 1–41. 1997. PMID 9505959. "Syringe Exchange Programs" (PDF). Centers for Disease Control. Retrieved 26 March 2012. "ABA Urges Federal Support for Syringe Exchange Programs". American Bar Association. Retrieved 26 March 2012. Stapleton, Stephanie (1997). "AMA endorses needle-exchange programs". American Medical News. "Needle Exchange Programs: Position Statement" (PDF). American Psychological Association. Retrieved 26 March 2012. "Drug use and HIV/AIDS" (PDF). Joint United Nations Programme on HIV/AIDS. Retrieved 26 March 2012. "2001 Annual report on the state of the drugs problem in the European Union | www.emcdda.europa.eu". www.emcdda.europa.eu. Retrieved 2022-01-05. |
低
しきい値療法プログラムサービスの影響を実証する無作為化臨床試験は
ないものの [33][34][48]
、利用可能な証拠、サービス利用への障壁、重症IDUの病院への遅い提示は、対象を絞り込んだ閾値の低いサービスの必要性を継続的に示唆している。
さら
に、HIVやC型肝炎の感染予防は、薬物注射をやめられない人、やめる気がない人でも明らかに可能であり、低閾値アプローチを用いている様々な国が、薬物
注射をする人の間でHIV感染の抑制または事実上の排除を達成している[49]
。米国国立衛生研究所[50]、米国疾病対策センター[51]、米国法曹協会[52]、米国医師会[53]、米国心理学会[54]、世界保健機関
[55]、欧州薬物・麻薬中毒監視センター[56]、その他多くの団体が針交換など閾値を低くするプログラムを推奨している。 文献 Islam, M. M.; Day, C. A.; Conigrave, K. M. (2010). 「Harm reduction healthcare: From an alternative to the mainstream platform?」. International Journal of Drug Policy. 21 (2): 131–133. doi:10.1016/j.drugpo.2010.01.001. PMID 20092999. ワール、ヘルゲ。「薬物乱用問題に対する包括的、学際的アプローチの要素としてのリスク低減」(PDF)。ポンピドゥー・グループ。2012年3月25日取得。 Rogers, S. J.; Ruefli, T. (2004). 「Does harm reduction programming make a difference in the lives of highly marginalized, at-risk drug users?」. Harm Reduction Journal. 1 (1): 7. doi:10.1186/1477-7517-1-7. PMC 420490. PMID 15171790. Islam, MM, Topp, L, Conigrave, KM, and Day, C (2013). 「『敷居の低い』薬物使用者向けサービスの定義:その基準とは?」. International Journal of Drug Policy. 24 (3): 220–222. doi:10.1016/j.drugpo.2013.03.005. PMID 23567101. Nealy, Eleanor C. (1997-11-07). 「Early Intervention with Active Drug and Alcohol Users in Community-Based Settings」. Journal of Chemical Dependency Treatment. 7 (1–2): 5–20. doi:10.1300/J034v07n01_02. ISSN 0885-4734. Elovich, R.E., & Cowing, M. (1995). 回復への準備:常習者がいる場所で治療を行う戦略。『ハームリダクションと変化へのステップ:トレーニング・ソースブック』ニューヨーク:ゲイ・メンズ・ヘルス・クライシス。 Latt, N.; Conigrave, K.; Marshall, J.; Saunders, J.; Marshall, J.; Nutt, D. (2009). アディクション・メディスン。オックスフォード大学出版局。ISBN 9780199539338。2011年6月4日オリジナルよりアーカイブ。 ウルフ、ダニエル(2007年8月1日)。「注射薬物使用者に対する抗レトロウイルス治療におけるパラドックス:アジアと旧ソ連におけるアクセス、服薬遵 守、構造的障壁」。『国際薬物政策ジャーナル』。注射薬物使用者に対するHIV治療とケア。18 (4): 246–254. doi:10.1016/j.drugpo.2007.01.012. ISSN 0955-3959. PMID 17689372. McCoy, C. B.; Metsch, L. R.; Chitwood, D. D.; Miles, C. (2001). 「薬物の使用と保健サービス利用の障壁」. Substance Use & Misuse. 36 (6–7): 789–806. doi:10.1081/ja-100104091. PMID 11697611. S2CID 23220436. マクドナルド、P(2002年)。「路上から歩道へ:注射薬物使用者のためのプライマリケアサービスの展開」。オーストラリアプライマリヘルスジャーナル。8: 65–69. doi:10.1071/PY02010. デジャレイ、D. C.; マクナイト、C.; ゴールドブラット、C.; パーチェス、D.(2009年)。「ハームリダクションをより良く行う:米国における注射針交換」. Addiction. 104 (9): 1441–1446. doi:10.1111/j.1360-0443.2008.02465.x. PMID 19215605. 「低敷居サービス」. 麻薬・麻薬依存症に関する欧州モニタリングセンター. 2012年2月19日アーカイブ。2012年3月23日取得。 疾病対策センター(CDC) (2010). 「注射器交換プログラム――米国、2008年」。 疾病率および死亡率週報。59 (45): 1488–1491. PMID 21085091. Islam, MM, Reid, SE, White, A, Grummett, S, Conigrave, KM and Haber, PS (2012). 「看護師が運営する注射針・注射器プログラムに基づくプライマリヘルスケアクリニックによる、注射薬物使用者の機会的継続的保健ケア」. Drug Alcohol Rev. 31 (1): 114–115. doi:10.1111/j.1465-3362.2011.00390.x. PMID 22145983. Islam, M. M. (2010). "Needle Syringe Program-Based Primary HealthCare Centers: 利点と欠点」. Journal of Primary Care & Community Health. 1 (2): 100–103. doi:10.1177/2150131910369684. PMID 23804370. S2CID 8663924. 「2011年米国における注射器交換プログラム」(PDF)。amfAR、エイズ研究財団。2012年3月25日取得。 ウィルキー、ロビン(2012年1月4日)。「注射針交換プログラムが連邦助成金を失う:地元エイズ対策プログラムは予算削減に備える」。ハフィントンポスト - サンフランシスコ。2012年3月25日取得。 「世界中の注射器交換プログラム:世界的な背景」(PDF)。ゲイ・メンズ・ヘルス・クライシス。2012年3月25日取得。 アンドートン、ジム。「注射針と注射器の交換プログラムが命を救う」。beehive.govt.nz、ニュージーランド政府の公式ウェブサイト。2012年3月26日取得。 「2010年 グローバル・ステート・オブ・ハームリダクション」(PDF)。国際ハームリダクション協会。2012年3月26日取得。 スモール、D.; グリックマン、A.; リヒター、G.; ウォルター、T. (2010年). 「ワシントン・ニードル・デポ:医療を注射薬物使用者向けに合わせるのではなく、注射薬物使用者に医療を合わせる:注射器交換プログラムから注射器配布モ デルへの移行」。Harm Reduction Journal. 7: 1. doi:10.1186/1477-7517-7-1. PMC 2806876. PMID 20047690. 「針交換に関するよくある質問」。オンタリオ州ハームリダクション配布プログラム。2011年12月30日オリジナルよりアーカイブ。2012年3月26日取得。 Keyl, P. M.; Gruskin, L.; Casano, K.; Montag, H.; Junge, B.; Vlahov, D. (1998).「針交換プログラムと薬局での注射器販売に対する地域社会の支援: ボルチモア、メリーランド州における世帯調査」。Journal of Acquired Immune Deficiency Syndromes and Human Retrovirology. 18 Suppl 1: S82–S88. doi:10.1097/00042560-199802001-00015. PMID 9663629. アーロン、ローレンス(2005年8月26日)。「なぜ針交換プログラムは良くないのか」。redOrbit.com。2012年3月26日取得。 「薬物に対する態度について、コミュニティが初めて協議された」 (PDF)。Anex。オリジナル(PDF)のアーカイブ。2014年7月28日取得。2012年3月26日取得。 Beletsky, L.; Grau, L. E.; White, E.; Bowman, S.; Heimer, R. (2011). 「米国の注射針交換プログラムの運営に対する警察の干渉の形成における法律、クライアントの民族、プログラムの可視性の役割」. Addiction. 106 (2): 357–365. doi:10.1111/j.1360-0443.2010.03149.x. PMC 3088513. PMID 21054615. Strathdee, S. A.; Patrick, D. M.; Currie, S. L.; Cornelisse, P. G.; Rekart, M. L.; Montaner, J. S.; Schechter, M. T.; O'Shaughnessy, M. V. (1997). 「Needle exchange is not enough: Lessons from the Vancouver injecting drug use study」. AIDS. 11 (8): F59–F65. doi:10.1097/00002030-199708000-00001. PMID 9223727. S2CID 12297178. Schechter, M. T.; Strathdee, S. A.; Cornelisse, P. G.; Currie, S.; Patrick, D. M.; Rekart, M. L.; O'Shaughnessy, M. V. (1999). 「Do needle exchange programmes increase the spread of HIV among injection drug users?: An investigation of the Vancouver outbreak」. AIDS. 13 (6): F45–F51. doi:10.1097/00002030-199904160-00002. PMID 10397556. Wood, E.; Lloyd-Smith, E.; Li, K.; Strathdee, S. A.; Small, W.; Tyndall, M. W.; Montaner, J. S. G.; Kerr, T. (2007). 「Frequent Needle Exchange Use and HIV Incidence in Vancouver, Canada」. The American Journal of Medicine. 120 (2): 172–179. doi:10.1016/j.amjmed.2006.02.030. PMID 17275459. デス・ジャレイ、D. C.; アラステ、K.; フリードマン、S. R. (2011年). 「ニューヨーク市ベスイスラエル医療センターにおける薬物使用者におけるHIV、最初の25年間」. Substance Use & Misuse. 46 (2–3): 131–139. doi:10.3109/10826084.2011.521456. PMID 21303233. S2CID 26988253. ファルスター、K.; カルダー、J. M.; メイハー、L.; オーストラリアの注射針・注射器プログラム共同研究(2008年)。「注射薬使用者におけるC型肝炎ウイルス感染:1995年から2004年のオーストラ リアにおける注射針・注射器プログラム参加者を対象とした国民の繰り返し横断調査の集団分析」。都市保健ジャーナル。86 (1): 106–118. doi:10.1007/s11524-008-9330-7. PMC 2629525. PMID 18979201. Wodak, A.; Maher, L. (2010). 「The effectiveness of harm reduction in preventing HIV among injecting drug users」 (PDF). New South Wales Public Health Bulletin. 21 (4): 69–73. doi:10.1071/NB10007. PMID 20513304. デルガド、C. (2004年). 「注射針交換プログラムの評価」。公衆衛生看護。21 (2): 171–178. doi:10.1111/j.0737-1209.2004.021211.x. PMID 14987217. Islam, M. M.; Topp, L.; Day, C. A.; Dawson, A.; Conigrave, K. M. (2012). 「The accessibility, acceptability, health impact and cost implications of primary healthcare outlets that target injecting drug users: A narrative synthesis of literature」. International Journal of Drug Policy. 23 (2): 94–102. doi:10.1016/j.drugpo.2011.08.005. PMID 21996165. Shriver, M. (1998). 「Needle exchange works」. Newsline (People with AIDS Coalition of New York): 35. PMID 11367470. Knittel, A. K.; Wren, P. A.; Gore, L. (2010). 「Lessons learned from a peri-urban needle exchange」. Harm Reduction Journal. 7: 8. doi:10.1186/1477-7517-7-8. PMC 2868839. PMID 20429944. Topp, L.; Day, C. A.; Iversen, J.; Wand, H.; Maher, L.; Collaboration Of Australian, N. (2011). 「Fifteen years of HIV surveillance among people who inject drugs: The Australian Needle and Syringe Program Survey 1995–2009」. AIDS. 25 (6): 835–842. doi:10.1097/QAD.0b013e32834412cc. PMID 21192232. S2CID 21228670. ウィリアムズ、C. T.; ウレット、L. J. (2010年). 「誤った反対意見:注射器交換プログラムに対する「ノット・イン・マイ・バックヤード」論争の反対意見の証拠」. 国際薬物政策ジャーナル. 21 (5): 437–439. doi:10.1016/j.drugpo.2010.02.003. PMID 20233654. トッド、C. S.; ナシル、A.; スタネックザイ、M.; フィカート、K.; ラズーリ、M.; ブラホフ、D.; ストラスディー、S. A. (2011年). 「アフガニスタンのカブールにおける男性の注射薬物使用者におけるHIV、梅毒、B型およびC型肝炎感染の有病率と関連要因、およびハームリダクションプ ログラムの利用:横断的評価」。Harm Reduction Journal. 8: 22. doi:10.1186/1477-7517-8-22. PMC 3180253. PMID 21867518. Zhang, L.; Yap, L.; Xun, Z.; Wu, Z.; Wilson, D. P. (2011). 「中国雲南省における注射針・注射器プログラムは保健と財政に利益をもたらす」. BMC公衆衛生. 11: 250. doi:10.1186/1471-2458-11-250. PMC 3102626. PMID 21507267. Ferrer-Castro, V.; Crespo-Leiro, M. R.; García-Marcos, L. S.; Pérez-Rivas, M.; Alonso-Conde, A.; García-Fernández, I.; Lorenzo-Guisado, A.; Sánchez-Fernández, J. L.; Seara-Selas, M.; Sanjosé-Vallejo, R. (2012). 「スペイン・オウレンセのペレイロ・デ・アギアル刑務所における針交換プログラムの評価:10年間の経験」. Revista Espanola de Sanidad Penitenciaria. 14 (1): 3–11. doi:10.4321/s1575-06202012000100002. PMID 22437903. リー、H. Y.; ヤン、Y. H.; ユー、W. J.; スー、L. W.; リン、T. Y.; チウ、H. J.; タン、H. P.; リン、C. Y.; パン、R. N.; リ、J. H. (2012). 「国民パイロット・ハームリダクション・プログラムにおける効果的なHIV対策のためのHIV検査と教育の必要性:台湾の経験」. 高雄医学雑誌. 28 (2): 79–85. doi:10.1016/j.kjms.2011.10.006. PMID 22313534. Uusküla, A.; Des Jarlais, D. C.; Kals, M.; Rüütel, K.; Abel-Ollo, K.; Talu, A.; Sobolev, I. (2011). 「エストニアのタリンにおける注射針交換プログラムの拡大と新規注射薬物使用者のHIV感染率の低下」. BMC公衆衛生. 11: 517. doi:10.1186/1471-2458-11-517. PMC 3146432. PMID 21718469. Pinkerton, S. D. (2010). 「Is Vancouver Canada's supervised injection facility cost-saving?」. Addiction. 105 (8): 1429–1436. doi:10.1111/j.1360-0443.2010.02977.x. PMID 20653622. Zamani, S.; Vazirian, M.; Nassirimanesh, B.; Razzaghi, E. M.; Ono-Kihara, M.; Mortazavi Ravari, S.; Gouya, M. M.; Kihara, M. (2008). "Needle and Syringe Sharing Practices Among Injecting Drug Users in Tehran: 2つの地区、1つは注射針・注射器プログラムあり、もう1つはプログラムなしの地区の比較」。AIDS and Behavior. 14 (4): 885–890. doi:10.1007/s10461-008-9404-2. PMID 18483849. S2CID 36532906. Chatterjee, A.; Sharma, M. (2010). 「Moving from a project to programmatic response: Scaling up harm reduction in Asia」. International Journal of Drug Policy. 21 (2): 134–136. doi:10.1016/j.drugpo.2009.12.004. PMID 20079618. Ngo, A. D.; Schmich, L.; Higgs, P.; Fischer, A. (2009). 「ベトナムにおけるピア主導の注射針プログラムの定性評価」. International Journal of Drug Policy. 20 (2): 179–182. doi:10.1016/j.drugpo.2007.12.009. PMID 18242971. オーバック, J. D.; スミス, W. (2008). 「エビデンスに基づくHIV予防における『エビデンス』への対処:現在の科学的および政治的課題」. BETA エイズの治療に関する実験的治療の会報. 20 (4): 44–49. PMID 18814374. Wodak, Alex; McLeod, Leah (2008年8月). 「注射薬物使用者におけるHIV抑制におけるハームリダクションの役割」. AIDS. 22 (Suppl 2): S81–S92. doi:10.1097/01.aids.0000327439.20914.33. ISSN 0269-9370. PMC 3329723. PMID 18641473. 「HIVリスク行動を防止するための介入」。NIHコンセンサスステートメント。15 (2): 1–41. 1997. PMID 9505959. 「注射器交換プログラム」(PDF)。疾病対策センター。2012年3月26日取得。 「ABA、注射器交換プログラムへの連邦支援を要請」。米国弁護士協会。2012年3月26日取得。 ステファニー・ステイプルトン(1997年)。「AMA、注射針交換プログラムを支持」。アメリカン・メディカル・ニュース。 「注射針交換プログラム:立場表明」(PDF)。米国心理学会。2012年3月26日取得。 「薬物使用とHIV/AIDS」(PDF)。国連合同エイズ計画。2012年3月26日取得。 「2001年欧州連合における薬物問題に関する年次報告書|www.emcdda.europa.eu」。www.emcdda.europa.eu。2022年1月5日取得。 |
| Low-threshold treatment programs | https://www.deepl.com/ja/translator |
| Initiation for first contact IDUs In English, Van Gennep's first sentence of his first chapter begins: "Each larger society contains within it several distinctly separate groupings. ... In addition, all these groups break down into still smaller societies in subgroups." The population of a society belongs to multiple groups, some more important to the individual than others. Van Gennep uses the metaphor, "as a kind of house divided into rooms and corridors." A passage occurs when an individual leaves one group to enter another; in the metaphor, he changes rooms. Van Gennep further distinguishes between "the secular" and "the sacred sphere." Theorizing that civilizations are arranged on a scale, implying that the lower levels represent "the simplest level of development," he hypothesizes that "social groups in such a society likewise have magico-religious foundations." Many groups in modern industrial society practice customs that can be traced to an earlier sacred phase. Passage between these groups requires a ceremony, or ritual hence rite of passage. The rest of Van Gennep's book presents a description of rites of passage and an organization into types, although in the end he despairs of ever capturing them all:[4] "It is but a rough sketch of an immense picture ...." He is able to find some universals, mainly two: "the sexual separation between men and women, and the magico-religious separation between the profane and the sacred." (Earlier the translators used secular for profane.) He refuses credit for being the first to recognize type of rites. In the work he concentrates on groups and rites individuals might normally encounter progressively: pregnancy, childbirth, initiation, betrothal, marriage, funerals and the like. He mentions some others, such as the territorial passage, a crossing of borders into a culturally different region, such as one where a different religion prevails. |
●標的型ヘルスケアに初めてアクセスする薬物利用者には、加入儀礼(イニシエーション)的側面がある——仮説 Van Gennepの第1章の最初の文章(英訳)はこう始まる。 「それぞれの大きな社会は、その中にいくつかの明確に分離したグループを含んでいる。... さらに、これらのグループはすべて、サブグループのさらに小さな社会に分解される。" 社会の人口は複数のグループに属しており、その中には個人にとって他よりも重要なものもある。Van Gennepは、"部屋と廊下に分かれた一種の家のようなもの "という比喩を使っています。通過とは、個人があるグループから別のグループに入ることであり、この比喩では部屋を変えることを意味する。 さらにVan Gennepは、「世俗的なもの」と「神聖なもの」を区別している。文明は規模に応じて配置されており、下位のレベルは「最も単純な発展レベル」であるこ とを示唆しており、彼は「そのような社会の社会集団は、同様に魔術的・宗教的な基盤を持っている」という仮説を立てている。現代の産業社会では、初期の神 聖な段階にまで遡ることができる習慣を実践している集団が多い。このような集団の間を行き来するには、儀式、つまり通過儀礼が必要である。 Van Gennepの本の残りの部分では、通過儀礼の説明とタイプ別の構成が紹介されているが、最終的にはすべてを把握することはできないと絶望している [4]。「それは、巨大な絵の大まかなスケッチにすぎない....」。 彼はいくつかの普遍性を見出すことができたが、その主なものは次の2つである。"男性と女性の間の性的な分離と、俗物と聖物の間の魔術的・宗教的な分離 "である。(彼は、儀式の種類を最初に認識したという功績を認めていない。彼はこの著作の中で、妊娠、出産、入会、婚約、結婚、葬儀など、個人が通常段階 的に遭遇するであろうグループや儀式に焦点を当てている。他にも、国境を越えて文化的に異なる地域、例えば異なる宗教が支配する地域に入る「領土通過」な どについても言及している。 |
| ●しきいを下げるための孤独対策について考える |
|
| Jo Cox Commission on Loneliness https://en.wikipedia.org/wiki/Jo_Cox_Commission_on_Loneliness The Jo Cox Commission on Loneliness was an establishment set up by British Member of parliament Jo Cox, in order to investigate ways to reduce loneliness in the United Kingdom. It published its final report at the end of 2017. While only running for just over a year, the commission led to the UK government making a lasting commitment to loneliness relief. |
孤独に関するジョー・コックス委員会は、イギリスの孤独を減らす方法を
調査するために、イギリスの国会議員であるジョー・コックスによって設立された施設です。2017年末に最終報告書を発表した。わずか1年あまりの運営期
間でしたが、この委員会をきっかけに、英国政府は孤独の解消に永続的に取り組むことになりました。 |
| The commission was established
by Jo Cox shortly before her death in the summer of 2016. It was always
intended to be a cross-party endeavour, with the Tory MP Seema Kennedy
a leading member from the start. In January 2017 the commission was
re-launched by Kennedy and the Labour MP Rachel Reeves; the two went on
to serve as co-chairs of the commission. Working together with 13
charities, including Age UK and Action for Children, the commission
produced a report outlining ways to combat loneliness in the UK. With
Jo having planned for the commission to only run for one year, the
commission was wound up in early 2018, shortly after producing its
final report.[1][2][3][4] |
この委員会は、2016年夏に亡くなる直前のジョー・コックスによって
設立されました。当初から党派を超えた取り組みとして意図されており、トリー派のシーマ・ケネディ議員が主要メンバーとして参加していました。2017年
1月、ケネディと労働党のレイチェル・リーヴス議員によって委員会は再スタートし、2人は委員会の共同議長を務めることになりました。Age
UKやAction for
Childrenを含む13の慈善団体と協力し、委員会は英国における孤独と闘う方法をまとめた報告書を作成しました。ジョーは委員会の運営期間を1年間
だけと計画していたため、委員会は最終報告書を作成した直後の2018年初頭に解散した[1][2][3][4]。 |
| The final report was released in
December 2017 and had recommendations in three areas: National leadership, including the nomination of a lead minister. Measurement, involving developing a national indicator and annual reporting. Funding, for unspecified initiatives. The report made clear that government alone would not be able to solve the problem of loneliness, with the commission also calling for action from other public sector leaders, business leaders, community and volunteer groups and regular citizens.[3][5] [4] |
最終報告書は2017年12月に発表され、3つの領域で提言がなされま
した: 主席大臣の指名を含む、国のリーダーシップ。 測定、国家指標の開発と年次報告を含む。 資金調達、不特定多数のイニシアチブのための資金調達。 報告書は、政府だけでは孤独の問題を解決できないことを明確にし、委員会は他の公共部門のリーダー、ビジネスリーダー、コミュニティやボランティアグルー プ、一般市民の行動も求めている[3][5][4]。 |
| Jo's friend Rachel Reeves
continued to lead an all party group working on loneliness even after
the commission was wound up. As of 2020 The Jo Cox Foundation still
works on the problem of loneliness in partnership with government and
with other charities.[2][1] In January 2018, prime minister Theresa May accepted the final report's recommendations, creating a ministerial lead for loneliness, with the intention that the new role will ensure loneliness reduction remains an enduring parliamentary priority. The position is often referred to by the media as the 'Minister for Loneliness' , though it is not a separate ministerial office. Initially the role was an expansion of the remit for the Minister for Sport and Civil Society. The post was first held by Tracey Crouch, then from November 2018 to July 2019 by Mims Davies, and as of 2020 is held by Baroness Barran. In October 2018, again as a result of the final report, the UK government became the first in the world to publish a loneliness reduction strategy. The strategy included commitments for loneliness reduction activity by nine different government departments; for example to encourage "social prescribing" by front line doctors, so that they can refer patients suffering from loneliness to local group activity & befriending schemes. As of May 2020, the UK government has distributed over £20 million to various initiatives to reduce loneliness. This initiative includes funding to charities dedicated to combatting loneliness, and to loneliness reduction projects run by both tech firms and community groups.[3][6][7][8][1 |
ジョーの友人であるレイチェル・リーヴスは、委員会が解散した後も、孤
独に取り組む全政党のグループを率い続けている。2020年現在、ジョー・コックス財団は、政府との連携や他の慈善団体と協力して孤独の問題に取り組んで
います[2][1]。 2018年1月、テリーザ・メイ首相は最終報告書の提言を受け入れ、孤独を担当する閣僚の主席を創設し、この新しい役割により、孤独の解消が議会の永続的 な優先事項であり続けることを意図している。この役職は、メディアでは「孤独担当大臣」と呼ばれることが多いが、別の大臣室ではない。当初、この役職は、 スポーツ・市民社会担当大臣の権限を拡大したものでした。このポストは最初トレイシー・クラウチが務め、2018年11月から2019年7月まではミム ス・デイヴィスが務め、2020年現在ではバラン男爵夫人が務めている。2018年10月、やはり最終報告の結果、英国政府は世界で初めて孤独解消戦略を 発表しました。この戦略には、9つの異なる政府省庁による孤独解消活動のコミットメントが含まれており、例えば、第一線の医師による「社会的処方」を奨励 し、孤独に苦しむ患者を地域のグループ活動&親睦スキームに紹介できるようにすることなどが挙げられています。2020年5月現在、英国政府は孤独を減ら すためのさまざまな取り組みに2,000万ポンド以上を分配しています。この取り組みには、孤独と闘うことを目的とした慈善団体への資金提供や、テック企 業やコミュニティグループの両方が運営する孤独解消プロジェクトへの資金提供が含まれています[3][6][7][8][1]。 |
| 孤独・孤立対策官民連携プラットフォーム https://www.cas.go.jp/jp/seisaku/kodoku_koritsu_platform/history/index.html |
|
| Primary healthcare outlets that
target injecting drug users: Opportunity to make services accessible
and acceptable to the target group, by M.
Mofizul Islam a b, Libby Topp c, Carolyn A. Day b d, Angela Dawson e,
Katherine M. Conigrave b d f |
注射薬物使用者を対象とした一次医療機関:
対象グループが利用しやすく、受け入れやすいサービスを提供する機会 |
| Six experts from different
regions of the world commented on our original paper (Islam, Topp, Day,
Dawson, & Conigrave, 2012) and despite their different opinions and
perspectives, all agree that providing anonymous, non-judgmental and
free-of-charge services under a harm reduction framework can increase
the accessibility and acceptability of primary healthcare (PHC) for
injecting drug users (IDUs). Nasiri (2012) and Bruce (2012) point out
that the conventional model of healthcare will fail if we presume the
needs of IDUs based on our own understandings; we must listen to and
observe our clients and adapt services accordingly. Both Nasiri and
Bruce recommend integrated, accessible services for IDUs, a notion
supported by the literature (Campbell et al., 2007, Umbricht-Schneiter
et al., 1994). Nasiri goes so far as to argue that for many IDUs,
offering referrals only is akin to denying services. Rowe (2012) points out the political and cultural environment in which PHC services for IDUs are established vary greatly. Nonetheless, we identified a number of common elements, including a harm reduction focus, suitable locations and drop-in arrangements. These approaches are crucial whether IDU-targeted health services are in Sydney, Nepal or Iran. As Nasiri and Bruce point out, service utilisation by IDUs is often determined by convenience, immediate satisfaction and respect, unless the perceived need for services is very high. But certainly the final ‘shape’ of any facility aiming to service IDUs will be influenced by local variables. Myers (2012) identifies the difficulties of offering PHCs to IDUs in low and middle income countries where needle and syringe programs (NSPs) and opioid substitution treatment services are either absent or coverage is poor. She suggests that existing services for similarly high-risk populations, such as sex-workers and men who have sex with men, may be well suited to providing PHC for IDUs; that indeed, given the considerable overlap in these populations, such services may be expanded to provide NSP. This makes good sense for countries where services for these high-risk groups exist, however many developing countries lack even minimal services for these groups (Islam & Conigrave, 2008). In such settings, continued attempts to gradually mainstream harm reduction services (Islam, Day, & Conigrave, 2010) may be the only viable option. Myers supports this suggestion and also recommends consideration of peer-led services, an approach well worth exploration in resource-poor settings. As Ford (2012) notes, it is difficult to measure the effectiveness of existing healthcare services, such as general practices (GPs), in caring for the needs of IDUs. Although we specifically excluded office-based PHC services from our original review, we strongly agree that direct support for GPs in caring for IDUs is valuable and there is much to learn from the experience of such initiatives. Clinicians, however, are likely to vary considerably in their level of preparedness and ability to deal with IDUs, regardless of available support (McKeown, Matheson, & Bond, 2003). van Beek's (2012) comments address concerns raised by Rowe and Ford, in particular the difficulties of collecting robust evidence on the effectiveness of IDU-targeted PHC services. This, of course, is one reason why the scientific literature on this subject is so sparse. Any study which could accurately measure effectiveness would most likely be expensive – and in reality, may need to be implemented as part of the establishment phase of a series of PHC centers. Multiple baseline methodology is one approach advocated where an RCT is either impractical or ethically indefensible (Sanson-Fisher, Bonevski, Green, & D’Este, 2007). We contend that more discussion and access to published evaluations, even those employing below “gold standard” methodology, will increase discourse about appropriate methods of evaluation. This in turn may lead to the development of evaluation-guidelines which can foster quality assessments, suitable for publication in academic journals, thereby increasing the accessibility of relevant literature to policymakers and service providers. Evaluations would necessarily, as Rowe points out, include client feedback. However, as highlighted by van Beek, client feedback is limited by selection bias, because only clients who are reasonably satisfied with a service (or desperate) tend to continue to use that service. Feedback may also be subject to social desirability bias. The available evidence, revealing barriers to service access and the late presentation of seriously ill IDUs to hospital, suggests the ongoing need for targeted PHC services. If conventional healthcare facilities evolve to offer safe and accessible environments which attract IDUs, targeted healthcare outlets may no longer be a priority. However, this time is yet to come. Undoubtedly, rigorous evaluation is still required to guide policymakers and clinicians in further improving service provision. However, it is imperative that IDUs are offered acceptable and accessible healthcare even whilst we await quality evidence to guide best practice. Consequently, gradual expansion and replication of PHC for IDUs are (and should be) continuing, although geographical coverage remains limited. |
私たちの原著論文(Islam, Topp, Day,
Dawson, & Conigrave,
2012)には、世界の異なる地域から6人の専門家がコメントを寄せており、意見や視点は異なるものの、危害軽減の枠組みの下で匿名、非審判、無料のサー
ビスを提供することで、注射薬物使用者(IDUs)に対するプライマリー・ヘルスケア(PHC)のアクセシビリティとアクセプタビリティを高めることがで
きるという点では、全員が同意している。Nasiri(2012)とBruce(2012)は、自分たちの理解に基づいてIDUのニーズを推測すると、従
来の医療モデルは失敗すると指摘している。ナシリもブルースも、IDUのために統合された利用しやすいサービスを推奨しているが、これは文献
(Campbell et al.) ナシリは、多くのIDUにとって、紹介だけを提供することはサービスを拒否することと同じだとまで主張している。 Rowe (2012)は、IDUのためのPHCサービスが確立される政治的・文化的環境は大きく異なると指摘している。それにもかかわらず、害の軽減に重点を置い ていること、適切な場所であること、ドロップインが可能であることなど、多くの共通点がある。これらのアプローチは、IDUを対象とした保健サービスがシ ドニーであろうと、ネパールであろうと、イランであろうと、極めて重要である。NasiriとBruceが指摘するように、IDUによるサービスの利用 は、サービスに対する必要性の認識が非常に高くない限り、利便性、即時的な満足度、敬意によって決定されることが多い。しかし、IDUにサービスを提供す ることを目的とした施設の最終的な「形」は、地域の変数に影響されることは確かである。 Myers(2012)は、注射針・注射器プログラム(NSP)やオピオイド代替治療サービスが存在しないか、カバー率が低い中低所得国で、IDUに PHCを提供することの難しさを明らかにしている。彼女は、セックスワーカーや男性と性交渉を持つ男性など、同様のハイリスク集団に対する既存のサービス が、IDUに対するPHCの提供に適している可能性があることを示唆している。実際、これらの集団がかなり重複していることを考えると、そのようなサービ スはNSPを提供するために拡大される可能性がある。これらのハイリスク集団に対するサービスが存在する国にとっては、これは理にかなったことであるが、 多くの発展途上国では、これらの集団に対する最低限のサービスさえも欠如している(Islam & Conigrave, 2008)。そのような環境では、徐々にハームリダクションサービスを主流化する試みを続けること(Islam, Day, & Conigrave, 2010)が、唯一の実行可能な選択肢かもしれない。Myersはこの提案を支持し、ピア主導のサービスの検討も推奨しているが、これは資源の乏しい環境 では十分に検討に値するアプローチである。 Ford (2012)が指摘するように、IDUのニーズをケアする上で、一般診療所(GP)のような既存のヘルスケアサービスの有効性を測定することは難しい。当 初のレビューでは、特に事務ベースのPHCサービスを除外したが、IDUのケアにおけるGPへの直接支援は貴重であり、そのような取り組みの経験から学ぶ ことは多いという点には強く同意する。しかし、臨床医は、利用可能な支援にかかわらず、IDUsに対処するための準備と能力のレベルにはかなりの差がある と思われる(McKeown, Matheson, & Bond, 2003)。 van Beek (2012)のコメントは、RoweとFordが提起した懸念、特にIDUを対象としたPHCサービスの有効性につ いて確実な証拠を集めることの難しさに言及している。もちろん、これがこの問題に関する科学的文献がまばらな理由の一つである。有効性を正確に測定できる ような研究は、ほとんどの場合費用がかかり、現実には、一連のPHCセンターの設立段階の一部として実施する必要があるかもしれない。多重ベースライン法 は、RCTが現実的でない、あるいは倫理的に擁護できない場合に提唱される方法の一つである(Sanson-Fisher, Bonevski, Green, & D'Este, 2007)。私たちは、「ゴールドスタンダード」以下の方法論を採用したものであっても、公表された評価についてより多くの議論がなされ、アクセスできる ようになることで、適切な評価方法についての議論が深まると主張する。その結果、学術誌に掲載するのに適した質の高い評価を促進する評価ガイドラインが策 定され、政策立案者やサービス提供者が関連文献にアクセスしやすくなる可能性がある。ロウが指摘するように、評価には必ずクライアントのフィードバックが 含まれる。しかし、van Beekが強調したように、クライアントのフィードバックは選択バイアスによって制限される。なぜなら、あるサービスにそれなりに満足している(あるいは 絶望している)クライアントだけが、そのサービスを利用し続ける傾向があるからである。フィードバックはまた、社会的望ましさバイアス(social desirability bias)の影響を受けるかもしれない。 サービス利用への障壁や重症IDUの病院受診の遅れを明らかにした利用可能な証拠は、ターゲットを絞ったPHCサービスの継続的な必要性を示唆している。 従来の医療施設が、IDUを惹きつける安全で利用しやすい環境を提供するように進化すれば、ターゲットを絞った医療施設はもはや優先事項ではなくなるかも しれない。しかし、その時はまだ来ていない。政策立案者や臨床医がサービス提供をさらに改善するためには、間違いなく厳密な評価が必要である。しかし、ベ ストプラクティスの指針となる質の高いエビデンスを待つ間にも、IDUが受け入れ可能で利用しやすい医療を提供することが不可欠である。その結果、 IDUsのためのPHCの漸進的な拡大と複製は、地理的な範囲は限定されたままではあるが、継続されている(はずである)。 |
| Social
Stigma Addiction and substance use disorders Throughout history, addiction has largely been seen as a moral failing or character flaw, as opposed to an issue of public health.[56][57][58] Substance use has been found to be more stigmatized than smoking, obesity, and mental illness.[56][59][60][61] Research has shown stigma to be a barrier to treatment-seeking behaviors among individuals with addiction, creating a "treatment gap".[62][63][64] A systematic review of all epidemiological studies on treatment rates of people with alcohol use disorders found that over 80% had not accessed any treatment for their disorder.[65] The study also found that the treatment gap was larger in low and lower-middle-income countries. Research shows that the words used to talk about addiction can contribute to stigmatization, and that the commonly used terms of "abuse" & "abuser" actually increase stigma.[66][67][68][69] Behavioral addictions (i.e. gambling, sex, etc.) are found to be more likely to be attributed to character flaws than substance-use addictions.[70] Stigma is reduced when Substance Use Disorders are portrayed as treatable conditions.[71][72] Acceptance and Commitment Therapy has been used effectively to help people to reduce shame associated with cultural stigma around substance use treatment.[73][74][75] The use of the drug methamphetamine has been strongly stigmatized. An Australian national population study have shown that the proportion of Australians who nominated methamphetamine as a "drug problem" increased between 2001–2019.[76] The epidemiological study provided evidence that levels of under-reporting have increased over the period, which coincided with the deployment of public health campaigns on the dangers of ice that had stigmatizing elements that portrayal of persons who used the drugs in a negative way.[76] The level of under-reporting of methamphetamine use is strongly associated with increasing negative attitudes towards their use over the same period.[76] https://en.wikipedia.org/wiki/Social_stigma |
社
会的スティグマ 依 存症と薬物使用障害 歴史を通じて、依存症は公衆衛生の問題とは対照的に、道徳的な失敗や性 格的欠陥と見なされてきた。[56][57][58] 薬物使用は、喫煙、肥満、精神疾患よりもスティグマ化されていることが判明している。 [62][63][64] アルコール使用障害者の治療率に関するすべての疫学研究の系統的レビューによると、80%以上が自分の障害の治療を一切受けていないことがわかった [65]。 この研究はまた、低・中所得国で治療格差がより大きいことも明らかにした。 研究によると、依存症について話す際に使用される言葉がスティグマ化の 一因となる可能性があり、「乱用」「乱用者」という一般的に使用される用語は、実際にスティグマを増大させる[66][67][68][69]。行動依存 症(ギャンブル、セックスなど)は、物質使用依存症よりも性格的欠陥に起因する可能性が高いことがわかっている。 [70] 薬物使用障害が治療可能な状態として描かれることで、スティグマは軽減される。 [71][72] 受容とコミットメント療法は、薬物使用治療をめぐる文化的スティグマに関連する羞恥心を軽減するために効果的に用いられている。 メタンフェタミンという薬物の使用は強くスティグマ化されている。オー ストラリアの全国人口調査によると、覚せい剤を「薬物問題」として指名するオーストラリア人の割合が2001年から2019年の間に増加した[76]。こ の疫学調査では、過少申告のレベルがこの期間に増加したという証拠が示されており、これは、薬物を使用する人を否定的に描くスティグマ的要素を持つ氷の危 険性に関する公衆衛生キャンペーンが展開された時期と一致している[76]。覚せい剤使用の過少申告のレベルは、同じ期間にその使用に対する否定的な態度 が増加したことと強く関連している[76]。 |
基本用語の整理
| 低しきい療法プログラム, LTTプログラム |
Low-threshold treatment programs | 薬物使用者を対象としたハームリダクション(HR)に基づくヘルスケアに中心化されたものであ り、患者への要求を最小限に抑え、薬物の摂取量をコントロールしようとせずにサービスを提供し、要求された場合のみカウンセリングを提供するプログラムの ことである。 |
| 高いしきいプログラム, HTTプログラム |
High-threshold treatment programs | 薬物利用者に、支援の前提として患者にカウンセリングの受け入れとすべ ての薬物使用の中止を要求するもの。 |
| 注射針交換プログラム |
Needle exchange programs, Needle-Syringe exchange programs (NSP) | Needle
and syringe programmes (注
射器・注射針プログラム)とも言う。注射器利用の薬物利用者( injecting drug users ,
IDUs)に対して清潔で未使用の注射針や必要関連用具(結紮バンド、アルコール、脱脂綿、注射液小皿など)を無償提供し、HIV/AIDSや肝炎の防止
のためにおこなう、ハームリダクション手法。 |
| ハームリダクション |
Harm Reduction, HR |
ハーム・リダクションとは、個人ならびに社会がもた
らす危害(ハーム、 harm)を軽減する(リダクション、reduction)ための社会実践のことであり、公衆衛生および社会政策
上の概念枠組み・実践モデルのひとつとして提唱されているもの。 |
| 回復、リカバリー |
recovery | 薬物利用からのリカバリーすなわち「回復」とは、薬物をつかわないよう
になる状態のことをいう。薬物利用経験のない人からみれば、回復は極めて当たり前で正常な状態であると考えられる。しかし、多くの薬物利用者には、そのよ
うな回復が、心理的および社会的プレッシャーになると、回復から足が遠のくと言われている。回復を望む利用者の身体的・心理的・社会的困難を軽減するため
にハームリダクションやしきい値の低いアプローチが提案されている。 |
| 標的型ヘルスケア支所、低しきい値ヘルスケア支所(注射器利用の薬物使 用者のための〜) | targeted health care outlet or
low-threshold health care outlet for IDUs |
患者への要求を最小限に抑え、薬物の摂取量をコントロールしようとせず にサービスを提供し、要求された場合のみカウンセリングを提供するプログラム、すなわち低しきい療法プログラムを提供するヘルスケアの支所(=拠点)の こと。標的とは、さまざまな社会的リスクを抱えている注射器利用の薬物使用者(IDUs)のことである。 |
| ドロップイン |
drop-in |
drop in
とはふらりと立ち寄ることであるので、薬物利用者が、犯罪行為や医療の監視対象とみなされず、ふらりと自由に立ち寄れるような環境を、そのような探求行動
をドロップインと呼ぶ。 |

Contents of a needle-exchange
kit(注射針交換プログラムキットの実例)
※文中のしきい値は、今後、しきい(あるいは敷居)と改める計画ですので、実際に「しきい 値」と表記してあっても、「しきい」と読み替えてください。
| There are those who
are more likely to be marginalized and invisibilized due to prejudice
and the effects of stigma, and who are more likely to stay away from
the mainstream support system. Drug users are one such example. In this
study, we consider "not using help" as a situation in which "choice" to
use public services is not a part of the individual's problem-solving
process or seeking help due to current interpretations of the
situation, the resources they have, and their past experiences. The
study examines the service gap, service access, and support programs
for drug users within the framework of "low-threshold services. |
偏見やスティグマの効果などから周縁化・不可視化されやすく、メインス
トリームの支援制度から遠ざかりやすい人たちがいる。薬物使用者らは、その例に含まれる。本研究では、「援助を用いない」という事象を、現在の状況解釈
や、保有する資源、過去の経験などによって、個人の問題解決プロセスや求助行動の中に、公的なサービスの利用という「選択」が働かない状況として、捉え
る。そして、薬物使用者の、サービスギャップとサービスアクセス、支援プログラムのあり方について「しきいの低いサービス(low-threshold
service)」という枠組みの中で検討する。 |
| This study takes a "low
threshold services" approach to address the issue of access to services
for drug users and others vulnerable to prejudice and stigma in Japan.
During the past six years of research activities, the principal
investigators have examined the concept of "harm reduction" as a
complement to the traditional view of support for recovery from
addiction. This research aims to open the way to a new view of support
in community care by focusing on the approach of "low threshold
services" following "harm reduction. The fiscal year 2021 was the first year of this research, and among the four tasks set forth in the research plan, we tackled Research Project 1, "Literature review and collection of basic information," and Research Project 2, "Study of research methods including digital ethnography and establishment of a research system. For Research Project 1, we organized the materials and information collected in previous studies and clarified additional information needed. In preparation for the collection of case studies in Japan and Europe, an additional researcher was assigned to conduct a survey of materials. In addition, information was collected through online participation in domestic and international conferences and practitioners' meetings related to HIV and drug use. For Research Project 2, a study group was held on digital ethnography methods, led by Ikeda, the co-researcher, and Suh, the principal investigator, prepared a research presentation at the conference of the Japanese Society of Health and Behavioral Sciences to be held in June 2022. In addition, Dr. Suh is preparing a monograph as a report on the results of his research on drug user support, and has incorporated some of the results of this research into the content of his writing. Suh cooperated with news media (newspapers and newspaper websites) by providing information and conducting interviews. |
本研究では、「しきいの低いサービス」というアプローチを取り上げ、日
本における薬物使用者他、偏見やスティグマの影響を受けやすい人たちのサービスアクセスの問題に取り組む。過去6年間の研究活動の中、研究代表者らは、従
来の依存症からの「回復支援」という支援観を補完する「ハームリダクション」という概念を取り上げ検討してきた。本研究では、「ハームリダクション」につ
いで「しきいの低いサービス」というアプローチに注目することにより、コミュニティ・ケアにおける、新しい支援観への道筋を開くことを目標とする。 2021年度は当該研究の初年次であり、研究計画で設定した4つの課題のうち、研究課題1「文献検討と基礎情報の収集」および研究課題2「デジタル・エス ノグラフィーを含む調査方法の検討と体制構築」に取り組んだ。研究課題1については、これまでの研究にて収集した資料・情報を整理し、追加で必要となる情 報を明確化した。日本およびヨーロッパにおける事例収集の準備として、分担研究者を追加し資料調査を行った。また、HIVや薬物使用にかかわる国内外の学 会・実践家集会にオンラインで参加し、情報収集を行った。 研究課題2については、分担研究者・池田を中心に、デジタル・エスノグラフィーの手法について研究会を行い、研究代表者・徐は、2022年6月開催の日本 保健医療行動科学会大会における研究発表を準備した。また、徐は、これまでの薬物使用者支援にかかわる研究の成果報告として単著を準備中であり、執筆内容 に当該研究の成果を一部取り入れた。報道メディア(新聞および新聞社のウェブサイト)への取材協力(情報提供およびインタビュー)を行った。 |
| https://kaken.nii.ac.jp/grant/KAKENHI-PROJECT-21K18460/ |
☆プライマリー・ヘルス・ケア(PHC)
| Primary
health care (PHC) is "essential health care" that is based on
scientifically sound and socially acceptable methods and technology.
This makes universal health care accessible to all individuals and
families in a community. PHC initiatives allow for the full
participation of community members in implementation and decision
making.[1] Services are provided at a cost that the community and the
country can afford at every stage of their development in the spirit of
self-reliance and self-determination.[2] In other words, PHC is an
approach to health beyond the traditional health care system that
focuses on health equity-producing social policy.[3][4] PHC includes
all areas that play a role in health, such as access to health
services, environment and lifestyle.[5] Thus, primary healthcare and
public health measures, taken together, may be considered as the
cornerstones of universal health systems.[6] The World Health
Organization, or WHO, elaborates on the goals of PHC as defined by
three major categories, "empowering people and communities,
multisectoral policy and action; and primary care and essential public
health functions as the core of integrated health services[1]." Based
on these definitions, PHC cannot only help an individual after being
diagnosed with a disease or disorder, but can actively contribute to
preventing such issues by understanding the individual as a whole. This ideal model of healthcare was adopted in the declaration of the International Conference on Primary Health Care held in Alma Ata, Kazakhstan in 1978 (known as the "Alma Ata Declaration"), and became a core concept of the World Health Organization's goal of Health for all.[7] The Alma-Ata Conference mobilized a "Primary Health Care movement" of professionals and institutions, governments and civil society organizations, researchers and grassroots organizations that undertook to tackle the "politically, socially and economically unacceptable" health inequalities in all countries. There were many factors that inspired PHC; a prominent example is the Barefoot Doctors of China.[5][8][9] |
プライマリーヘルスケア(PHC)とは、科学的に正しく、
社会的に受け入れられる方法と技術に基づいた「必要不可欠なヘルスケア」である。これによって、地域社会のすべての個人と家族が、普遍的なヘルスケアにア
クセスできるようになる。PHCの取り組みでは、実施や意思決定に地域社会の人々が全面的に参加することができる[1]。
サービスは、自立と自己決定の精神に基づき、地域社会や国が発展のあらゆる段階で負担できる費用で提供される[2]。言い換えれば、PHCは、健康の公平
性を生み出す社会政策に焦点を当てた、従来の医療制度を超えた健康へのアプローチである。
[3][4]PHCには、保健サービスへのアクセス、環境、ライフスタイルなど、健康に関与するすべての分野が含まれる[5]。したがって、プライマリ・
ヘルスケアと公衆衛生対策を合わせて、ユニバーサル・ヘルス・システムの礎石と考えることができる[6]。これらの定義に基づけば、PHCは病気や障害と
診断された個人を助けるだけでなく、個人を全体として理解することで、そのような問題の予防に積極的に貢献することができる。 このヘルスケアの理想的なモデルは、1978年にカザフスタンのアルマ・アタで開催された「プライマリ・ヘルスケア国際会議」の宣言(「アルマ・アタ宣 言」として知られる)で採用され、世界保健機関(WHO)が目指す「万人のための保健」の中核概念となった[7]。アルマ・アタ会議は、すべての国におけ る「政治的、社会的、経済的に容認できない」健康格差に取り組むために、専門家や機関、政府、市民社会組織、研究者、草の根組織からなる「プライマリ・ヘ ルスケア運動」を動員した。PHCを触発した要因は数多くあるが、その顕著な例が中国の「裸足の医者」である[5][8][9]。 |
Goals and principles A primary health care worker in Saudi Arabia, 2008 The ultimate goal of primary healthcare is the attainment of better health services for all. It is for this reason that the World Health Organization (WHO), has identified five key elements to achieving this goal:[10] reducing exclusion and social disparities in health (universal coverage reforms); organizing health services around people's needs and expectations (service delivery reforms); integrating health into all sectors (public policy reforms); pursuing collaborative models of policy dialogue (leadership reforms); and increasing stakeholder participation. Behind these elements lies a series of basic principles identified in the Alma Ata Declaration that should be formulated in national policies in order to launch and sustain PHC as part of a comprehensive health system and in coordination with other sectors:[2] Equitable distribution of health care – according to this principle, primary care and other services to meet the main health problems in a community must be provided equally to all individuals irrespective of their gender, age, caste, color, urban/rural location and social class. Community participation – in order to make the fullest use of local, national and other available resources. Community participation was considered sustainable due to its grass roots nature and emphasis on self-sufficiency, as opposed to targeted (or vertical) approaches dependent on international development assistance.[5] Health human resources development – comprehensive healthcare relies on an adequate number and distribution of trained physicians, nurses, allied health professions, community health workers and others working as a health team and supported at the local and referral levels. Use of appropriate technology – medical technology should be provided that is accessible, affordable, feasible and culturally acceptable to the community. Examples of appropriate technology include refrigerators for cold vaccine storage. Less appropriate examples of medical technology could include, in many settings, body scanners or heart-lung machines, which benefit only a small minority concentrated in urban areas. They are generally not accessible to the poor, but draw a large share of resources.[5] Multi-sectional approach – recognition that health cannot be improved by intervention within just the formal health sector; other sectors are equally important in promoting the health and self-reliance of communities. These sectors include, at least: agriculture (e.g. food security); education; communication (e.g. concerning prevailing health problems and the methods of preventing and controlling them); housing; public works (e.g. ensuring an adequate supply of safe water and basic sanitation); rural development; industry; community organizations (including Panchayats or local governments, voluntary organizations, etc.). In sum, PHC recognizes that healthcare is not a short-lived intervention, but an ongoing process of improving people's lives and alleviating the underlying socioeconomic conditions that contribute to poor health. The principles link health, development, and advocating political interventions rather than passive acceptance of economic conditions.[5] |
目標と原則 2008年、サウジアラビアのプライマリ・ヘルスケア従事者 プライマリ・ヘルスケアの究極の目標は、すべての人々により良い医療サービスを提供することである。このため、世界保健機関(WHO)は、この目標を達成 するための5つの重要な要素を挙げている[10]。 健康における排除と社会的格差を減らす(ユニバーサル・カバレッジ改革); 人々のニーズと期待を中心に保健サービスを組織化する(サービス提供改革); 保健をあらゆる分野に統合する(公共政策改革); 政策対話の協調モデルを追求する(リーダーシップ改革)。 利害関係者の参加の促進 これらの要素の背後には、アルマ・アタ宣言で明らかにされた一連の基本原則があり、PHCを包括的な保健システムの一部として、また他のセクターと協調し ながら立ち上げ、持続させるために、国家政策として策定されるべきである[2]。 ヘルスケアの衡平な配分-この原則によれば、プライマリー・ケアや、地域社会の主な健康問題に対応するその他のサービスは、性別、年齢、カースト、肌の 色、都市と農村の違い、社会階級に関係なく、すべての人に平等に提供されなければならない。 地域社会の参加 - 地域、国、その他の利用可能な資源を最大限に活用するため。地域社会への参加は、国際的な開発援助に依存した的を絞った(あるいは垂直的な)アプローチと は対照的に、草の根的な性質と自給自足を重視することから、持続可能であると考えられていた[5]。 保健医療人材の育成 - 包括的な保健医療は、訓練を受けた医師、看護師、保健医療専門職、コミュニティ・ヘルス・ワーカー、その他が適切な数と配分を受け、保健チームとして活動 し、地域レベルや紹介レベルで支援されることに依存する。 適切な技術の使用-医療技術は、アクセスしやすく、手ごろな価格で、実現可能で、地域社会に文化的に受け入れられるものを提供すべきである。適切な技術の 例としては、冷たいワクチンを保管するための冷蔵庫などがある。適切でない医療技術の例としては、多くの場 合、ボディスキャナーや人工心肺装置などが考えられるが、 これらは都市部に集中する少数派にしか恩恵がない。これらは一般に、貧しい人々には利用できないが、多くの資源を引き出 している[5]。 多部門アプローチ - 公式の保健分野だけの介入では健康は改善され ないという認識である。これらのセクターには、少なくとも、農業(食料安全保障など)、教育、コミュニケーション(一般的な健康問題やその予防・管理方法 など)、住宅、公共事業(安全な水の十分な供給や基本的な衛生設備の確保など)、農村開発、産業、コミュニティ組織(パンチャーヤットや地方自治体、ボラ ンティア組織など)が含まれる。 まとめると、PHCは、ヘルスケアは短期的な介入ではなく、人々の生活を改善し、不健康の原因となる社会経済的状況を緩和する継続的なプロセスであること を認識している。この原則は、健康と開発とを結びつけ、経済状況を受動的に受け入れるのではなく、政治的介入を提唱するものである[5]。 |
Approaches The hospital ship USNS Mercy (T-AH-19) in Manado, Indonesia, during Pacific Partnership 2012. The primary health care approach has seen significant gains in health where applied even when adverse economic and political conditions prevail.[11] The Alma-Ata declaration proposed PHC (Primary Health Care) goals but faced global criticism for being vague, costly, and unattainable. This led to diverse PHC approaches, including SPHC (Selective Primary Health Care), accommodating resource disparities and local health priorities Selective Primary Health Care After the year 1978 Alma Ata Conference, the Rockefeller Foundation held a conference in 1979 at its Bellagio conference center in Italy to address several concerns. Here, the idea of Selective Primary Health Care was introduced as a strategy to complement comprehensive PHC. It was based on a paper by Julia Walsh and Kenneth S. Warren entitled "Selective Primary Health Care, an Interim Strategy for Disease Control in Developing Countries".[12] This new framework advocated a more economically feasible approach to PHC by only targeting specific areas of health and choosing the most effective treatment plan in terms of cost and effectiveness. One of the foremost examples of SPHC is "GOBI" (growth monitoring, oral rehydration, breastfeeding, and immunization),[5] focusing on combating the main diseases in developing nations. GOBI and GOBI-FFF GOBI is a strategy of World Health Organization consisting of (and an acronym for) four low-cost, high impact, knowledge mediated measures introduced as key to halving child mortality by James P. Grant at UNICEF in 1983. The measures are: Growth monitoring: the monitoring of how much infants grow within a period, with the goal to understand needs for better early nutrition.[5] Oral rehydration therapy: to combat dehydration associated with diarrhea. Breastfeeding Immunization Three additional measures were introduced to the strategy later (though food supplementation had been used by UNICEF since its inception in 1946), leading to the acronym GOBI-FFF. Family planning (birth spacing) Female education Food supplementation: for example, iron and folic acid fortification/supplementation to prevent deficiencies in pregnant women. These strategies focus on severe population health problems in certain developing countries, where a few diseases are responsible for high rates of infant and child mortality. Health care planning is used to see which diseases require most attention and, subsequently, which intervention can be most effectively applied as part of primary care in a least-cost method. The targets and effects of selective PHC are specific and measurable.[vague] The approach aims to prevent most health and nutrition problems before they begin:[13][14] PHC and population aging Given global demographic trends, with the numbers of people age 60 and over expected to double by 2025, PHC approaches have taken into account the need for countries to address the consequences of population ageing. In particular, in the future the majority of older people will be living in developing countries that are often the least prepared to confront the challenges of rapidly ageing societies, including high risk of having at least one chronic non-communicable disease, such as diabetes and osteoporosis[15] and conditions like hearing loss.[16]According to WHO, dealing with this increasing burden requires health promotion and disease prevention intervention at the community level as well as disease management strategies within health care systems. PHC and mental health Some jurisdictions apply PHC principles in planning and managing their healthcare services for the detection, diagnosis and treatment of common mental health conditions at local clinics, and organizing the referral of more complicated mental health problems to more appropriate levels of mental health care.[17] The Ministerial Conference, which took place in Alma Ata, made the decision that measures should be taken to support mental health in regard to primary health care. However, there was no such documentation of this event in the Alma Ata Declaration. These discrepancies caused an inability for proper funding and although was worthy of being a part of the declaration, changing it would call for another conference. Individuals with severe mental health disorders are found to live much shorter lives than those without, anywhere from ten to twenty-five-year reduction in life expectancy when compared to those without.[18] Cardiovascular diseases in particular are one of the leading causes of death with individuals already suffering from severe mental health disorders. General health services such as PHC is one approach to integrating an improved access to such health services that could help treat already existing mental health disorders as well as prevent other disorders that could arise simultaneously as the pre-existing condition. PHC and hearing health Considering that 360 million people across the world live with disabling hearing loss, including 32 million children and nearly 180 million older adults, and that chronic ear diseases, such as chronic suppurative otitis media, can lead to hearing loss and may cause life-threatening complications, the seventieth World Health Assembly on May 31 2017 signed the resolution WHA70.13 (Agenda item 15.8) urging member states to integrate strategies for ear and hearing care within the framework of their primary health care systems, under the umbrella of universal health coverage.[1] A World Report on Hearing (WRH) was published in response to the resolution (WHA70.13), to provide guidance for Member States to integrate ear and hearing care into their national health plans.[19] |
アプローチ パシフィック・パートナーシップ2012の期間中、インドネシアのマナドに停泊中の病院船USNSマーシー(T-AH-19)。 プライマリ・ヘルスケア・アプローチは、経済的・政治的に不利な状況が続いている場合でも、適用されれば保健において大きな成果を上げてきた[11]。ア ルマ・アタ宣言は、PHC(プライマリ・ヘルスケア)の目標を提案したが、漠然としており、コストがかかり、達成不可能であるという世界的な批判に直面し た。このため、資源格差や地域の保健上の優先事項に対応するSPHC(選択的プライマリ・ヘルスケア)など、多様なPHCアプローチが生まれた。 選択的プライマリー・ヘルスケア 1978年のアルマ・アタ会議の後、ロックフェラー財団は1979年にイタリアのベラージオ会議センターで会議を開き、いくつかの懸念に対処した。ここ で、包括的PHCを補完する戦略として、選択的プライマリ・ヘルスケア(Selective Primary Health Care)という考え方が紹介された。これは、ジュリア・ウォルシュとケネス・S・ウォーレンによる論文「選択的プライマリ・ヘルスケア、発展途上国にお ける疾病コントロールのための暫定的戦略」[12]に基づくものであった。この新しい枠組みは、特定の健康分野のみを対象とし、費用と効果の観点から最も 効果的な治療計画を選択することで、より経済的に実現可能なPHCへのアプローチを提唱するものであった。SPHCの最も代表的な例のひとつが 「GOBI」(発育モニタリング、経口補水、母乳育児、予防接種)であり[5]、開発途上国における主要な疾病との闘いに焦点を当てている。 GOBIとGOBI-FFF GOBIは、世界保健機関の戦略であり、1983年にユニセフのジェームス・P・グラントが子どもの死亡率を半減させる鍵として紹介した、低コストでイン パクトが高く、知識を媒介とする4つの対策からなる(その頭文字をとったものである)。その対策とは 成長モニタリング:乳幼児が一定期間内にどれだけ成長したかをモニタリングし、早期栄養改善の必要性を把握することを目的とする[5]。 経口補水療法:下痢に伴う脱水と闘う。 母乳育児 予防接種 この戦略には、後に3つの追加措置が導入され(ただし、ユニセフでは1946年の設立当初から食糧補給が行われていた)、頭文字をとってGOBI-FFF と呼ばれるようになった。 家族計画(出産間隔) 女性教育 食品補給:例えば、妊婦の欠乏症予防のための鉄と葉酸の強化/補給。 これらの戦略は、特定の発展途上国における深刻な人口保健問題に焦点を当てたもので、そこでは少数の疾病が乳幼児死亡率の高さの原因となっている。保健医 療計画は、どの疾病に最も注意を払う必要があるか、そしてその後、プライマリ・ケアの一環として、最もコストのかからない方法で、どの介入を最も効果的に 適用できるかを確認するために用いられる。選択的PHCの目標と効果は、具体的で測定可能である[vague]。このアプローチは、健康と栄養の問題のほ とんどを、その問題が始まる前に予防することを目的としている[13][14]。 PHCと高齢化 2025年までに60歳以上の人口が倍増すると予想される世界的な人口統計学的傾向を考慮すると、PHCのアプローチは、各国が人口高齢化の結果に対処す る必要性を考慮している。特に将来、高齢者の大多数は、糖尿病や骨粗鬆症[15]、難聴[16]などの慢性非伝染性疾患を少なくとも1つは抱えるリスクが 高いなど、急速に高齢化する社会の課題に立ち向かう準備が最も遅れている発展途上国に住むことになる。WHOによれば、このような負担の増加に対処するに は、医療システム内での疾病管理戦略だけでなく、コミュニティレベルでの健康増進や疾病予防の介入が必要である。 PHCとメンタルヘルス いくつかの管轄区域では、地域の診療所における一般的な精神衛生状態の発見、診断、治療のためのヘルスケアサービスの計画と管理においてPHCの原則を適 用し、より複雑な精神衛生問題をより適切なレベルの精神衛生ケアに紹介することを組織している[17]。 アルマアタで開催された閣僚会議では、プライマリーヘルスケアに関して精神衛生を支援するための対策を講じるべきであるという決定がなされた。しかし、ア ルマ・アタ宣言には、この出来事に関するそのような文書はなかった。これらの食い違いは、適切な資金援助ができない原因となっており、宣言の一部とする価 値はあったが、それを変更することは、別の会議を必要とするだろう。 重度の精神障害を持つ人は、そうでない人に比べてはるかに短命であり、そうでない人と比較した場合、平均余命は10年から25年短縮することが分かってい る[18]。特に心血管疾患は、すでに重度の精神障害を患っている人の主な死因のひとつである。PHCのような一般的な保健サービスは、すでに存在する精 神疾患の治療だけでなく、既存の状態として同時に発生する可能性のある他の疾患の予防にも役立つ可能性のある、そのような保健サービスへのアクセス改善を 統合するための1つのアプローチである。 PHCと聴覚の健康 3,200万人の子どもや約1億8,000万人の高齢者を含む、世界中で3億6,000万人が障害を伴う難聴を抱え、慢性化膿性中耳炎などの慢性的な耳の 病気が難聴につながり、生命を脅かす合併症を引き起こす可能性があることを考慮し、第70回世界保健総会は2017年5月31日、決議WHA70.13 (議題15. 8)に署名し、加盟国に対し、ユニバーサル・ヘルス・カバレッジの傘の下、プライマリ・ヘルスケア制度の枠組みの中で耳と聴覚のケアの戦略を統合するよう 促した[1]。 この決議(WHA70.13)を受けて、加盟国が耳と聴覚のケアを国の保健計画に統合するための指針を示す「聴覚に関する世界報告(WRH)」が発表され た[19]。 |
| Background and controversies Barefoot Doctors The "Barefoot Doctors" of China were an important inspiration for PHC because they illustrated the effectiveness of having a healthcare professional at the community level with community ties. Barefoot Doctors were a diverse array of village health workers who lived in rural areas and received basic healthcare training. They stressed rural rather than urban healthcare, and preventive rather than curative services. They also provided a combination of western and traditional medicines. The Barefoot Doctors had close community ties, were relatively low-cost, and perhaps most importantly they encouraged self-reliance through advocating prevention and hygiene practices.[5] The program experienced a massive expansion of rural medical services in China, with the number of Barefoot Doctors increasing dramatically between the early 1960s and the Cultural Revolution (1964-1976). Criticisms Although many countries were keen on the idea of primary healthcare after the Alma Ata conference, the Declaration itself was criticized for being too “idealistic” and “having an unrealistic time table”.[5] More specific approaches to prevent and control diseases - based on evidence of prevalence, morbidity, mortality and feasibility of control (cost-effectiveness) - were subsequently proposed. The best known model was the Selective PHC approach (described above). Selective PHC favoured short-term goals and targeted health investment, but it did not address the social causes of disease. As such, the SPHC approach has been criticized as not following Alma Ata's core principle of everyone's entitlement to healthcare and health system development.[5] In Africa, the PHC system has been extended into isolated rural areas through construction of health posts and centers that offer basic maternal-child health, immunization, nutrition, first aid, and referral services.[20] Implementation of PHC is said to be affected after the introduction of structural adjustment programs by the World Bank.[20] |
背景と論争 はだしの医者 中国の "はだしの医者 "は、PHCにとって重要なインスピレーションの源であった。はだしの医者」は、農村に住み、基本的な医療訓練を受けた多様な村の保健ワーカーであった。 彼らは都市部よりも農村部での医療を重視し、治療的サービスよりも予防的サービスを重視した。また、西洋薬と伝統薬を組み合わせて提供した。はだしの医者 たちは、地域社会と密接なつながりを持ち、比較的低費用で、おそらく最も重要なことは、予防と衛生の実践を提唱することで自立を促したことである[5]。 このプログラムは、中国の農村医療サービスの大規模な拡大をもたらし、はだしの医者たちの数は、1960 年代初頭から文化大革命(1964-1976 年)にかけて劇的に増加した。 批判 アルマ・アタ会議後、多くの国々がプライマリ・ヘルスケアの考えに熱心であったが、宣言そのものは「理想主義的」で「非現実的なタイムテーブルを持ってい る」という批判を受けた[5]。その後、有病率、罹患率、死亡率、管理可能性(費用対効果)のエビデンスに基づく、疾病の予防と管理のより具体的なアプ ローチが提案された。最もよく知られたモデルは、選択的PHCアプローチ(前述)である。選択的PHCは、短期的な目標と的を絞った保健投資を優先した が、疾病の社会的原因には対処しなかった。そのため、SPHCアプローチは、アルマ・アタの基本原則である、すべての人が保健医療を受ける権利と保健シス テム開発に則っていないとして批判されてきた[5]。 アフリカでは、PHCシステムは、基本的な母子保健、予防接種、栄養、応急処置、紹介サービスを提供するヘルスポストやセンターの建設を通じて、孤立した 農村地域にまで拡大されている[20]。PHCの実施は、世界銀行による構造調整プログラムの導入後に影響を受けたと言われている[20]。 |
| https://en.wikipedia.org/wiki/Primary_health_care |
|
| Addiction
and substance use disorders, Citation again. Throughout history, addiction has largely been seen as a moral failing or character flaw, as opposed to an issue of public health.[56][57][58] Substance use has been found to be more stigmatized than smoking, obesity, and mental illness.[56][59][60][61] Research has shown stigma to be a barrier to treatment-seeking behaviors among individuals with addiction, creating a "treatment gap".[62][63][64] A systematic review of all epidemiological studies on treatment rates of people with alcohol use disorders found that over 80% had not accessed any treatment for their disorder.[65] The study also found that the treatment gap was larger in low and lower-middle-income countries. Research shows that the words used to talk about addiction can contribute to stigmatization, and that the commonly used terms of "abuse" & "abuser" actually increase stigma.[66][67][68][69] Behavioral addictions (i.e. gambling, sex, etc.) are found to be more likely to be attributed to character flaws than substance-use addictions.[70] Stigma is reduced when Substance Use Disorders are portrayed as treatable conditions.[71][72] Acceptance and Commitment Therapy has been used effectively to help people to reduce shame associated with cultural stigma around substance use treatment.[73][74][75] The use of the drug methamphetamine has been strongly stigmatized. An Australian national population study have shown that the proportion of Australians who nominated methamphetamine as a "drug problem" increased between 2001–2019.[76] The epidemiological study provided evidence that levels of under-reporting have increased over the period, which coincided with the deployment of public health campaigns on the dangers of ice that had stigmatizing elements that portrayal of persons who used the drugs in a negative way.[76] The level of under-reporting of methamphetamine use is strongly associated with increasing negative attitudes towards their use over the same period.[76] https://en.wikipedia.org/wiki/Social_stigma |
依
存症と薬物使用障害(再掲) 歴史を通じて、依存症は公衆衛生の問題とは対照的に、道徳的な失敗や性 格的欠陥と見なされてきた。[56][57][58] 薬物使用は、喫煙、肥満、精神疾患よりもスティグマ化されていることが判明している。 [62][63][64] アルコール使用障害者の治療率に関するすべての疫学研究の系統的レビューによると、80%以上が自分の障害の治療を一切受けていないことがわかった [65]。 この研究はまた、低・中所得国で治療格差がより大きいことも明らかにした。 研究によると、依存症について話す際に使用される言葉がスティグマ化の 一因となる可能性があり、「乱用」「乱用者」という一般的に使用される用語は、実際にスティグマを増大させる[66][67][68][69]。行動依存 症(ギャンブル、セックスなど)は、物質使用依存症よりも性格的欠陥に起因する可能性が高いことがわかっている。 [70] 薬物使用障害が治療可能な状態として描かれることで、スティグマは軽減される。 [71][72] 受容とコミットメント療法は、薬物使用治療をめぐる文化的スティグマに関連する羞恥心を軽減するために効果的に用いられている。 メタンフェタミンという薬物の使用は強くスティグマ化されている。オー ストラリアの全国人口調査によると、覚せい剤を「薬物問題」として指名するオーストラリア人の割合が2001年から2019年の間に増加した[76]。こ の疫学調査では、過少申告のレベルがこの期間に増加したという証拠が示されており、これは、薬物を使用する人を否定的に描くスティグマ的要素を持つ氷の危 険性に関する公衆衛生キャンペーンが展開された時期と一致している[76]。覚せい剤使用の過少申告のレベルは、同じ期間にその使用に対する否定的な態度 が増加したことと強く関連している[76]。 |
What Is Low-Threshold Care and How Does It Work for Addiction Treatment?
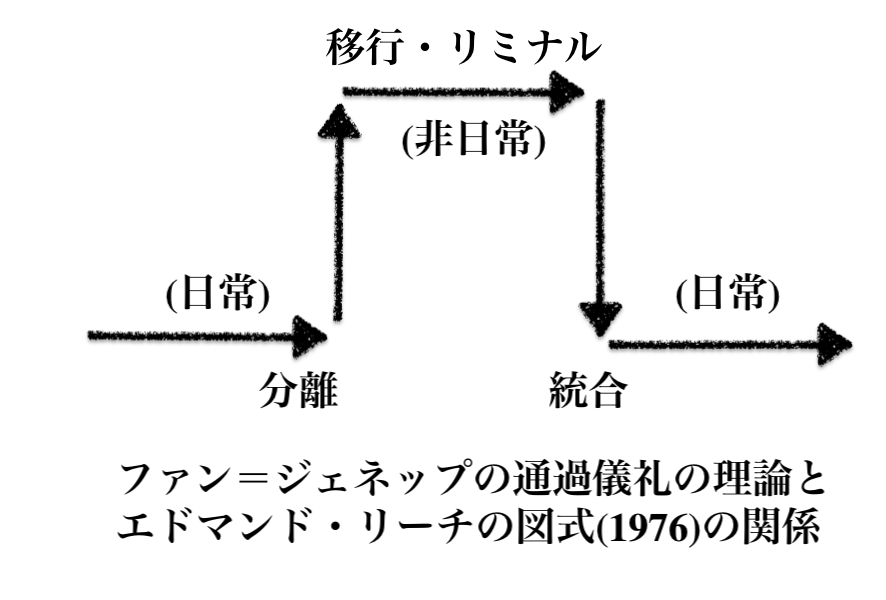
+++
Links
リンク
文献
その他の情報


cc
Copyleft,
CC, Mitzub'ixi Quq Chi'j, 1996-2099