Clinical Ethics
臨床倫理
Clinical Ethics
臨床倫理(Clinical ethics)とは、保健ケアとくに医療に関す る倫理的事象(=医療倫理) のことである。臨床倫理学すなわち医療倫理学、医療のみならず、生物学、政治学、 社会学、文化人類学、法学、哲学などのさまざまな分野と関連性をもつ、学際的な研究分野である。生命倫理学(bioethics, バイオエシックス)と医療倫理学はテーマを共有することが多いので、医療倫理学あるいは臨床倫理学と「基本的に同じ」と判断しても間違いではないだろう。 私は、別項で生命倫理学を次のように定義した「人間を対象にした治療および実験に関する倫理・道徳、ひいてはそれらに関する諸研究」(→ 出典「生命倫理学と医療人類学」「医療倫理学」)
臨床倫理、すなわち医療倫理学は、医療倫理(リンク先はウィキペ ディア日本語)という歴史に先行する経験的事実と原則に依存する、すなわち先例拘束の原則(stare decisis)があるので、そのことを次に解説しよう(Weise, Mary Victoria, Medical Ethics Made Easy, 2016)。なおこのページは「医療倫理学」のページから独立したものであり、その内容は当該のページと重複していることをお断りしておく。
医療倫理の4原則というものがもっとも有名である。すなわち、1)自己決 定(Autonomy)、2)善行(Benevolence)、3)無加害(Nonmaleficence)、そして、4)配分上の正義 (Distributive Justice)
★現在のバイオエシックス(生命倫理学) は、(1)哲学・倫理学の伝統を引き継ぐ「原則主義(Principlism)」と、 (2)臨 床倫理(clinical ethics)に大別され、実際の医療倫理(medical ethics)の現場で、この2つの流れがしばしば、対立、交渉、相互無視を通して並存状態にある。前者の原則主義(Principlism)では、抽象的な原則レベルでは、関係者の間の合意は可能であり、抽象原則への合意をもとに倫理的判断をおこなうべきだと考える。それに対して後者の臨 床倫理(clinical ethics)では、直観的な判断が可能な具体的な現場——(例)臓器移植の臨床現場で医療資源の社会的配分などは議論されずに組織適合性や予測される余命から〈適切さ〉の判断が導き出される——を軸にして決疑論(casuistry)的に推論が行われるべきだと考える。
| Clinical
ethics is the practical application of morality and ethical principles
to healthcare to improve patient care by identifying, analyzing, and
resolving ethical dilemmas. It provides a structured framework for
healthcare professionals, patients, and families to navigate complex
situations by applying core ethical principles like autonomy,
beneficence, non-maleficence, and justice. Clinical ethicists offer
support through consultations, education, and policy development within
healthcare systems to ensure patient well-being and uphold ethical
standards. +++ Clinical ethics is a field of applied ethics that addresses moral issues arising in direct patient care. It is a practical branch of the broader field of bioethics, offering healthcare professionals a structured approach to identify, analyze, and resolve ethical dilemmas that occur at the bedside. These situations often arise from disagreements or misunderstandings of different values and priorities among patients, their families, and the healthcare team. |
臨
床倫理とは、医療現場において道徳と倫理原則を実践的に適用し、倫理的ジレンマを特定・分析・解決することで患者ケアを向上させるものである。自律性、善
行、非加害、公正といった中核的倫理原則を適用することで、医療従事者、患者、家族が複雑な状況を乗り切るための体系的な枠組みを提供する。臨床倫理専門
家は、医療システム内でのコンサルテーション、教育、政策立案を通じて支援を行い、患者の福祉を確保し倫理基準を維持する。 ++++++ 臨床倫理とは、直接的な患者ケアにおいて生じる道徳的問題を扱う応用倫理学の一分野である。これはより広範な生命倫理学の実践的分科であり、医療従事者に 病床で発生する倫理的ジレンマを特定・分析・解決するための体系的なアプローチを提供する。こうした状況は、患者、その家族、医療チームの間で異なる価値 観や優先順位に関する意見の相違や誤解から生じることが多い。 |
| Key Concepts Application of Morality: Clinical ethics applies the science of morality to medical and health practices to make sound decisions in patient care. Structured Approach: It offers a systematic method for healthcare professionals to identify, analyze, and resolve ethical issues in patient care. Broader Field of Bioethics: Clinical ethics is a practical component of bioethics, which studies ethical issues in life sciences and healthcare. |
主要概念 道徳の応用:臨床倫理は、医療と健康実践において道徳の科学を応用し、患者ケアにおいて適切な判断を下すものである。 体系的なアプローチ:医療従事者が患者ケアにおける倫理的問題を特定し、分析し、解決するための体系的な方法を提供する。 生命倫理学のより広い分野:臨床倫理は、生命科学と医療における倫理的問題を研究する生命倫理学の実践的要素である。 |
| Core principles of clinical ethics The most widely used framework for navigating clinical ethics is "principlism," based on four fundamental principles. Autonomy: This principle respects a competent patient's right to make their own decisions about their medical care based on their personal values. It is the basis for informed consent, truth-telling, and respecting a patient's confidentiality. Conflicts can arise when a patient's choices conflict with a clinician's recommendations for their well-being. Beneficence: This is the healthcare provider's obligation to act for the benefit of the patient. It is a positive duty that involves preventing, removing, and not inflicting harm. In some cases, beneficence may conflict with patient autonomy, for example, if a patient refuses a life-saving treatment. Non-maleficence: Rooted in the Hippocratic Oath's "do no harm," this principle states that a healthcare provider should not inflict harm upon a patient. A key aspect is weighing the benefits of a treatment against its potential burdens and risks. Justice: This principle requires that care is provided fairly and equitably. In clinical practice, this includes considering the fair distribution of scarce resources, such as organ transplants, without discriminating based on factors like age, gender, or race. |
臨床倫理の核心原則(→Principlism; 原則主義) 臨床倫理を導く最も広く用いられる枠組みは「原理主義」であり、四つの基本原則に基づいている。 自律性:この原則は、判断能力のある患者が自身の価値観に基づき医療に関する決定を行う権利を尊重する。インフォームド・コンセント、真実の告知、患者の 秘密保持の尊重の基盤となる。患者の選択が、医療従事者が患者の福祉のために推奨する内容と矛盾する場合、対立が生じることがある。 善行の原則:これは医療提供者が患者の利益のために行動する義務である。積極的な義務であり、危害の予防、除去、加害の回避を含む。例えば患者が救命治療を拒否する場合など、善行の原則は患者の自律性と対立することがある。 非加害の原則:ヒポクラテスの誓い「害をなすな」に根ざし、医療提供者は患者に害を与えてはならないと定める。治療の利益と潜在的な負担・リスクを比較検討することが重要である。 公正性:この原則は、医療が公平かつ平等に提供されることを求める。臨床現場では、臓器移植などの限られた資源を、年齢・性別・人種などの要因による差別なく公平に分配することを含む。 |
| Role of a Clinical Ethicist A clinical ethicist helps address ethical issues in a healthcare setting by: Consulting: Providing support and guidance on ethical dilemmas to healthcare teams, patients, and families. Educating: Offering education on important topics such as informed consent and advanced directives. Developing Policy: Contributing to the development of hospital policies on ethics-related matters. Representing Patients: Ensuring that patient values and preferences are central to the decision-making process. |
臨床倫理専門家の役割 臨床倫理専門家は、医療現場における倫理的問題に対処するため、以下の活動を行う: 相談:医療チーム、患者、家族に対し、倫理的ジレンマに関する支援と助言を提供する。 教育:インフォームド・コンセントや事前指示書など重要なテーマに関する教育を行う。 方針策定:倫理関連事項に関する病院方針の策定に貢献する。 患者代表:意思決定プロセスにおいて患者の価値観と希望が中心となるよう確保する。 |
| Examples of ethical dilemmas End-of-life care: Decisions about withholding or withdrawing life support, implementing a "Do Not Resuscitate" order, or discussing advance directives can create conflicts between patient autonomy and the medical team's desire to extend life. Informed consent: Issues can arise if a patient's capacity to understand and make decisions is in question due to their medical condition, especially if it affects their mental state. Resource allocation: During a public health crisis like a pandemic, clinicians may face difficult decisions about allocating scarce resources, such as ventilators, based on ethical criteria. Treatment disagreements: A patient or family may request treatments a clinician believes are unnecessary, burdensome, or not clinically indicated, leading to a clash of values. |
倫理的ジレンマの例 終末期医療:生命維持装置の中止や撤去、蘇生処置拒否指示の実施、事前指示書の話し合いといった決定は、患者の自律性と医療チームの延命願望との間で葛藤を生むことがある。 インフォームド・コンセント:患者の病状、特に精神状態に影響がある場合、理解や意思決定能力が疑問視されると問題が生じうる。 資源配分:パンデミックのような公衆衛生危機時には、臨床医は人工呼吸器などの限られた資源を倫理的基準に基づいて配分する難しい決断に直面する可能性がある。 治療方針の対立:患者や家族が、臨床医が不要、負担が大きい、あるいは臨床的に適応外と判断する治療を要求する場合があり、価値観の衝突を引き起こす。 |
| Why is Clinical Ethics Important? Navigating Complexity: It helps clarify the moral dimensions of clinical care, especially with advancements in medical technology and changing societal views. Improving Patient Care: By providing a structured approach to ethical challenges, it aims to enhance the quality of patient care. Fostering Trust: Adhering to ethical principles builds trust and confidence in the healthcare system. |
臨床倫理が重要な理由とは? 複雑さの対応:医療技術の進歩や社会観の変化に伴い、臨床ケアにおける道徳的側面を明確化する助けとなる。 患者ケアの向上:倫理的課題への体系的なアプローチを提供することで、患者ケアの質を高めることを目指す。 信頼の醸成:倫理原則を遵守することで、医療システムへの信頼と確信を築く。 |
| Google AI |
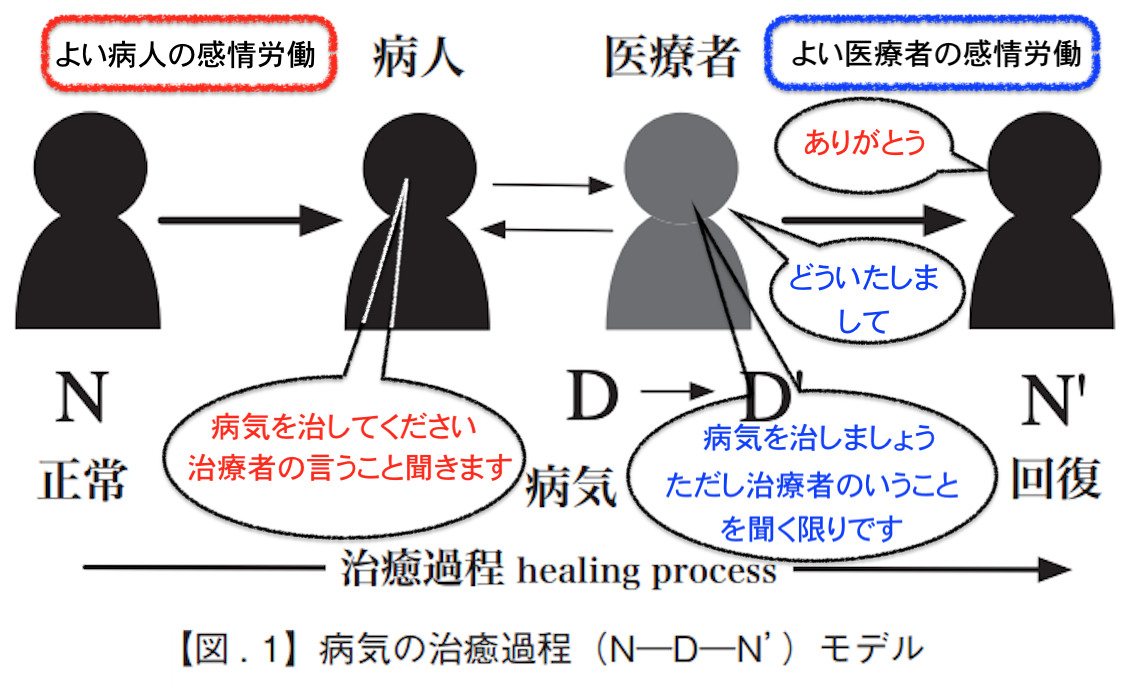
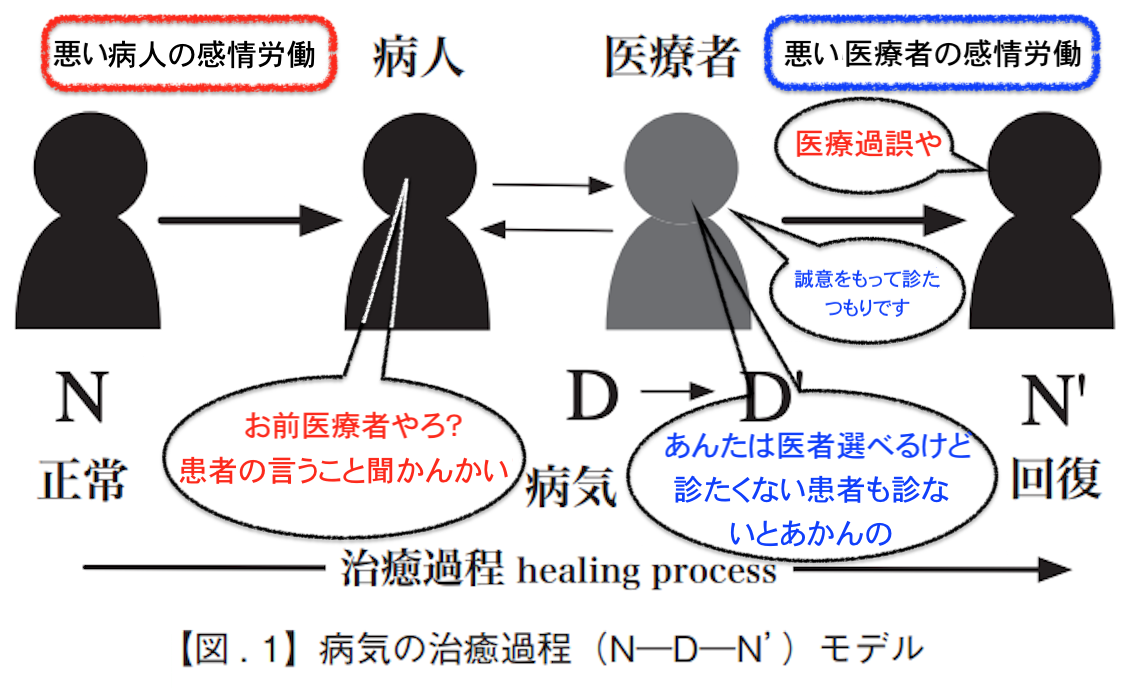
☆人と人のあいだの倫理原則と感情労働
これは、社会的存在としての人間が「世 間」を渡っていくときに、個人が社会ととり結ぶ関係性について考察するものである。しかし、これだけでは まだ足らない「倫理」や「道徳」という課題がある。すなわち、(b)人と人の関係と、(c)個人の中の内面における価値や実践の倫理(マルチン・ブーバー の用語だと「我」と「汝」、ジョージ・ハーバート・ミードだと、アイ(I)とミー(Me))の関係である。
(b)人と人の関係
人と人の関係を規定する倫理は「コミュニケーションの 倫理」(正確にはinter-personal communication)でもある。医療倫理の4原則というものがもっとも有名である。すなわち、1)自己決 定(Autonomy)、2)善行(Benevolence)、3)無加害(Nonmaleficence)、そして、4)配分上の正義(Distributive Justice)
よくいわれる、医療倫理実践における原則(出典:バーナード・ロウ[2003:12-21])
バーナード・ロウ『医療の倫理ジレンマ』北野喜良, 中澤英之, 小宮良輔監訳、新潟:西村書店。
(c)個人の中の内面における価値や実践 の倫理
個人の中の内面における価値や実践の倫理 (マルチン・ブーバーの用語だと「我」と「汝」、ジョージ・ハーバート・ミードだと、アイ(I)とミー (Me))の関係である
「われわ れはみな、甲胃を身にまとい、われわれに生ずるしるしを近づけぬようにしている。 しるしはたえず生じている。生きていることは、語りか けられていることであり、われわれはただこのしるしに立ち向かい、これに耳を傾けることだけが必要である。しかしこの冒険はわれわれにとって非常に危険な ものである。音のない雷は、われわれに破滅の威嚇をなすごとく見え、それゆえ、われわれは世代ごとに防禦の備えを完全なものにしようとする。われわれの知 識は、つぎのような確信を与える〈落着きなさい、すべては必然的に起るべくして起る。何もあなたに向けられているのではない、あなたがねらわれているので はない。まさにこのようなのが世界である。あなたは自分で望むままに世界を体験することができる。しかしあなたが心の中でいつも思っていることは、すべて あなたから生ずるのである。あなたは何も要求されず、だれもあなたに語りかけず、すべては静かである〉と」(ブーバー 1979:189)。
★以下は「医療倫理学」に続きます
リンク
文献
その他の情報
Copyleft, CC, Mitzub'ixi Quq Chi'j, 1996-2099
++
Copyleft,
CC, Mitzub'ixi Quq Chi'j, 1996-2099