
健康と病気の社会学
Sociology of health and illness
☆
健康と病気の社会学、健康とウェルネスの社会学、または健康社会学は、社会と健康の相互関係を研究する。この学問分野は、健康と幸福に影響を与え、変化を
もたらす現代および歴史的な影響を含む生活のあらゆる側面に関心を持っている。
誕生から死に至るまで、社会的なプロセスが健康と幸福に織り込まれ、影響を及ぼしていることを立証する。こうした影響には、生育環境、病気に対する地域社
会の理解や捉え方、あるいはテクノロジーが健康に与える影響などが含まれる。このように、保健とそれに関わる医学は社会的な構築物であり、病気や健康、そ
れらとの相互作用の認識の仕方は社会的に解釈されるものであると概説している。
保健社会学では、この洞察を基に、人体を機械的な存在として捉える長年にわたって定着してきた考え方を批判し、心と体を別個の空間として扱うという考え方
を覆そうとしている。この生物医学モデルは、健康と幸福が奪われたり、維持されたり、改善されたりする過程において大きな役割を果たす、より広範な社会
的、文化的、経済的、政治的、環境的文脈の中に人間を全体的に位置づけるものではないと見なされている。代替モデルには、心理的な側面とともにこれらの要
素を統合することを目的とする生物心理社会モデル(biopsychosocial model)[5][6]がある。
この研究分野は、保健と健康の生涯にわたる過程に焦点を当てた独自の洞察を提供していることから、医学社会学、身体社会学、疾病社会学[7]といった分野
と重なる幅広い学派として、また家族社会学や教育社会学といったより幅広い社会学とも重なる学派として機能している(→「社会学」「医療社会学」)。
| The sociology of
health and illness, sociology of health and wellness, or health
sociology examines the interaction between society and health. As a
field of study it is interested in all aspects of life, including
contemporary as well as historical influences, that impact and alter
health and wellbeing.[1][2] It establishes that, from birth to death, social processes interweave and influence health and wellbeing. These influences may include location of upbringing, how illness is understood and framed by immediate community members, or the impact that technology has on health. As such, it outlines that both health and the medical science that engages it are social constructs; that the way of knowing illness, wellbeing, and interactions with them are socially interpreted.[3][4] Health sociology uses this insight to critique long-established ideas around the human body as a mechanical entity alongside disrupting the idea that the mind and body can be treated as distinct spaces. This biomedical model is viewed as not holistically placing humans within the wider social, cultural, economic, political, and environmental contexts that play a large part in how health and wellbeing are deprived, maintained, or improved. Alternative models include the biopsychosocial model[5][6] which aims to incorporate these elements alongside the psychological aspect of the mind. This field of research acts as a broad school overlapping with areas like the sociology of medicine, sociology of the body, sociology of disease[7] to wider sociologies like that of the family or education as they contribute insights from their distinct focuses on the life-course of health and wellness.[8] |
健康と病気の社会学、健康とウェルネスの社会学、または健康社会学は、
社会と健康の相互関係を研究する。この学問分野は、健康と幸福に影響を与え、変化をもたらす現代および歴史的な影響を含む生活のあらゆる側面に関心を持っ
ている。 誕生から死に至るまで、社会的なプロセスが健康と幸福に織り込まれ、影響を及ぼしていることを立証する。こうした影響には、生育環境、病気に対する地域社 会の理解や捉え方、あるいはテクノロジーが健康に与える影響などが含まれる。このように、保健とそれに関わる医学は社会的な構築物であり、病気や健康、そ れらとの相互作用の認識の仕方は社会的に解釈されるものであると概説している。 保健社会学では、この洞察を基に、人体を機械的な存在として捉える長年にわたって定着してきた考え方を批判し、心と体を別個の空間として扱うという考え方 を覆そうとしている。この生物医学モデルは、健康と幸福が奪われたり、維持されたり、改善されたりする過程において大きな役割を果たす、より広範な社会 的、文化的、経済的、政治的、環境的文脈の中に人間を全体的に位置づけるものではないと見なされている。代替モデルには、心理的な側面とともにこれらの要 素を統合することを目的とする生物心理社会モデル(biopsychosocial model)[5][6]がある。 この研究分野は、保健と健康の生涯にわたる過程に焦点を当てた独自の洞察を提供していることから、医学社会学、身体社会学、疾病社会学[7]といった分野 と重なる幅広い学派として、また家族社会学や教育社会学といったより幅広い社会学とも重なる学派として機能している。[8] |
| Nursing
student graduate (center) participates in the reading of the
International Nurses' Pledge during Germanna Community College's
Nursing and Health Technologies convocation, held at the Fredericksburg
Expo and Conference Center in Fredericksburg, Virginia, USA. |
バージニア州フレデリックスバーグのフレデリックスバーグ・エキスポ・アンド・カンファレンス・センターで開催されたジャーマンナ・コミュニティ・カレッジの看護・保健技術学位授与式で、看護学生の卒業生(中央)が国際看護師誓約書の朗読に参加した。 |
| Theoretical perspectives The field of sociology of health and illness has been shaped by the perspectives and contributing works of various authors that have enabled its development. Many research studies touch on the relationship between the patient and doctor as well as their environment within the healthcare system. One of the founders of the sociology of health and illness is Talcott Parsons, an American sociologist, who analyzed the relationship between patients and their doctors in his book The Social System written in 1951. In his sick role theory,[9] he argued that people who were sick adopted a social role, not just a biological condition. Those who were sick deviated from social roles were unable to fulfill their respective functions, thus if too many people claimed to be ill, this would create a dysfunctional society that needed regulating. Creating this mechanism would prevent people who were pretending to be sick to form a subculture of being sick. By developing the “sick role mechanism” patients and doctors had to abide by a set of “rights” and “obligations” that would monitor entry into the sick role. The “rights” of a patient constituted an exemption from performing their respective social roles, such as going to work or housekeeping with the further exemption being given to those severely ill. These rights were given if they maintained two obligations, the first being that they had to view being sick as undesirable and thus must find a way to get better. Second, after a while of being sick, the person must seek the help of a doctor and follow their advice in other to alleviate their illness. The “obligations” of the doctors were to be trained in their field, be motivated to help the patient, have objective and emotional detachment from the patient, and be bound by the rules of professional conduct. Their “rights” consisted of being able to examine the patient physically and ask about their personal life, and have a position of authority and autonomy in their professional practice. Lastly, receive status and reward from their important role in society. Parson’s perspective. In addition, Michel Foucault[10] published The Birth of the Clinic in 1963, in which he developed his theory of the “medical gaze[11]” referring to how doctors filter patient information into a biomedical paradigm, which focuses solely on biological factors excluding how social, environmental and psychological factors can influence a patient’s condition. According to Foucault doctors are trained to be doctor-oriented rather than patient-oriented, which creates a form of abusive power structure. Among these authors have contributed to the development of the field of health and illness by bringing in their perspectives at the time. |
理論的視点 保健と病の社会学の分野は、その発展を可能にしたさまざまな著者の視点や貢献的な著作によって形作られてきた。多くの研究は、患者と医師の関係、および医 療制度内の環境に触れている。保健と疾病の社会学の創始者の一人であるタルコット・パ-ソンズは、1951年に著した『社会システム』の中で、患者と医師 の関係を分析した。彼の病気役割理論では、[9] 病気の人々は生物学的状態だけでなく社会的役割も担っていると主張した。病気の人は社会的役割から逸脱し、それぞれの機能を果たせなくなる。そのため、あ まりにも多くの人が病気であると主張すれば、それは機能不全に陥った社会を生み出し、規制が必要となる。このメカニズムを構築することで、病気のふりをす る人々が病気のサブカルチャーを形成することを防ぐことができる。「病気の役割メカニズム」を発展させることで、患者と医師は「権利」と「義務」のセット に従う必要が生じ、それによって病気の役割への参入が監視されることになる。患者の「権利」とは、それぞれの社会的役割、例えば仕事や家事などから免除さ れることであり、重病の場合はさらに免除される。これらの権利は、2つの義務を維持している場合に与えられる。1つ目は、病気を望ましくないものと見な し、回復する方法を見つけなければならないということである。2つ目は、病気を患ってしばらくすると、その人格は医師の助けを求め、病状を緩和するために 医師の助言に従わなければならないということである。医師の「義務」は、その分野の訓練を受け、患者を助けようという意欲を持ち、患者に対して客観的かつ 感情的に距離を置き、職業上の行動規範に従うことである。医師の「権利」は、患者の身体を診察し、私生活について尋ねることができ、職業上の実践において 権威と自主性を持つ立場にあることである。最後に、社会における重要な役割から地位と報酬を得る。パーソンズの視点。さらに、ミシェル・フーコー (Michel Foucault)[10]は1963年に『臨床の誕生』を出版し、医師が患者の情報を生物医学的パラダイムにフィルタリングする方法について言及した 「医療のまなざし(medical gaze)[11]」の理論を展開した。このパラダイムは、患者の状態に影響を与える可能性のある社会的、環境的、心理的要因を除外し、生物学的要因のみ に焦点を当てている。フーコーによれば、医師は患者よりも医師を重視するように訓練されており、これは一種の権力乱用構造を生み出す。これらの著者のうち 何人かは、その時代における彼らの視点を持ち込むことで、保健と病気の分野の発展に貢献した。 |
Historical background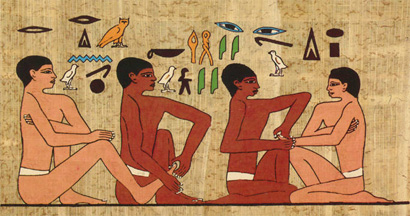 Wall painting found in the tomb of an Egyptian official known as the physicians tomb Humans have long sought advice from those with knowledge or skill in healing. Paleopathology and other historical records, allow an examination of how ancient societies dealt with illness and outbreak. Rulers in Ancient Egypt sponsored physicians that were specialists in specific diseases.[12] Imhotep was the first medical doctor known by name. An Egyptian who lived around 2650 B.C., he was an adviser to King Zoser at a time when Egyptians were making progress in medicine. Among his contributions to medicine was a textbook on the treatment of wounds, broken bones, and even tumors.[13] Stopping the spread of infectious disease was of utmost importance for maintaining a healthy society.[12] The outbreak of disease during the Peloponnesian War was recorded by Thucydides who survived the epidemic. From his account it is shown how factors outside the disease itself can affect society. The Athenians were under siege and concentrated within the city. Major city centers were the hardest hit.[14] This made the outbreak even more deadly and with probable food shortages the fate of Athens was inevitable.[14] Approximately 25% of the population died of the disease.[14] Thucydides stated that the epidemic "carried away all alike". The disease attacked people of different ages, sexes and nationalities.[14]  Physician in Ancient Greece treating a patient 480–470 BC Ancient medical systems stressed the importance of reducing illness through divination and ritual.[12] Other codes of behavior and dietary protocols were widespread in the ancient world.[12] During the Zhou dynasty in China, doctors suggested exercise, meditation and temperance to preserve one's health.[12] The Chinese closely link health with spiritual well-being. Health regimes in ancient India focused on oral health as the best method for a healthy life.[12] The Talmudic code created rules for health which stressed ritual cleanliness, connected disease with certain animals and created diets.[12] Other examples include the Mosaic Code and Roman baths and aqueducts.[12] Those that were most concerned with health, sanitation and illness in the ancient world were those in the elite class.[12] Good health was thought to reduce the risk of spiritual defilement and therefore enhanced the social status of the ruling class who saw themselves as the beacon of civilization.[12] During the late Roman Period, sanitation for the lower classes was a concern for the leisured class.[12] Those that had the means would donate to charities that focused on the health of non-elites.[12] After the decline of the Roman Empire, physicians and concern with public health disappeared except in the largest cities.[12] Health and public doctors remained in the Byzantine Empire.[12] Focusing on preventing the spread of diseases such as small pox lead to a smaller mortality rate in much of the western world.[12] Other factors that allowed the modern rise in population include: better nutrition and environmental reforms (such as getting clean water supplies).[12] The present day sense of health being a public concern for the state began in the Middle Ages.[15] A few state interventions include maintaining clean towns, enforcing quarantines during epidemics and supervising sewer systems.[15] Private corporations also played a role in public health. The funding for research and the institutions for them to work were funded by governments and private firms.[15] Epidemics were the cause of most government interventions. The early goal of public health was reactionary whereas the modern goal is to prevent disease before it becomes a problem.[15] Despite the overall improvement of world health, there still has not been any decrease in the health gap between the affluent and the impoverished.[16] Today, society is more likely to blame health issues on the individual rather than society as a whole. This was the prevailing view in the late 20th century.[16] In the 1980s the Black Report, published in the United Kingdom, went against this view and argued that the true root of the problem was material deprivation.[16] This report proposed a comprehensive anti-poverty strategy to address these issues.[16] Since this did not parallel the views of the Conservative government, it did not go into action immediately.[16] The Conservative government was criticized by the Labour Party for not implementing the suggestions that the Black Report listed.[16] This criticism gave the Black Report the exposure it needed and its arguments were considered a valid explanation for health inequality.[16] There is also a debate over whether poverty causes ill-health or if ill-health causes poverty.[16] Arguments by the National Health Service gave considerable emphasis to poverty and lack of access to health care. It has also been found that heredity has more of a bearing on health than social environment, but research has also proved that there is indeed a positive correlation between socioeconomic inequalities and illness.[16] |
歴史的背景 医師の墓として知られるエジプト高官の墓から発見された壁画 人間は長い間、治療に関する知識や技術を持つ人々から助言を求めてきた。古病理学やその他の歴史的記録から、古代社会が病気や流行にどのように対処してい たかを検証することができる。古代エジプトの支配者は、特定の疾患の専門家である医師を後援していた。[12] イムホテプは、名前が知られている最初の医師である。紀元前2650年頃に生きたエジプト人である彼は、エジプト人が医学の進歩を遂げつつあった時代に、 ソセラー王の顧問を務めていた。医学への貢献のひとつに、傷や骨折、さらには腫瘍の治療に関する教科書がある。[13] 感染症の蔓延を食い止めることは、健全な社会を維持する上で最も重要であった。[12] ペロポネソス戦争中の伝染病の発生は、その流行を生き延びたトゥキュディデスによって記録されている。彼の記述から、伝染病以外の要因が社会にどのような 影響を与えるかが示されている。アテナイ人は包囲され、都市内に集中していた。主要都市が最も大きな打撃を受けた。[14] これがさらに致命的な流行を引き起こし、食糧不足も予想されたため、アテナイの運命は避けられなかった。[14] 人口のおよそ25%がこの病気で死亡した。[14] トゥキュディデスは、この流行病が「すべての人々を等しく奪っていった」と述べている。この病気は、異なる年齢、性別、国籍の人々を襲った。[14] 古代ギリシャの医師が患者を治療している様子(紀元前480年~470年 古代の医療システムでは、占いや儀式を通じて病気を軽減することの重要性が強調されていた。[12] その他の行動規範や食事療法も古代世界では広く普及していた。[12] 中国の周王朝では、医師は健康維持のために運動、瞑想、節制を勧めていた。[12] 中国では、健康と精神的な幸福は密接に関連している。古代インドの保健制度では、健康的な生活を送るための最善の方法として口腔衛生に重点が置かれてい た。[12] タルムードの規定では、儀式的な清潔さを強調し、特定の動物と病気を関連付け、食事療法を考案するなど、保健のための規則が定められた。[12] その他の例としては、モーセの律法やローマの浴場や水道橋などがある。[12] 古代世界において、保健、衛生、病気について最も関心を寄せていたのはエリート階級の人々であった。[12] 健康であることは精神的な穢れを減らすと考えられており、そのため、文明の灯台であると自負する支配階級の社会的地位を高めることにもなった。 [12] ローマ時代後期には、下層階級の衛生状態は富裕層の関心事であった。[12] 余裕のある人々は、エリート層以外の健康に焦点を当てた慈善団体に寄付をした。[12] ローマ帝国の衰退後、医師や公衆衛生への関心は、最大都市を除いて消滅した。[12] 健康と公衆衛生はビザンチン帝国に残った。 [12] 天然痘などの病気の蔓延防止に重点的に取り組んだことで、西側世界の大部分で死亡率が低下した。[12] その他、人口の近代的な増加を可能にした要因としては、栄養状態の改善や環境改革(清潔な水の供給など)が挙げられる。[12] 保健が国家にとっての公共の関心事であるという感覚は、中世に始まった。[15] いくつかの国家による介入には、清潔な街の維持、流行病発生時の隔離の実施、下水システムの監督などがある。[15] 民間企業も公衆衛生において役割を果たした。研究のための資金や研究機関は、政府や民間企業によって賄われた。[15] 流行病は、ほとんどの政府介入の原因となった。公衆衛生の初期の目標は事後対応であったが、現代の目標は問題となる前に疾病を予防することである。 [15] 世界の保健状態は全体的に改善しているにもかかわらず、富裕層と貧困層の間の保健格差は依然として縮小していない。[16] 今日、社会は保健問題を社会全体よりも個人の責任であると考える傾向が強い。これは20世紀後半の一般的な見解であった。[16] 1980年代に英国で発表されたブラック・レポートは、この見解に反論し、問題の真の根源は物質的剥奪にあると主張した。[16] このレポートは、これらの問題に対処するための包括的な貧困対策戦略を提案した。[16] しかし、これは保守党政府の見解と一致しなかったため、すぐに実行に移されることはなかった。 保守党政府は、ブラック・レポートが挙げた提案を実施しなかったとして労働党から批判された。[16] この批判により、ブラック・レポートは必要な注目を集めることとなり、その主張は保健格差の妥当な説明とみなされるようになった。[16] また、貧困が不健康の原因なのか、それとも不健康が貧困の原因なのかについても議論がある。[16] 英国国民保健サービス(NHS)の主張では、貧困と医療へのアクセスの欠如が特に強調された。また、社会環境よりも遺伝が健康に大きな影響を与えることも 分かっているが、社会経済的不平等と疾病の間には確かに正の相関関係があることも研究で証明されている。[16] |
| cial
environment, but research has also proved that there is indeed a
positive correlation between socioeconomic inequalities and illness.[16] Methodology The Sociology of Health and Illness focuses on three areas: the conceptualization, the study of measurement and social distribution, and the justification of patterns in health and illness. By looking at these things researchers can look at different diseases through a sociological lens. The prevalence and response to different diseases varies by culture.[17] By looking at bad health, researchers can see if health affects different social regulations or controls. When measuring the distribution of health and illness, it is useful to look at official statistics and community surveys. Official statistics make it possible to look at people who have been treated. It shows that they are both willing and able to use health services. It also sheds light on the infected person's view of their illness. On the other hand, community surveys look at people's rating of their health. Then looking at the relation of clinically defined illness and self reports and find that there is often a discrepancy. A great deal of the time, mortality statistics take the place of the morbidity statistics because in many developed societies where people typically die from degenerative conditions, the age in which they die sheds more light on their life-time health. This produces many limitations when looking at the pattern of sickness, but sociologists try to look at various data to analyze the distribution better. Normally, developing societies have lower life expectancies in comparison to developed countries. They have also found correlations between mortality and sex and age. Very young and old people are more susceptible to sickness and death. On average women typically live longer than men, although women are more likely to have bad health.[17] 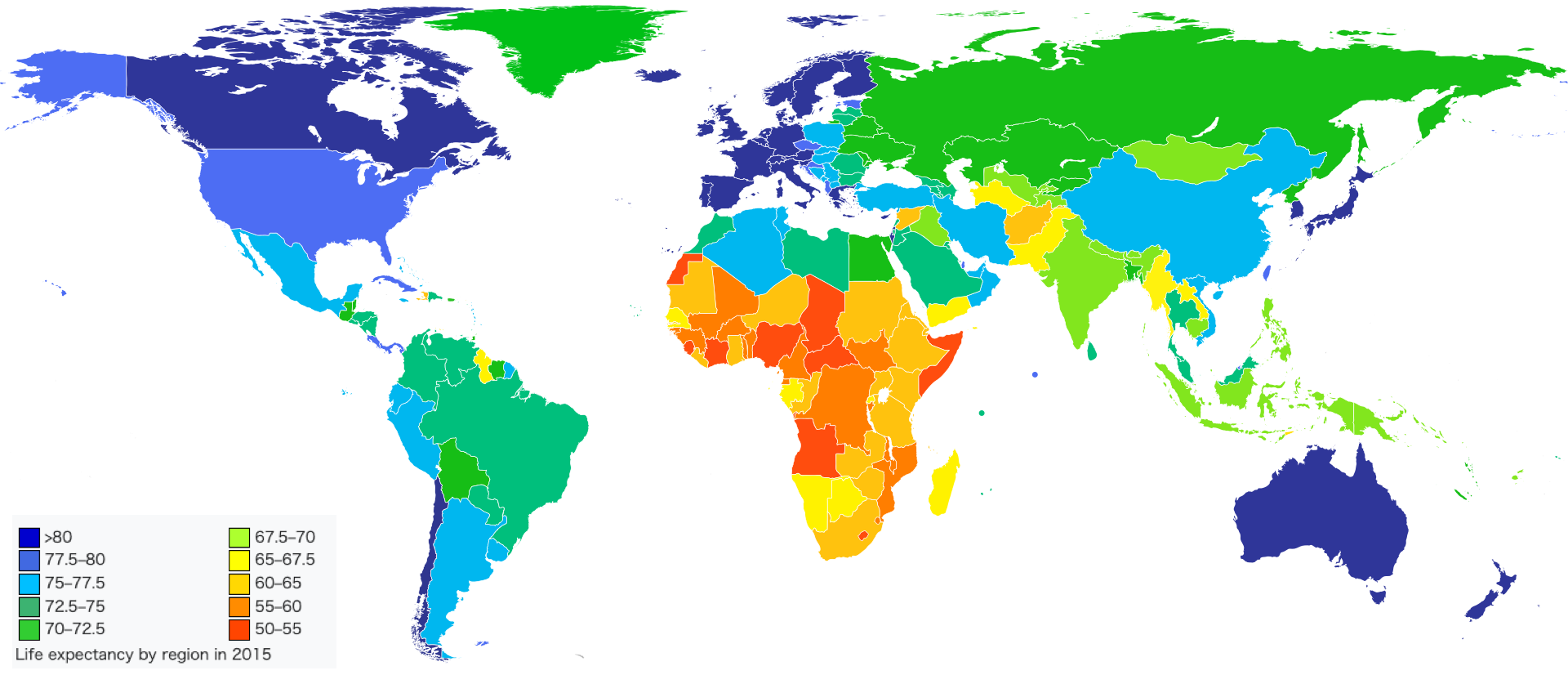 >80 77.5–80 75–77.5 72.5–75 70–72.5 67.5–70 65–67.5 60–65 55–60 50–55 Life expectancy by region in 2015 Disparities in health were also found between people in different social classes and ethnicities within the same society, even though in the medical profession they put more importance in "health related behaviors" such as alcohol consumption, smoking, diet, and exercise. There is a great deal of data supporting the conclusion that these behaviors affect health more significantly than other factors.[17] Sociologists think that it is more helpful to look at health and illness through a broad lens. Sociologists agree that alcohol consumption, smoking, diet, and exercise are important issues, but they also see the importance of analyzing the cultural factors that affect these patterns. Sociologists also look at the effects that the productive process has on health and illness. While also looking at things such as industrial pollution, environmental pollution, accidents at work, and stress-related diseases.[17] Social factors play a significant role in developing health and illness. Studies of epidemiology show that autonomy and control in the workplace are vital factors in the etiology of heart disease. One cause is an effort-reward imbalance. Decreasing career advancement opportunities and major imbalances in control over work have been coupled with various negative health costs. Various studies have shown that pension rights may shed light on mortality differences between retired men and women of different socioeconomic statuses. These studies show that there are outside factors that influence health and illness.[17] |
社会環境も関係しているが、研究により、社会経済格差と疾病には確かに正の相関関係があることが証明されている。[16] 方法論 健康と疾病の社会学は、概念化、測定と社会分布の研究、健康と疾病のパターンの正当化という3つの領域に焦点を当てている。これらの事柄を研究すること で、研究者は社会学的レンズを通して異なる疾病を観察することができる。異なる疾病の発生率や対応は文化によって異なる。[17] 健康状態の悪さを見れば、保健がさまざまな社会的規制や管理に影響を及ぼしているかどうかを研究者は知ることができる。保健と疾病の分布を測定する際に は、公式統計や地域社会調査を参考にすることが有益である。公式統計では、治療を受けたことがある人々を調査することができる。これにより、彼らが保健 サービスを利用する意思と能力の両方を持っていることがわかる。また、感染者の疾病に対する見方も明らかになる。一方、地域社会調査では、人々の健康状態 の評価を調べる。そして、臨床的に定義された疾患と自己申告との関係を調べ、しばしば相違があることが判明する。 多くの先進社会では、人々は通常、退行性疾患で死亡するため、死亡統計が罹患率統計の代わりとなることが多い。なぜなら、死亡した年齢の方が、その人の生 涯の健康状態をより明らかにするからである。このため、疾病のパターンを分析する際に多くの制限が生じるが、社会学者はより良い分布分析を行うために、さ まざまなデータに目を向けようとしている。通常、発展途上社会では、先進国と比較して平均余命が短い。また、死亡率と性別および年齢との相関関係も発見さ れている。非常に若い人々や高齢者は、病気や死亡のリスクが高い。平均すると、女性は男性よりも長生きであるが、女性の方が健康状態が悪い傾向にある。 [17] >80 77.5–80 75–77.5 72.5–75 70–72.5 67.5–70 65–67.5 60–65 55–60 50–55 Life expectancy by region in 2015 医療関係者は、アルコール摂取、喫煙、食事、運動などの「保健関連行動」をより重視しているが、同じ社会の中でも異なる社会階級や民族に属する人々の間で も、保健状態に格差があることが分かっている。これらの行動が他の要因よりも健康に大きな影響を与えるという結論を裏付けるデータは数多く存在する。 [17] 社会学者は、保健と疾病をより広い視点から見る方が有益だと考えている。社会学者は、アルコール摂取、喫煙、食事、運動が重要な問題であることに同意して いるが、これらのパターンに影響を与える文化的要因を分析することの重要性も認識している。社会学者はまた、生産プロセスが保健と疾病に与える影響につい ても調査している。産業公害、環境汚染、労働災害、ストレス関連疾患なども調査対象となっている。 社会的な要因は、保健と疾病の発生において重要な役割を果たしている。疫学の研究では、職場における自主性と統制が心臓疾患の病因において重要な要因であ ることが示されている。その原因の一つは、努力と報酬の不均衡である。キャリアアップの機会の減少と仕事に対する統制の大きな不均衡は、さまざまな健康上 の悪影響と関連している。さまざまな研究により、異なる社会経済的地位にある退職した男女の死亡率の違いを解明する手がかりとして、年金受給権が注目され ている。これらの研究は、保健と疾病に影響を与える外部要因が存在することを示している。[17] |
| International perspective Africa 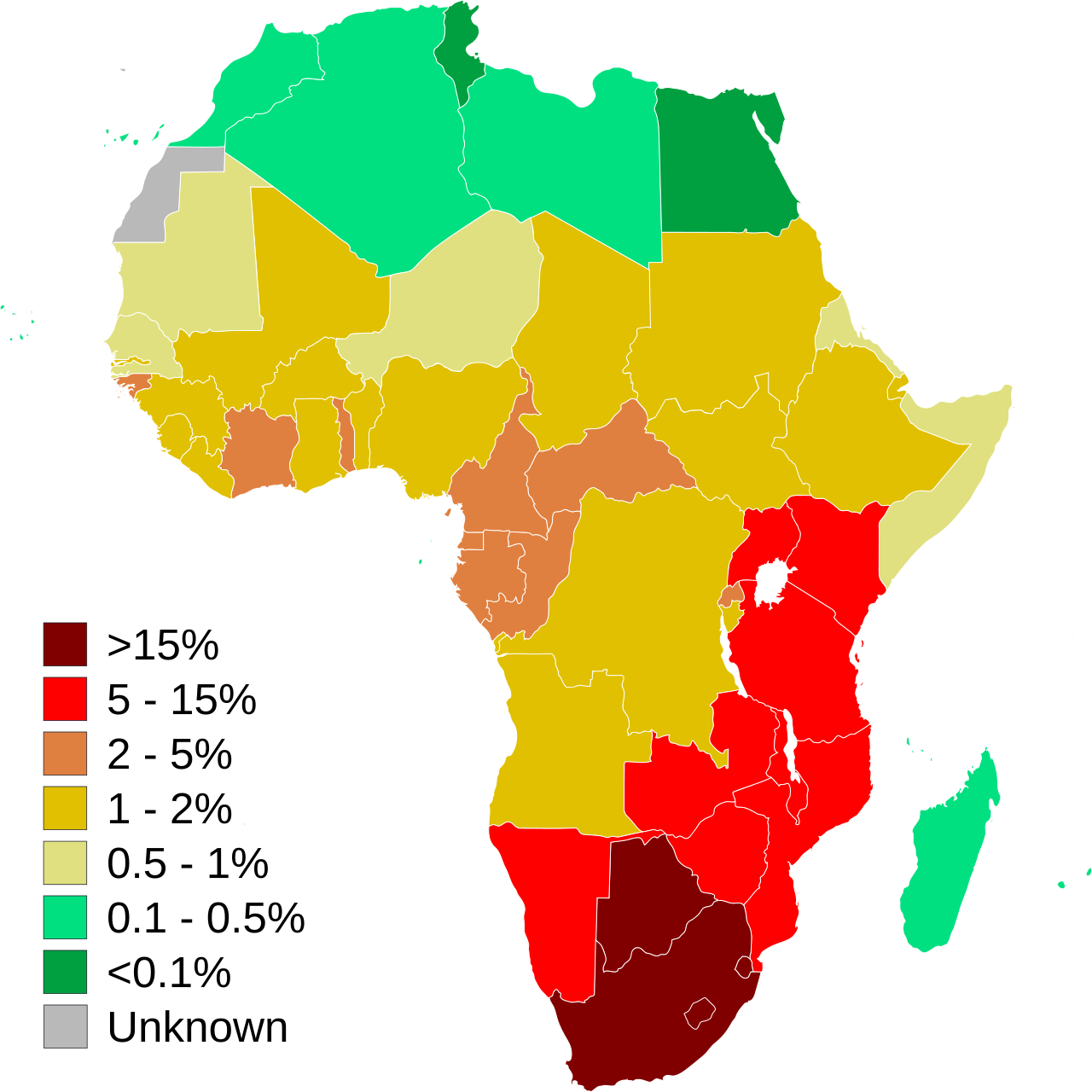 Estimation of the number of adults in Africa who are infected with HIV or AIDS. Note that levels of infection are much higher in sub-Saharan Africa. HIV/AIDS is the leading epidemic that affects the social welfare of Africa.[18] Human Immunodeficiency virus (HIV) can cause AIDS which is an acronym for Acquired Immunodeficiency Syndrome (AIDS), a condition in humans in which the immune system begins to fail, leading to life-threatening infections. Two-thirds of the world's HIV population is located in Sub-Saharan Africa. Since the epidemic started more than 15 million Africans have died by complications with HIV/AIDS.[18] People who are a part of religious sub-groups of Sub-Saharan Africa, and those who actively and frequently participate in religious activities, are more likely to be at a lower risk of contracting HIV/AIDS. On the opposite end, there are many beliefs that an infected male can be cured of the infection by having sex with a virgin. These beliefs increase the number of people with the virus and also increase the number of rapes against women.[19] Herbal treatment is one of the primary medicines used to treat HIV in Africa. It is used more than standard treatment because it is more affordable.[18] Herbal treatment is more affordable but is not researched and is poorly regulated . This lack of research on whether the herbal medicines work and what the medicines consist of is a major flaw in the healing cycle of HIV in Africa.[19] Economically, HIV has a significant negative effect. The labor force in Africa is slowly diminishing, due to HIV-related deaths and illness. In response, government income declines and so does tax revenue. The government has to spend more money than it is making, in order to care for those affected with HIV/AIDS.[18]  AIDS orphans in Malawi A major social problem in Africa in regards to HIV is the orphan epidemic. The orphan epidemic in Africa is a regional problem. In most cases, both of the parents are affected with HIV. Due to this, the children are usually raised by their grandmothers and in extreme cases they are raised by themselves. In order to care for the sick parents, the children have to take on more responsibility by working to produce an income. Not only do the children lose their parents but they also lose their childhood as well. Having to provide care for their parents, the children also miss out on an education which increases the risk of teen pregnancy and people affected with HIV. The most efficient way to diminish the orphan epidemic is prevention: preventing children from acquiring HIV from their mothers at birth, as well as educating them on the disease as they grow older. Also, educating adults about HIV and caring for the infected people adequately will lower the orphan population.[20] The HIV/AIDS epidemic is reducing the average life expectancy of people in Africa by twenty years. The age range with the highest death rates, due to HIV, are those between the ages of 20 and 49 years. The fact that this age range is when adults acquire most of their income means they often cannot afford to send their children to school due to the high medication costs. It also removes the people who could help aid in responding to the epidemic.[18] |
国際的な視点 アフリカ アフリカにおけるHIVまたはAIDSに感染している成人の数。感染率はサハラ以南のアフリカで特に高い。 HIV/AIDSは、アフリカの社会福祉に影響を及ぼす主要な伝染病である。[18] ヒト免疫不全ウイルス(HIV)は、後天性免疫不全症候群(AIDS)の頭文字を取ったエイズ(AIDS)を引き起こす。エイズは、免疫システムが機能し なくなり、生命を脅かす感染症を引き起こす状態である。世界のHIV感染者の3分の2はサハラ以南のアフリカに集中している。この伝染病が蔓延し始めて以 来、1500万人以上のアフリカ人がHIV/AIDSの合併症で死亡している。 サハラ以南のアフリカの宗教的少数派に属する人々や、宗教活動に積極的に頻繁に参加する人々は、HIV/AIDSに感染するリスクが低い傾向にある。一方 で、感染した男性が処女と性交渉を持つことで感染が治癒するという考えも数多く存在する。こうした考えはウイルス保有者の数を増やすとともに、女性に対す るレイプの件数も増加させている。 アフリカでは、HIVの治療に主に用いられている薬の一つに、ハーブ療法がある。これは標準的な治療よりも手頃な価格であるため、より多く使用されてい る。[18] ハーブ療法は手頃な価格であるが、研究は行われておらず、規制も不十分である。ハーブ療法が効果があるのか、またその薬がどのような成分で構成されている のかという研究が行われていないことは、アフリカにおけるHIVの治療サイクルにおける大きな欠陥である。[19] 経済的には、HIVは重大な悪影響を及ぼしている。アフリカでは、HIV関連の死亡や病気により労働人口が徐々に減少している。それに応じて政府収入も減少し、税収も減少している。政府はHIV/AIDS感染者のケアに、収入以上の支出を余儀なくされている。 マラウイのエイズ孤児 HIVに関してアフリカで大きな社会問題となっているのは、孤児の蔓延である。アフリカにおける孤児問題は地域的な問題である。ほとんどの場合、両親がと もにHIVに感染している。そのため、子供たちは通常、祖母に育てられ、極端な場合には自分だけで育つことになる。病気の親の世話をしなければならないた め、子供たちは収入を得るために働くなど、より多くの責任を担わなければならない。子供たちは親を失うだけでなく、子供時代をも失うことになる。親の介護 をしなければならないため、子供たちは教育を受ける機会を失い、その結果、思春期での妊娠やHIV感染のリスクが高まる。孤児の増加を食い止める最も効果 的な方法は、予防である。つまり、子供たちが母親からHIVに感染しないようにすること、そして子供たちが成長する過程で、この病気について教育すること である。また、HIVについて大人たちに教育し、感染者に対して適切なケアを行うことで、孤児の数を減らすことができる。 HIV/エイズの流行により、アフリカの人々の平均余命は20年縮まっている。HIVが原因で死亡する率が最も高い年齢層は、20歳から49歳である。こ の年齢層は、大人が収入の大半を得る時期であるため、高額な薬代を支払う余裕がなく、子供たちを学校に行かせることができないことが多い。また、この流行 への対応を支援できる人材も失われている。[18] |
| Asia Asian countries have wide variations of population, wealth, technology and health care, causing attitudes towards health and illness to differ. Japan, for example, has the third highest life expectancy (82 years old), while Afghanistan has the 11th worst (44 years old).[21] Key issues in Asian health include childbirth and maternal health, HIV and AIDS, mental health, and aging and the elderly. These problems are influenced by the sociological factors of religion or belief systems, attempts to reconcile traditional medicinal practices with modern professionalism, and the economic status of the inhabitants of Asia.  People living with HIV/AIDS Like the rest of the world, Asia is threatened by a possible pandemic of HIV and AIDS. Vietnam is a good example of how society is shaping Asian HIV/AIDS awareness and attitudes towards this disease. Vietnam is a country with feudal, traditional roots, which, due to invasion, wars, technology and travel is becoming increasingly globalized. Globalization has altered traditional viewpoints and values. It is also responsible for the spread of HIV and AIDS in Vietnam. Even early globalization has added to this problem – Chinese influence made Vietnam a Confucian society, in which women are of less importance than men. Men in their superiority have no need to be sexually responsible, and women, generally not well educated, are often unaware of the risk, perpetuating the spread of HIV and AIDS as well as other STIs.[22] Confucianism has had a strong influence on the belief system in Asia for centuries, particularly in China, Japan, and Korea, and its influence can be seen in the way people chose to seek, or not seek, medical care.[citation needed] An important issue in Asia is societal effect on the ability of disabled individuals to adjust to a disability. Cultural beliefs shape attitudes towards physical and mental disabilities. China exemplifies this problem. According to Chinese Confucian tradition (which is also applicable in other countries where Confucianism has been spread), people should always pursue good health in their lives, with an emphasis on health promotion and disease prevention.[23] To the Chinese, having a disability signifies that one has not led a proper lifestyle and therefore there is a lack of opportunities for disabled individuals to explore better ways to accept or adapt to their disability.[23] Indigenous healing practices are extremely diverse throughout Asia but often follow certain patterns and are still prevalent today. Many traditional healing practices include shamanism and herbal medicines, and may have been passed down orally in small groups or even institutionalized and professionalized.[24] In many developing countries the only health care available until a few decades ago were those based on traditional medicine and spiritual healing. Now governments must be careful to create health policies that strike a balance between modernity and tradition. Organizations, like the World Health Organization, try to create policies that respect tradition without trying to replace it with modern science, instead regulating it to ensure safety but keeping it accessible.[25] India in particular tries to make traditional medicines safe but still available to as many people as possible, adapting tradition to match modernization while still considering the economic positions and culture of its citizens.[25]  Flag of World Health Organization Mental health issues are gaining an increasing amount of attention in the Asian countries.[citation needed] Many of these countries have a preoccupation with modernizing and developing their economies, resulting in cultural changes. In order to reconcile modern techniques with traditional practices, social psychologists in India are in the process of "indigenizing psychology". Indigenous psychology is that which is derived from the laws, theories, principals, and ideas of a culture and unique to each society.[23] In many Asian countries, childbirth is still treated by traditional means and is thought of with regional attitudes. For example, in Pakistan, decisions concerning pregnancy and antenatal care (ANC) are usually made by older women, often the pregnant woman's mother-in-law, while the mother and father to be are distanced from the process. They may or may not receive professional ANC depending on their education, class, and financial situation.[26] Generally in Asia, childbirth is still a woman's area and male obstetricians are rare. Female midwives and healers are still the norm in most places. Western methods are overtaking the traditional in an attempt to improve maternal health and increase the number of live births.[27] Asian countries, which are mostly developing nations, are aging rapidly even as they are attempting to build their economies. Even wealthy Asian nations, such as Japan, Singapore, and Taiwan, also have very elderly populations and thus have to try to sustain their economies and society with small younger generations while caring for their elderly citizens.[28] The elderly have been traditionally well respected and well cared for in most Asian cultures; experts predict that younger generations in the future are less likely to be concerned and involved in the health care of their older relatives due to various factors such as women joining the workforce more, the separation of families because of urbanization or migration, and the proliferation of Western ideals such as individualism.[29] |
アジア アジア諸国には、人口、富、技術、医療の面で大きなばらつきがあり、健康や病気に対する考え方も異なる。例えば、日本は世界で3番目に平均寿命が長い国 (82歳)であるが、アフガニスタンは11番目に短い国(44歳)である。[21] アジアの保健における主な問題には、出産と妊産婦の健康、HIVとエイズ、精神衛生、高齢化と高齢者が含まれる。これらの問題は、宗教や信念体系、伝統的 な医療行為と近代的な専門性の調和を図る試み、アジアの住民の経済状況といった社会学的要因の影響を受けている。 HIV/AIDSと共に生きる人々 他の国々と同様に、アジアもHIVとAIDSのパンデミック(世界的大流行)の脅威にさらされている。ベトナムは、アジアにおけるHIV/AIDSに対す る認識と、この病気に対する態度が社会によってどのように形成されていくかを示す好例である。ベトナムは封建的で伝統的なルーツを持つ国であるが、侵略、 戦争、技術、旅行により、次第にグローバル化が進んでいる。グローバル化は、伝統的な視点や価値観を変化させた。また、ベトナムにおけるHIVとエイズの 蔓延にも一因している。初期のグローバル化ですら、この問題に拍車をかけた。中国の影響により、ベトナムは儒教社会となり、女性は男性よりも重要視されな くなった。優位に立つ男性は性的に責任を持つ必要がなく、一般的に教育を受けていない女性はリスクを認識しておらず、HIVとエイズ、およびその他の性感 染症の蔓延を助長している。 儒教は数世紀にわたってアジアの信念体系に強い影響を与えており、特に中国、日本、韓国においてその影響は顕著である。その影響は、人々が医療を受けるか 受けないかを選択する方法にも見られる。[要出典] アジアにおける重要な問題は、障害を持つ個人が障害に適応する能力に対する社会的な影響である。文化的な信念は、身体障害や精神障害に対する態度を形成す る。中国はこの問題の典型例である。中国の儒教の伝統(儒教が普及している他の国々にも当てはまる)では、人々は常に健康増進と疾病予防に重点を置いて、 健康を追求すべきであるとされている。[23] 中国人にとって、障害を持つことは適切な生活習慣を維持できていないことを意味し、そのため障害を持つ人々が障害を受け入れる、あるいは障害に適応するた めのより良い方法を模索する機会が不足している。[23] アジア各地の伝統的な治療法はきわめて多様であるが、一定のパターンに従っている場合も多く、現在でも広く普及している。多くの伝統的な治療法には、 シャーマニズムや薬草療法が含まれ、小集団内で口頭で伝えられてきたものや、制度化され専門化されたものもある。[24] 多くの発展途上国では、ほんの数十年前まで、伝統医療やスピリチュアル・ヒーリングに基づく医療が唯一の医療であった。現在、各国政府は、近代性と伝統の バランスを考慮した保健政策を策定する必要がある。世界保健機関(WHO)などの組織は、伝統を近代科学で置き換えるのではなく、伝統を尊重しながら安全 性を確保し、誰もが利用できるように規制する政策の策定を試みている。[25] 特にインドでは、伝統医学を安全なものにしながらも、できるだけ多くの人々が利用できるようにし、伝統を近代化に適応させつつも、国民の経済状況や文化を 考慮している。[25] 世界保健機関の旗 アジア諸国では、メンタルヘルス問題への関心が高まっている。[要出典] これらの国々の多くは経済の近代化と発展に専念しており、その結果、文化の変化が生じている。 近代的な技術と伝統的な慣習を調和させるため、インドの社会心理学者たちは「心理学の現地化」を進めている。 現地の心理学とは、文化の法則、理論、原則、およびアイデアから派生したもので、各社会に特有のものである。[23] アジアの多くの国々では、出産は今でも伝統的な方法で扱われ、地域特有の考え方で捉えられている。例えば、パキスタンでは、妊娠や妊婦健診(ANC)に関 する決定は通常、年配の女性、多くの場合、妊婦の義理の母親によってなされるが、父親や母親はプロセスから距離を置いている。彼らは、教育、階級、経済状 況によって、専門家の助産ケアを受ける場合も受けない場合もある。[26] 一般的にアジアでは、出産は依然として女性の領域であり、男性産科医はまれである。女性の助産師や治療師が、ほとんどの場所で今でも一般的である。女性の 保健の改善と生存出産数の増加を目指して、西洋の方法が伝統的な方法を追い越そうとしている。[27] アジア諸国は、そのほとんどが発展途上国であり、経済発展を図っている最中にもかかわらず急速に高齢化が進んでいる。日本、シンガポール、台湾などの富裕 なアジア諸国でも高齢化が進んでおり、高齢者のケアをしながら、少ない若い世代で経済と社会を維持していかなければならない状況にある。 [28] ほとんどのアジア文化では、高齢者は伝統的に尊敬され、大切にされてきた。専門家は、女性の労働参加の増加、都市化や移住による家族の離散、個人主義など の西洋的価値観の普及といったさまざまな要因により、将来の若い世代は、高齢の親族の保健ケアにあまり関心を示さず、関与しない可能性が高いと予測してい る。[29] |
| Australia The health patterns found on the continent of Australia which includes the Pacific Islands, have been very much influenced by European colonization. While indigenous medicinal beliefs are not significantly prevalent in Australia, traditional ideas are still influential in the health care problems in many of the islands of the Pacific.[30] The rapid urbanization of Australia led to epidemics of typhoid fever and the Bubonic plague. Because of this, public health was professionalized beginning in the late 1870s in an effort to control these and other diseases. Since then Australia's health system has evolved similarly to Western countries and the main cultural influence affecting health care are the political ideologies of the parties in control of the government.[30] 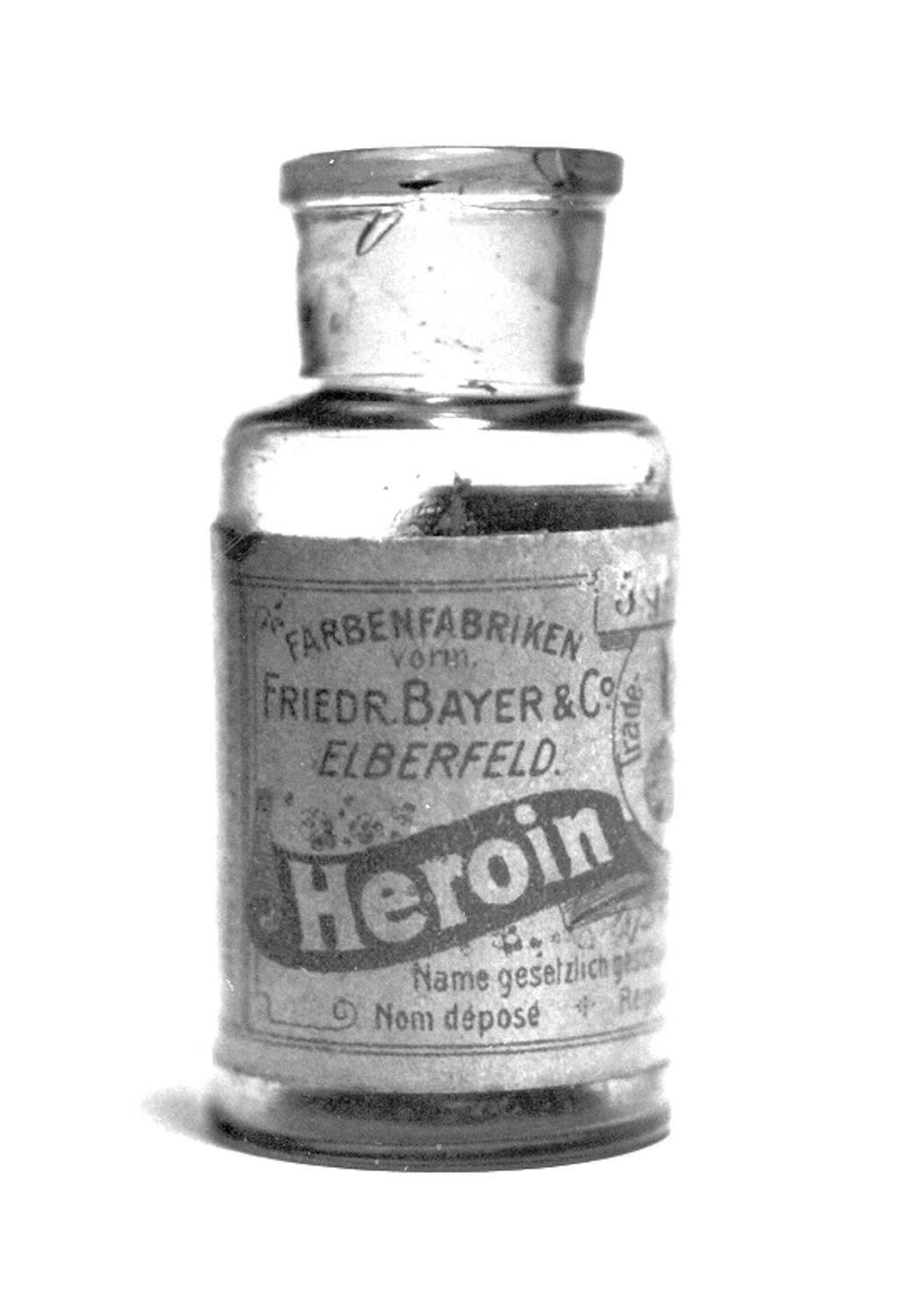 Old heroin bottle Australia has had treatment facilities for 'problem drinkers' since the 1870s. In the 1960s and 1970s it was recognized that Australia had several hundred thousand alcoholics and prevention became a priority over cures, as there was a societal consensus that treatments are generally ineffective.[30] The government began passing laws attempting to curb alcohol consumption but consistently met opposition from the wine-making regions of southern Australia. The government has also waged a war on illegal drugs, particularly heroin, which in the 1950s became widely used as a pain reliever.[30] Experts believe that many of the health problems in the Pacific Islands can be traced back to European colonization and the subsequent globalization and modernization of island communities.[31] (See History of the Pacific Islands.) European colonization and late independence meant modernization but also slow economic growth, which had an enormous effect on health care, particularly on nutrition in the Pacific Islands. The end of colonization meant a loss of medical resources, and the fledgling independent governments could not afford to continue the health policies put in place by the colonial governments.[31] Nutrition was changed radically, contributing to various other health problems. While more prosperous, urban areas could afford food, they chose poor diets, causing 'overnourishment', and leading to extremely high levels of obesity, type 2 diabetes, and cardiovascular diseases. Poorer rural communities, on the other hand, continue to suffer from malnutrition and malaria.[31] Traditional diets in the Pacific are very low in fat, but since World War II there has been a significant increase in fat and protein in Pacific diets. Native attitudes towards weight contribute to the obesity problem. Tongan natives see obesity as a positive thing, especially in men. They also believe that women should do as little physical work as possible while the men provide for them, meaning they get very little exercise.[31] |
オーストラリア 太平洋諸島を含むオーストラリア大陸で見られる保健のパターンは、ヨーロッパの植民地化の影響を強く受けている。オーストラリアでは、先住民の薬草信仰は あまり一般的ではないが、伝統的な考え方は太平洋諸島の多くの島々における保健上の問題に今でも影響を与えている。[30] オーストラリアの急速な都市化は、腸チフスやペストの流行を招いた。このため、1870年代後半から、これらの病気やその他の病気を制御するために公衆衛 生が専門化された。それ以来、オーストラリアの保健システムは欧米諸国と同様に発展し、医療に影響を与える主な文化的要因は、政府を支配する政党の政治的 イデオロギーである。 古いヘロインのビン(バイエル) オーストラリアでは1870年代から「問題飲酒者」のための治療施設が存在していた。1960年代と1970年代には、オーストラリアには数十万人のアル コール依存症患者がいることが認識され、治療よりも予防が優先されるようになった。治療は一般的に効果がないという社会的なコンセンサスがあったためであ る。[30] 政府はアルコール消費を抑えようと法律を制定し始めたが、オーストラリア南部のワイン生産地域からの反対に常に遭った。政府は違法薬物、特に1950年代 に鎮痛剤として広く使用されるようになったヘロインとの戦いも展開した。 専門家は、太平洋諸島における多くの保健問題は、ヨーロッパによる植民地化と、それに続く島嶼社会のグローバル化と近代化に起因すると考えている。(太平 洋諸島の歴史を参照)ヨーロッパによる植民地化と遅れて訪れた独立は、近代化をもたらしたが、経済成長は緩慢で、太平洋諸島の保健医療、特に栄養状態に多 大な影響を与えた。植民地化の終結は医療資源の損失を意味し、独立したばかりの政府には、植民地政府が実施していた保健政策を継続する余裕がなかった。栄 養状態は劇的に変化し、さまざまな健康問題を引き起こした。都市部では食料を入手できるようになったが、栄養価の低い食事を選んだため栄養過多となり、肥 満、2型糖尿病、心血管疾患が極めて高いレベルで発生するようになった。一方、貧しい農村地域では、栄養失調とマラリアが依然として問題となっている。 [31] 太平洋諸島における伝統的な食事は脂肪分が非常に少ないが、第二次世界大戦以降、太平洋諸島の食事における脂肪分とタンパク質の摂取量は大幅に増加してい る。 体重に対する先住民の考え方も、肥満問題の一因となっている。 トンガの先住民は、特に男性の間で肥満を肯定的に捉えている。 また、女性はできるだけ肉体労働をせず、男性が養ってくれるべきだと考えている。つまり、運動をほとんどしないということだ。[31] |
| Europe The largest endeavors to improve health across Europe is the World Health Organization European Region.[32] The goal is to improve the health of poor and disadvantaged populations by promoting healthy lifestyles including environmental, economic, social and providing health care.[32] Overall health in Europe is very high compared to the rest of the world.[32] The average life expectancy is around 78 in EU countries but there is a wide gap between Western and Eastern Europe. It is as low as 67 in Russia and 73 in the Balkan states.[32] Europe is seeing an increase in the spread of HIV/AIDS in Eastern Europe because of a worsening socioeconomic situation.[32] Cardiovascular disease, cancer and diabetes mellitus are more prevalent is Eastern Europe.[32] The WHO claims that poverty is the most important factor bringing on ill health across Europe.[32] Those at low socioeconomic status levels and many young people are also at risk because of their increased tobacco, alcohol, and non-medical substance use.[32] Health and illness prevention in Europe is largely funded by the governmental services including: regulating health care, insurance and social programs.[32] The role of religion and traditional medicine, however, is often left unexamined in such reports. The study of hypertension within the United Kingdom has turned to examining the role that beliefs play in its diagnosis and treatment. Hypertension is an essential topic for study since it is linked to increased risk of stroke and coronary heart disease. The most common treatment for hypertension is medication but compliance for this treatment plan is low.[33] A study conducted in the UK examined the differences between 'white' patients and first generation immigrants from the West Indies. There were differing reasons for non-compliance that involve the patients' perception and beliefs about the diagnosis. Patients commonly believe that high levels of anxiety when first diagnosed are the major cause and think that when stress levels decline so too will their hypertension. Other respondents in this UK based study had varying beliefs concerning the necessity of medication while others still argued that it was the side effects of medication that made them end their prescribed regimen.[33] West Indian respondents whose lay culture teaches them to reject long-term drug therapy opted instead for folk remedies in higher numbers than the 'white' respondents. What can be seen here is that some people will choose to ignore a doctor's expert advice and will employ 'lay consultation' instead.[33] 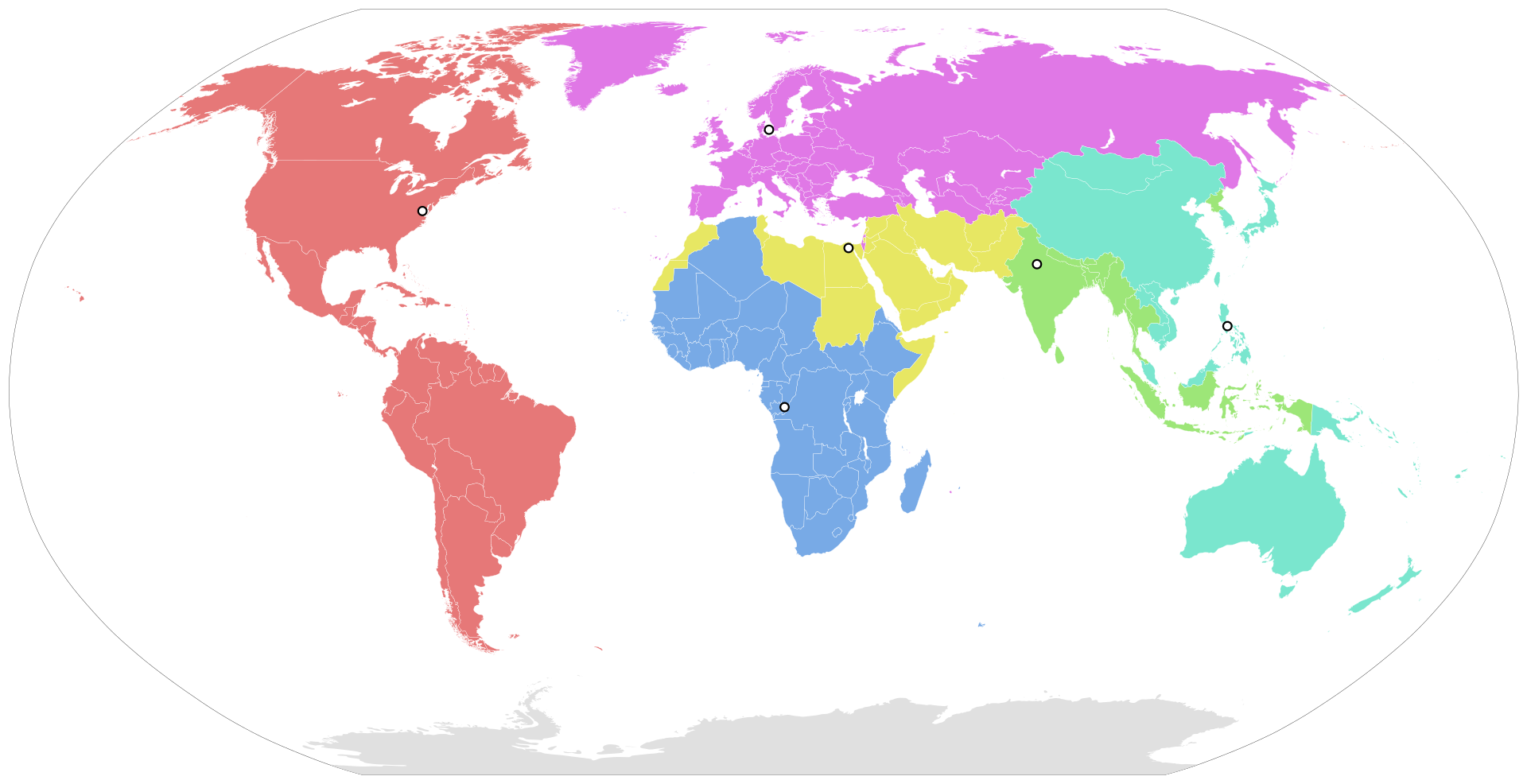 Regions of the WHO Before people seek medical help they try to interpret the symptoms themselves and often consult people in their lives or use 'self-help' measures.[34] A study of 'everyday illness' in Finland including: influenza, infections and musculo-skeletal problems focused on reasons for consulting medical experts and explanations of illness. These common illness were examined not because of their seriousness but because of their frequency. The researchers explain five possible triggers that people seek medical aid: 1- the occurrence of an interpersonal crisis 2- perceived interference with social and personal relations 3- perceived interference with vocational & physical activity 4- sanctioning by other people 5- patients' ideas about how long certain complaints should last. These kind of explanatory models are part of the process that people use to construct medical culture.[34] They give meaning to illness and health, answer questions about personal responsibility about health and most importantly are part of the dialogue between patients' and professionals' illness explanations. It can help explore why some patients will follow a doctors instructions to the letter and others ignore them completely. A patient's explanation or understanding of their illness can be much broader than a physician's and this dynamic has become a major criticism of modern medical practice since it normally excludes the "social, psychological and experiential dimensions of illness."[34] The Finnish study examined 127 patients and the results have been different from findings in other countries where there is more 'lay consultation'. Half of the respondents did not have any lay consultation before coming to the doctors office. One-third did not try any self-treatment and three-quarters of the sample consulted the doctor within three days of symptoms developing.[34] Possible explanations are that in Finland there is an aspect "over-protectiveness" within their health care system. Many[who?] might conclude that the Finnish people are dependent and helpless but the researchers of this study found that people chose to consult professionals because they trusted them over some lay explanation. These results echo similar studies in Ireland that explain this phenomenon as being based in a strong work ethic. Illness in these countries will affect their work and Finnish people will quickly get treatment so they can return to work. This research out of Finland also describes that this relationship between patient and doctor is based on: national and municipal administrative bureaucracies that demand more output and more satisfied patients the public demanding better care nurses criticizing physicians for not taking a holistic view of patients hospital specialists wanting better/earlier screening for serious illnesses (e.g. cancer).[34] The conflict between medical and lay worlds is prominent. On one hand many patients believe they are the expert of their own body and view the Doctor-patient relationship as authoritarian. These people will often use knowledge outside the medical field to deal with health and illness. Others see the doctor as the expert and are shy about describing their symptoms and therefore rely on the doctor for diagnosis and treatment.[34] In Europe, sociology of health and illness is represented by the European Society for Health and Medical Sociology (ESHMS). |
ヨーロッパ ヨーロッパ全土で保健の改善に最も力を入れているのは世界保健機関(WHO)のヨーロッパ地域事務局である。[32] 環境、経済、社会、医療の提供など、健康的なライフスタイルの促進を通じて、貧困層や恵まれない人々の健康状態を改善することが目標である。[32] ヨーロッパの保健状態は、世界的に見ても非常に高い。[32] EU諸国の平均余命はおよそ78歳であるが、西欧と東欧の間には大きな格差がある。ロシアでは67歳、バルカン諸国では73歳と低い。[32] 欧州では、社会経済状況の悪化により、東欧でのHIV/AIDSの感染拡大が増加している。[32] 東欧では、心臓血管疾患、癌、糖尿病がより多く見られる。[32] WHOは、欧州全域で健康を損なう最も重要な要因は貧困であると主張している。 [32] 社会経済的地位が低い人々や多くの若者も、たばこやアルコール、非医療用物質の使用が増えているため、リスクにさらされている。[32] 欧州における保健および疾病予防は、主に政府サービスによって資金提供されており、その中には医療、保険、社会プログラムの規制も含まれる。[32] しかし、宗教や伝統医療の役割は、このような報告書ではしばしば検討されないままである。 英国における高血圧の研究では、診断と治療における信念の役割が調査されるようになった。高血圧は脳卒中や冠動脈性心臓病のリスクを高めるため、研究の重 要なテーマとなっている。高血圧の最も一般的な治療法は薬物療法であるが、この治療計画の順守率は低い。[33] 英国で実施されたある研究では、「白人」患者と西インド諸島からの第一世代移民との違いが調査された。 服薬を順守しない理由は様々であり、患者の診断に対する認識や信念が関わっている。 患者は一般的に、最初に診断された際の強い不安が主な原因であると考え、ストレスレベルが低下すれば高血圧も改善すると考えている。この英国を拠点とした 研究の他の回答者は、薬物療法の必要性についてさまざまな考えを持っており、また、薬物療法の副作用が原因で処方された治療を中断したと主張する回答者も いた。[33] 長期の薬物療法を拒否することを教える素人文化を持つ西インド諸島の回答者は、代わりに民間療法を選択する傾向が「白人」の回答者よりも高かった。ここで 見られるのは、一部の人々は専門家の医師の助言を無視し、代わりに「素人相談」を利用するという選択をするということである。 WHOの地域 人々は医療支援を求める前に、自分自身で症状を解釈しようとし、しばしば身近な人に相談したり、「自己治療」の手段を講じたりする。[34] フィンランドにおける「日常的な病気」に関する研究では、インフルエンザ、感染症、筋骨格系の問題など、医療専門家に相談する理由と病気の説明に焦点を当 てた。これらの一般的な病気は、深刻な病気であるからではなく、頻繁に起こる病気であるために調査された。研究者は、人々が医療支援を求める5つの可能性 のある誘因を説明している。1- 人間関係の危機の発生 2- 社会および個人的関係への干渉の認識 3- 職業および身体活動への干渉の認識 4- 他者による制裁 5- 特定の苦情がどのくらい続くべきかについての患者の考え。この種の説明モデルは、人々が医療文化を構築する際に用いるプロセスの一部である。[34] 病気と保健に意味を与え、保健に関する個人の責任についての疑問に答え、そして最も重要なのは、患者と専門家の病気の説明の間の対話の一部である。このモ デルは、ある患者が医師の指示を忠実に守る一方で、他の患者はそれを完全に無視する理由を解明するのに役立つ。患者が自身の病気を説明したり理解したりす る方法は、医師のそれよりもはるかに幅広い可能性があり、このダイナミクスは通常「病気の社会的、心理的、経験的側面」を除外しているため、現代の医療行 為に対する主な批判となっている。[34] フィンランドの研究では127人の患者を対象に調査が行われたが、その結果は「素人による相談」がより多く存在する他の国々での調査結果とは異なってい る。回答者の半数は、医師の診察を受ける前に素人による相談を受けていなかった。また、3分の1は自己治療を試しておらず、サンプルの4分の3は症状が現 れてから3日以内に医師に相談していた。[34] 考えられる説明としては、フィンランドの保健医療システムには「過保護」な側面があることが挙げられる。多くの人々は(出典不明)、フィンランドの人々は 依存的で無力だと結論づけるかもしれないが、この研究の研究者たちは、人々が専門家に相談することを選ぶのは、素人判断よりも専門家を信頼しているからだ と結論づけている。この結果は、アイルランドにおける同様の研究結果を反映しており、この現象は強い労働倫理に基づいていると説明している。これらの国々 では、病気は仕事に影響を及ぼすため、フィンランドの人々はすぐに治療を受け、仕事に復帰できる。フィンランド国外で行われたこの研究では、患者と医師の 関係は、 国民および地方自治体の行政官僚が、より多くの成果とより満足した患者を要求していること より良い医療を求める国民 患者を全体的に見ていないとして医師を批判する看護師 深刻な病気(例えば癌)に対するより良い/より早いスクリーニングを望む病院の専門家[34] 医療界と素人との間の対立は顕著である。一方、多くの患者は、自分の体の専門家は自分自身であると信じており、医師と患者の関係を権威主義的なものと見な している。こうした人々は、保健や病気に対処する際に医療分野以外の知識をしばしば利用する。また、医師を専門家と見なし、症状を説明することにためらい を覚えるため、診断や治療を医師に委ねる人もいる。 ヨーロッパでは、保健と病気の社会学は、ヨーロッパ保健・医療社会学会(ESHMS)によって代表されている。 |
North America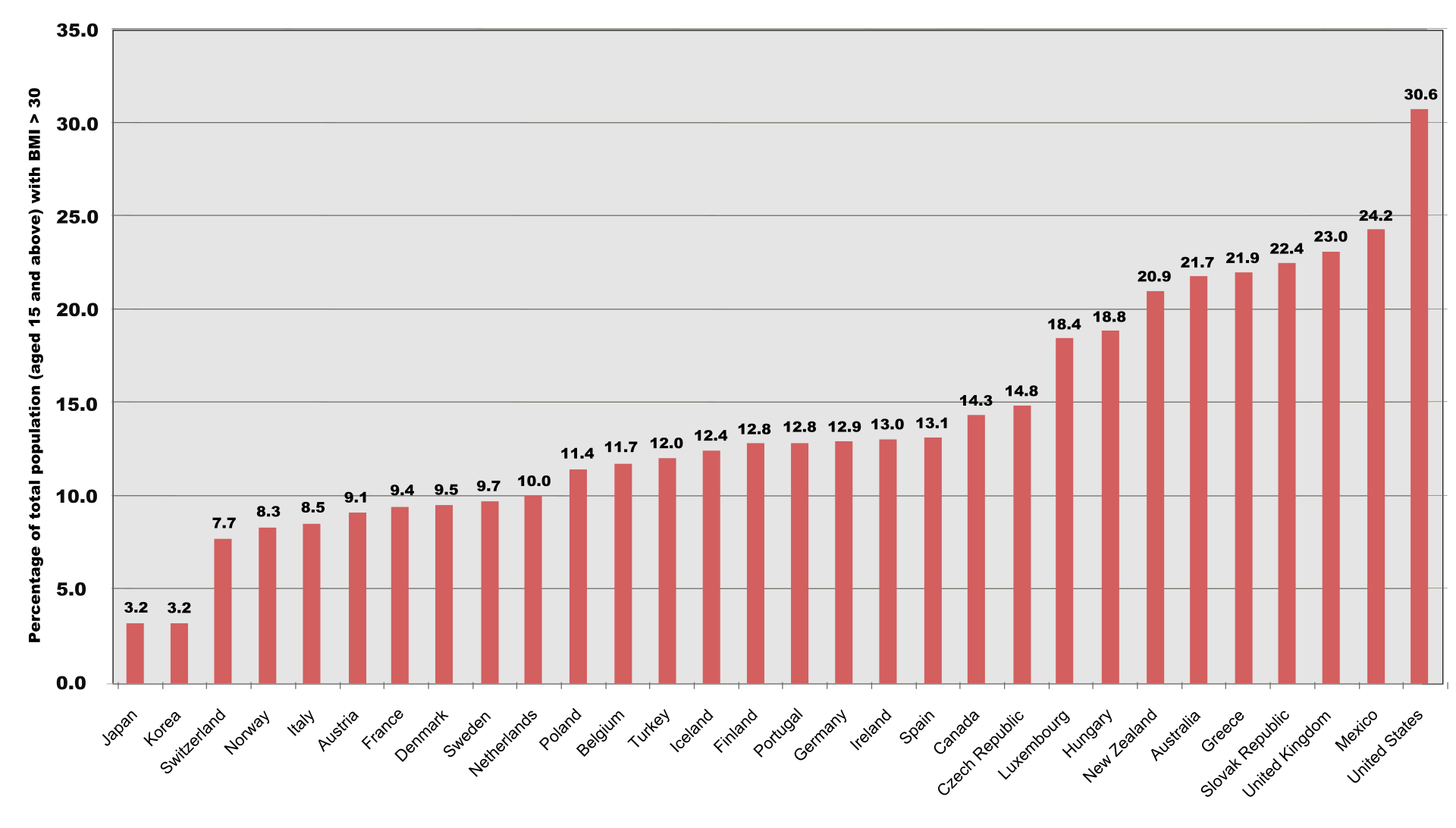 Compares figures in the population of OECD countries and the percentage of total population (aged 15 and above) with a body mass index greater than 30. Data was collected between 1996 and 2003. North America is a fairly recent settled continent, made up of the United States, Canada, Mexico, Central America, and the Caribbean. It was built by an amalgamation of wealth, ideas, culture, and practices. North America is highly advanced intellectually, technologically, and traditionally. This advantageous character of North American nations has caused a high average life expectancy of 75 years for males and 80 years for females. This leads to the conclusion that North America has cultivated a comparatively healthy society. As North America contains several core nations, the growing economies in those nations are able to maintain and develop medical institutions. This subsequently provides more access to health care for American citizens but health care is not universal. North America is known for being a leading nation in regards to industrialization and modernization, but the United States lacks federal laws regarding health care as a basic human right. This lag of health care security causes subsequent issues with pharmaceutical competition, lack of care for the elderly, and little attention to alternative medicine.[35] Health care and education are plentiful at a price and illness still persists for many reasons.[36] A main reason is that a lower- and middle-class population still exists in plentiful numbers, maintaining a group that is highly vulnerable to physical ailment. 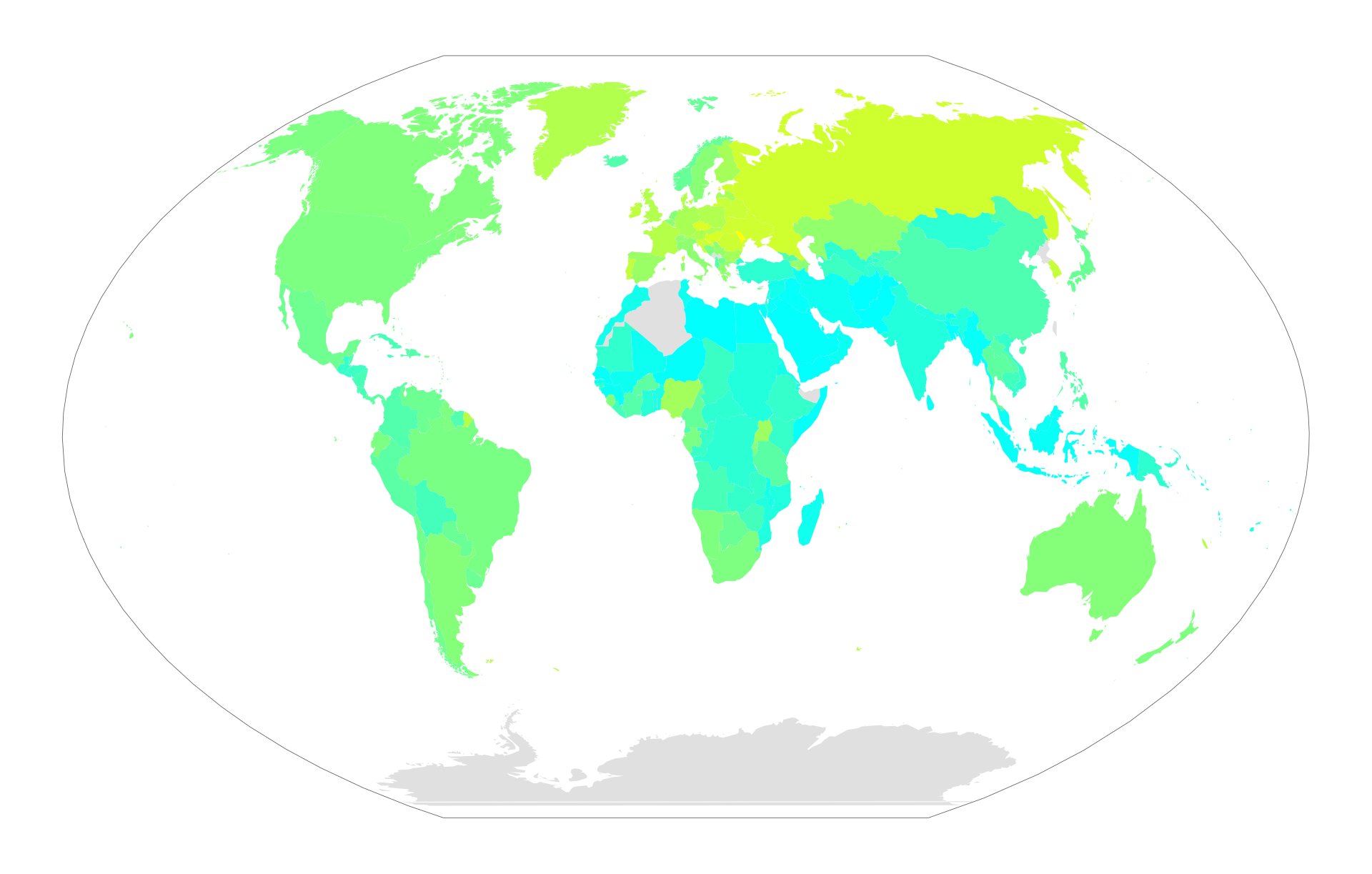 World map showing alcohol consumption around the world North America's primary risk factors for illness are currently[when?] excessive alcohol use, malnutrition, obesity, tobacco use, and water sanitation.[36] Obesity is a recent epidemic in North America. The 1990s brought a rise in the average Body Mass Index, or BMI. From the beginning and to the end of the decade, the median percent of adults who were obese rose from 12% to 20%.[36] Alcoholism is the addiction of over-consumption of alcohol and is highly prevalent in the US. There are high incidence rates in many other world regions. Roughly 61% of American adults drank in 2007, and 21% of current drinkers consumed five or more drinks at one point in the last year. There have also been 22,073 alcohol induced deaths in the United States in the past year, about 13,000 of which were related to liver disease.[37] Alcoholism has many risk factors ingrained in North American culture, such as heredity, stress from competition or availability. The Swine Flu (also known as H1N1) epidemic is a recent disease emerging in the early 21st century. In April 2009, during the early days of the outbreak, a molecular biologist named Dr. Henry Miller wrote in the Wall Street Journal about New York City high-school students. These students apparently brought the virus back from Mexico and infected their classmates.[38] All six cases so far reported in Canada were connected directly or indirectly with travel to Mexico as well. Flu viruses can be directly transmitted (via droplets from sneezing or coughing) from pigs to people, and vice versa. These cross-species infections occur most commonly when people are close to large numbers of pigs, such as in barns, livestock exhibits at fairs, and slaughterhouses. The flu is transmissible from human to human, either directly or via contaminated surfaces."[38] |
北米 OECD諸国の人口における数値と、BMIが30を超える人口の割合(15歳以上)を比較する。データは1996年から2003年の間に収集された。 北米は、米国、カナダ、メキシコ、中央アメリカ、カリブ海地域から成る、比較的新しく開拓された大陸である。この大陸は、富、アイデア、文化、慣習の融合 によって築き上げられた。北米は、知的にも、技術的にも、伝統的にも非常に高度な地域である。北米諸国のこうした有利な特性により、平均寿命は男性で75 歳、女性で80歳と高い。このことから、北米は比較的健全な社会を築いてきたという結論が導かれる。北米には複数の主要国が存在するため、それらの国々に おける経済成長により医療機関の維持と発展が可能となっている。その結果、アメリカ国民はより手軽に医療サービスを受けられるようになったが、医療が万人 に行き渡っているわけではない。北米は工業化と近代化を牽引する国として知られているが、アメリカには保健医療を基本的人権として保障する連邦法が存在し ない。この医療保障の遅れは、医薬品競争、高齢者へのケア不足、代替医療への関心の低さといった問題を引き起こしている。[35] 保健と教育は充実しているが、さまざまな理由で病気は依然として蔓延している。[36] 主な理由は、低所得者層と中流階級が依然として多数存在し、身体的な不調に非常に弱い集団を形成していることである。 世界のアルコール消費量を示す世界地図 北米における主な疾病リスク要因は、現在[いつ?]、過剰なアルコール摂取、栄養不良、肥満、喫煙、水の衛生状態である。[36] 肥満は北米における最近の流行病である。1990年代には平均ボディマス指数(BMI)が上昇した。1990年代の初めから終わりにかけて、肥満の成人が 占める割合の中央値は12%から20%に上昇した。[36] アルコール依存症はアルコールの過剰摂取による中毒であり、米国では非常に多く見られる。他の多くの世界の地域でも高い発生率が見られる。2007年に は、米国成人の約61%が飲酒しており、現飲酒者の21%は、過去1年間に5杯以上の飲酒を1度でも経験している。また、過去1年間に米国でアルコールが 原因で死亡した人は22,073人に上り、そのうち約13,000人は肝臓疾患が原因であった。[37] アルコール依存症には、遺伝や競争によるストレス、入手のしやすさなど、北米文化に深く根付いた多くのリスク要因がある。 新型インフルエンザ(H1N1としても知られる)は、21世紀初頭に発生した最近の病気である。2009年4月、発生初期に、分子生物学者のヘンリー・ミ ラー博士がウォールストリート・ジャーナル紙に、ニューヨーク市の高校生について書いた。これらの生徒はメキシコからウイルスを持ち帰り、クラスメートに 感染させたようである。[38] カナダでこれまでに報告された6件の症例もすべて、直接的または間接的にメキシコへの渡航と関連していた。インフルエンザウイルスは、豚から人へ、またそ の逆にも、直接感染(くしゃみや咳による飛沫感染)することがある。このような種を越えた感染は、人が多数の豚に近づく場合、例えば畜舎や家畜展示場、食 肉処理場などで最もよく起こる。インフルエンザは、直接感染または汚染された表面を介して、人から人へ感染する可能性がある。」[38] |
| South America There are many diseases that affect South America, but two major conditions are malaria and Hepatitis D. Malaria affects every country in South America except Uruguay, Chile, and The Falkland Islands. Elevation is a major factor in the areas where malaria is found. The disease is spread from person to person via mosquito bites. People are typically bitten by mosquitoes at dusk and dawn. Symptoms of this disorder are: high fever, chills, sweating, headaches, body aches, weakness, vomiting and diarrhea. If left untreated, new symptoms can occur; people that are infected may experience seizures, delirium and coma. Severe cases may end in death. Malaria can be cured, but the symptoms may not become noticeable until months later. There are three forms of medication that can cure Malaria. An infected person's accessibility to these drugs is dependent upon their access to medical care and their financial situation. Literature about Malaria treatment typically is focused toward people who are tourists. Most sources are not written with the native in mind.[39] 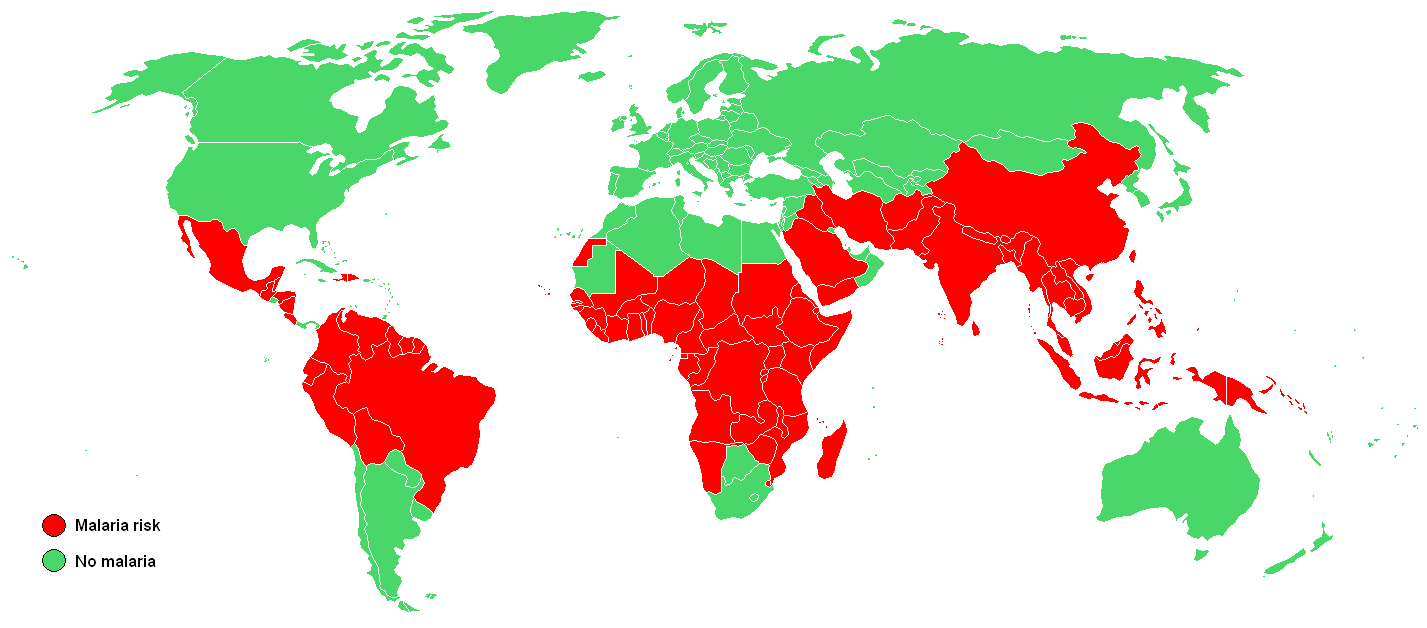 Malaria The first sign of Hepatitis D was detected in 1978 when a strange and unrecognizable internuclear antigen was discovered during a liver biopsy of several Italians who developed HBV infections. Scientists initially thought that it was an antigenic specificity of HBV, but they soon found that it was a protein from another disease altogether. They called it "Hepatitis Delta Virus" (HDV). This new virus was found to be defective. HDV needed HBV to act as a helper function in order for it to be detected. Normally Hepatitis B is transmitted through blood or any type of blood product. In South America Hepatitis D was found to be fatal. Scientists are still unsure in what way this disease was being transmitted throughout certain South American countries. Sexual contact and drug use are the most common means of transmission. HDV is still considered an unusual form of hepatitis. Agents of this virus resemble that of plant viroids. It is still hard to tell how many stereotypes exist because HDV is under the umbrella of HBV. HDV causes very high titers in the blood of people who are infected. Incubation of Hepatitis D typically lasts for thirty five days. Most often Hepatitis D is a co-infection with Hepatitis B or a super-infection with chronic hepatitis. In terms of super infections there are high mortality rates, ranging seventy to eighty percent; in contrast with co-infections which have a one to three percent mortality rate. There is little information with the ecology of Hepatitis D. Epidemics have been found in Venezuela, Peru, Columbia, and Brazil. People who are treated for Hepatitis B have been able to control Hepatitis D. People who have chronic HDB will continue to get HDV.[40] Another disease that affects South America is HIV and AIDS. In 2008 roughly two million people had HIV and AIDS. By the end of 2008 one hundred and seventy thousand people were infected with AIDS and HIV. Seventy seven thousand people died from this disease by the end of that year. Brazil has the most people that are affected with AIDS and HIV in South America. In Brazil sixty percent of the inhabitants are HIV positive because of drug use. Usually this disease is transmitted by either drug use involving needles or unprotected sex. Sharing needles and being infected with HIV and AIDS is most common in Paraguay and Uruguay. South America is trying to get treatment to the thousands of people infected by this disease. Brazil is offering generic AIDS prescriptions that are much less expensive than the name brand drugs. One hundred and eighty-one thousand inhabitants in Brazil who were infected are being treated. That accounts for eighty percent of those who needed immediate help. This aid from the government has had positive results. Statistics show that there was a fifty percent decrease in mortality rates, approximately sixty to eighty percent decrease in morbidity rates and a seventy percent decrease in hospitalization of infected people.[41] In very remote areas of South America, traditional healers are the only forms of health care people have.[42] In north Aymara and south Mapuche, where the indigenous groups have the strongest voices, they still heavily use traditional medicine. The government in Chile has implemented an Indigenous Health System to help strengthen the health care system. Even with Chile's indigenous groups, Chile still has the best public health services in South America.[citation needed] They also have the lowest mortality rates in the area. Their health care policies are centered around family and community wellbeing by focusing on the strategies for prevention health strategies. Reports have shown an increase in mental health issues, diabetes, and cardiovascular diseases.[43] South America's economy is developing rapidly and has a great deal of industries.[citation needed] The major industry in South America are agriculture. Other industries are fishing, handicrafts, and natural resources. Its trade and import-export market is continually thriving. In the past South American countries moved slowly in regards to economic development. South America began to build its economy ever since World War II. South America's largest economies are Brazil, Chile, Argentina, and Columbia. Venezuela, Peru, and Argentina's economy are growing very rapidly.[44] |
南アメリカ 南アメリカには多くの疾病が存在するが、そのうちの2つの主要な疾患はマラリアとD型肝炎である。マラリアはウルグアイ、チリ、フォークランド諸島を除く 南アメリカのすべての国で発生している。マラリアが発生する地域では標高が主な要因となっている。この病気は蚊に刺されることで人から人へと感染する。人 々は通常、夕暮れ時や夜明けに蚊に刺される。この疾患の症状は、高熱、悪寒、発汗、頭痛、身体の痛み、脱力感、嘔吐、下痢などである。治療せずに放置する と、新たな症状が現れる可能性がある。感染した人は、発作、錯乱、昏睡状態になる可能性もある。重症の場合は死に至ることもある。マラリアは治療可能であ るが、症状が顕著になるまで数ヶ月かかる場合もある。マラリアを治療できる薬は3種類ある。感染者がこれらの薬品を入手できるかどうかは、医療へのアクセ スと経済状況に左右される。マラリア治療に関する文献は、通常、旅行者向けに書かれている。ほとんどの情報源は、現地の人向けに書かれていない。[39] マラリア D型肝炎の最初の兆候は、HBV感染を発症したイタリア人数名の肝生検中に、奇妙で認識できない核間抗原が発見された1978年に検出された。科学者たち は当初、これはHBVの抗原特異性であると考えたが、すぐにそれはまったく別の疾患のタンパク質であることが判明した。彼らはそれを「デルタ型肝炎ウイル ス(HDV)」と名付けた。この新しいウイルスは欠陥があることが判明した。HDVはHBVの助けを借りて初めて検出される。通常、B型肝炎は血液または 血液製剤を介して感染する。南米では、D型肝炎は致命的なことが分かっている。科学者たちは、この病気が南米の特定の国々でどのように感染しているのか、 まだ分かっていない。性行為と薬物の使用が最も一般的な感染経路である。HDVは依然として、珍しいタイプの肝炎と考えられている。このウイルスの因子は 植物ウイロイドのそれに類似している。 HDVはHBVの傘下にあるため、いまだにどれほどの固定観念が存在するのかを判断するのは難しい。 HDVに感染した人の血液中には非常に高い抗体価が認められる。 D型肝炎の潜伏期間は通常35日間である。 D型肝炎は、B型肝炎との重感染または慢性肝炎の二次感染である場合がほとんどである。二次感染の場合、死亡率は70~80%と高いが、一次感染の場合は 死亡率は1~3%である。D型肝炎の生態についてはほとんど知られていない。ベネズエラ、ペルー、コロンビア、ブラジルで流行が確認されている。B型肝炎 の治療を受けた人はD型肝炎を抑制できる。HDBの慢性感染者は引き続きHDVに感染する。 南米に影響を及ぼしている別の病気はHIVとAIDSである。2008年にはおよそ200万人がHIVとAIDSに感染していた。2008年末までに17 万人がAIDSとHIVに感染した。その年末までに7万7千人がこの病気で死亡した。ブラジルは南米で最もAIDSとHIVに感染している人が多い国であ る。ブラジルでは人口の60%が麻薬の使用によりHIVに感染している。通常、この病気は、注射針の使いまわしによる麻薬の使用や、無防備な性行為によっ て感染する。 注射針の共用によるHIVおよびエイズへの感染は、パラグアイとウルグアイで最も多い。 南米では、この病気によって感染した何千人もの人々への治療を試みている。 ブラジルでは、ブランド薬よりもはるかに安価なジェネリック医薬品のエイズ治療薬を処方している。 感染したブラジル国民18万1000人が治療を受けている。 これは、緊急の支援を必要とした人々の80%に相当する。この政府による支援は、良い結果をもたらしている。統計によると、死亡率は50%減少し、罹患率 は約60~80%減少し、感染者の入院率は70%減少した。[41] 南米の非常に辺境の地域では、伝統的な治療師が人々が利用できる唯一の医療形態である。[42] 先住民グループが最も強い発言力を持つ北アイマラ族と南マプチェ族では、伝統的な医療が今でも広く利用されている。チリ政府は、医療制度の強化を目的とし て、先住民医療制度を導入している。チリの先住民グループにおいても、チリは南米で最も優れた公衆衛生サービスを提供している。[要出典] また、この地域の死亡率も最も低い。保健政策は、予防保健戦略に重点を置くことで、家族と地域社会の幸福を中心に展開されている。報告書によると、精神衛 生上の問題、糖尿病、心血管疾患が増加していることが示されている。[43] 南米の経済は急速に発展しており、多くの産業がある。[要出典]南米の主要産業は農業である。その他の産業には、漁業、手工芸、天然資源がある。貿易およ び輸出入市場は、継続的に活況を呈している。過去においては、南米諸国の経済発展は遅々としていた。南米は第二次世界大戦以降、経済発展を始めた。南米最 大の経済規模を持つ国は、ブラジル、チリ、アルゼンチン、コロンビアである。ベネズエラ、ペルー、アルゼンチンの経済は急速に成長している。[44] |
| Journals Sociology of Health and Illness Social Science and Medicine Health: An Interdisciplinary Journal for the Social Study of Health Illness and Medicine Social Theory and Health Health, Risk and Society |
ジャーナル 健康と病気の社会学 社会科学と医学 保健:保健の社会科学的研究のための学際的ジャーナル 病気と医学 社会理論と保健 保健、リスク、社会 |
| Alternative medicine Medicalization Epidemiology Naturalistic disease theories European Society for Health and Medical Sociology |
代替医療 医学化 疫学 自然主義的疾病理論 ヨーロッパ保健・医療社会学会 |
| Nettleton, Sarah (2006). The Sociology of Health and Illness. Polity. ISBN 0-7456-2828-1. Conrad, Peter (2008). The Sociology of Health and Illness. Macmillan. ISBN 978-1-4292-0558-0. Porter, Dorothy (1999). Health, Civilization, and the State A History of Public Health from Ancient to Modern Times. Routledge. ISBN 978-0-415-12244-3. United Nations Industrial Development Organization (1978). Technologies from Developing Countries. ISBN 978-0-7619-6400-1. Seale, Gabe, Wainwright, Williams. Sociology of Health & Illness, Vol. 33 2011 ISSN 1467-9566 |
ネトルトン、サラ(2006年)。『保健と疾病の社会学』。Polity。ISBN 0-7456-2828-1。 コンラッド、ピーター(2008年)。『健康と病気の社会学』マクミラン。ISBN 978-1-4292-0558-0。 ポーター、ドロシー(1999年)。『健康、文明、国家:古代から現代までの公衆衛生の歴史』ルードリッジ。ISBN 978-0-415-12244-3。 国際連合工業開発機関 (1978). 開発途上国発の技術。ISBN 978-0-7619-6400-1. Seale, Gabe, Wainwright, Williams. 保健と疾病の社会学、第33巻、2011年、ISSN 1467-9566 |
| https://en.wikipedia.org/wiki/Sociology_of_health_and_illness |
リ ンク
文 献
そ の他の情報
Copyleft,
CC, Mitzub'ixi Quq Chi'j, 1996-2099